INTRODUCTION
The development of the urogenital system is highly complicated in human beings. Therefore, the congenital anomalies or the variations are higher as compared to those in other systems in the same individual. Some of the anomalies of the kidneys and their vessels are common. Few of them do not even cause clinical symptoms and thus do not require treatment. However, they may predispose to a renal pathology like a vascular insufficiency. A delay in the migration of the kidney into the lumbar region or the persistence of the embryological structures, leads to anomalies [1]. Normally, the kidneys are retroperitoneal and they are located in the lumbar region, with the upper pole of the left kidney at the level of the T11vertebra, whereas the upper pole of the right kidney lies at a lower level, at the level of the T11-T12 intercostal space. The variations in the number, shape, size, position, rotation and the vascularization of the kidneys are of immense importance due to their susceptibilities [2,3]. The kidneys are supplied by a pair of renal arteries which arise from the abdominal aorta, below the origin of the superior mesenteric artery. Developmentally, the human kidneys first lie in the pelvic cavity, with the hilum being directed anteriorly. Gradually, the kidneys ascend with the medial rotation of the hilum and they reach the lumbar region, with their hila being directed antero medially. Normally, as the kidneys ascend from the pelvis, the regional arteries which are close to it provide nutrition. These are the lateral splanchnic branches of the internal and the common iliac arteries and they receive new branches from the abdominal aorta as the kidneys ascend. Later, the inferior branches disappear, as the kidneys reach the lumbar position, with the hilum being rotated medially [4].
In the present study, a unilateral, right renal ectopia with the hilum facing anteriorly and bilateral multiple renal arteries were observed. The renal veins also presented variations with the retro aortic left renal vein, which were observed during the routine dissection of a male cadaver. These observations are of immense importance for interventional radiologists, nephrologists and vascular surgeons.
CASE REPORT
During the routine dissection of a formalin fixed male cadaver who was aged 55 years, in the Department of Anatomy, N.R.I Medical College, Chinnakakani, Guntur, Andhra Pradesh, India, in the year 2006-07, bilateral multiple renal vascular variations with a unilateral right ectopic kidney was noticed. The kidneys with renal vessels were neatly dissected and photographs were taken.
A case of a unilateral right ectopic kidney with bilateral multiple renal vessels was observed, which showed the following:
The Right Kidney: The upper pole of the right kidney was located at the intervertebral disc between the L1-L2 vertebrae, with the hilum facing anteriorly. Thus, it was ectopic in position. It was vascularized by five renal arteries (1-main and 4 accessory renal arteries) and 3 renal veins (1 main and 2 accessory renal veins).
The Right Renal Arteries: [Table/Fig-1] From above downwards, first is the main renal artery and the rest of the 4 are accessory renal arteries. The first renal artery (the RRA -1 or the main renal artery) originated from the aorta, it ran obliquely upwards, crossed by a middle renal vein and entered the hilum. It was above the level of the inferior mesenteric artery.
The right ectopic kidney showing multiple renal arteries
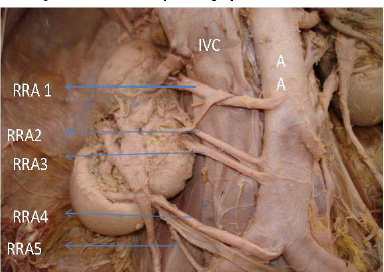
The Second and the Third Renal Arteries: The RRA – 2 and RRA-3- both are accessory renal arteries, direct branches of the aorta and they entered the hilum. At the origin, these were below the level of the inferior mesenteric artery.
The Fourth Renal Artery: (the rra-4 or the accessory renal artery): It originated from the aortic bifurcation, coursed obliquely upwards along with the right inferior renal vein and it entered the hilum of the right kidney by passing behind the ureter.
The Fifth Renal Artery: (the RRA-5 or the accessory renal artery): It originated from the right common iliac artery. It entered the hilum.
The Right Renal Veins: [Table/Fig-2] There were 3 renal veins – the superior, middle, and the inferior renal veins. All the three renal veins drained into the inferior vena cava.
Multiple renal veins. SRV- Superior renal vein, MRV-Middle renal vein, IRV- Inferior renal vein, IVC-Inferior vena cava, AA-Abdominal aorta
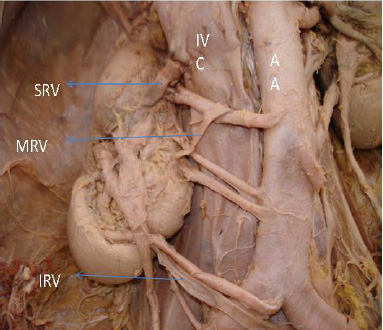
The Superior Renal Vein: (the main renal vein- SRV) From the hilum, it crossed the upper pole obliquely and drained into the inferior vena cava.
Middle Renal Vein: (the MRV) It drained into the inferior vena cava by crossing the main renal artery anteriorly.
Inferior Renal Vein: (the IRV) It followed the course of the 4th renal artery and drained into the inferior vena cava.
The Left Kidney: The upper pole was located at the intervertebral disc between T12 and L1. The hilum as directed antero-medially. It was normal in position.
The Left Renal Arteries: [Table/Fig-3] Two renal arteries vascularized the left kidney.
Indicates left renal vessels: accessory left renal vein which is retro-aortic& accessory renal artery was seen
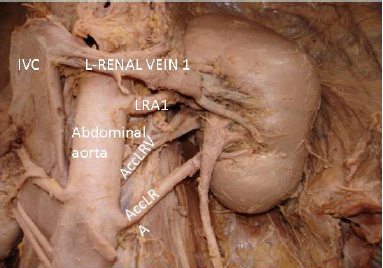
Of the two, one was the main renal artery (LRA-1) and the other was the accessory renal artery (AccLRA). The accessory renal artery was a direct branch from the aorta and it originated at the level of the inferior mesenteric Artery.
The Left Renal Veins: [Table/Fig-3]. These were two in number.
One was the main renal vein (LRV-1) and the other was the accessory renal vein (Acc LRV). The accessory left renal vein extended behind the aorta as the retro-aortic renal vein and it drained into the inferior vena cava.
DISCUSSION
In this part, the variations in the renal arteries, the renal veins and the renal ectopia have been discussed in that order.
The variations in the origin of the renal artery were divided into two groups.
They were: (1). The early division and (2). The extra renal arteries.
The early division consisted of the branching of the main renal arteries into segmental branches, which lay more proximal in terms of their origins.
Extra Renal Arteries (Era) Were Divided into 2 Groups: the hilar (also called as accessory) and the polar (also called as aberrant) arteries. The hilar arteries entered the kidneys from the hilus with the main renal artery, whereas the polar arteries entered the kidneys directly from the capsule outside the hilus [5].
In the present case, bilateral multiple renal vessels were observed, in which the right kidney presented 5 renal arteries and the left kidney presented 2 renal arteries [Table/Fig-1& 2]. The frequencies of the multiple renal arteries ranged from 9%-76%, with an average occurrence rate of 28–30%, depending on the gender and the race [1,2]. Thus, the occurrence of the 4 renal arteries was about one in 266 cases which were studied (0.4%) [6]. A study was conducted on the kidneys of donors, in which there were multiple renal arteries which were found to be 31% altogether; they were bilateral in 10.2% and unilateral in 20.8% cases [7]. During the ascent of the kidneys from the pelvis to the lumbar region, the blood supply was from the common iliac, the abdominal aorta near the bifurcation and gradually, from the abdominal aorta at the level of the first lumbar vertebra. As the kidneys ascended, the caudal branches disappeared and the cranial ones persisted. According to the observations which were made by Felix, there are nine pairs of arteries which supply the mesonephros, metanephros, gonads and the adrenal glands. These nine pairs have been divided into the cranial (the 1st and the 2nd pair), middle (the 3rd to the 5th pair) and the caudal (the 6th to the 9th pair) groups. The renal arteries develop from a single pair, from the middle group. The remaining arteries of the middle group, if they persist; give rise to the accessory or the aberrant renal arteries. Thus, the variations in the number of renal arteries are due to the persistence of the arteries which arise from the aorta, the common iliac arteries, the internal iliac arteries and the lateral splanchnic branches. These arteries persist due to the non ascent or the incomplete ascent of the kidneys to the normal position [8–10].
In an ectopic kidney, the blood vascular pattern is retained at whichever level the kidney ascension stops [9].
The procedure of laparoscopic donor nephrectomy has gained popularity over the years and research studies have clearly spelt out the difficulty in carrying out such procedures in the presence of multiple renal arteries [11].
In the present study, it was observed that there were triple right renal veins, in which one was the main renal vein (SRV) and the remaining (MRV and IRV) were accessory [Table/Fig-2]. On the left side, there were 2 renal veins [Table/Fig-3], in which one was the main renal vein (LRV 1) and the other was the accessory retro aortic left renal vein (ACCLRV). According to the development of the abdominal veins, there are 3 pairs of veins which are called the post cardinal veins, the sub cardinal veins and the supra cardinal veins, which along with their communications, give rise to the inferior vena cava and its tributaries. These veins remain for a short duration and along with their transverse anastomosis near the developing kidneys, form a renal anastomosis or a renal collar. Any mishap in the development of the veins in the region of the developing kidneys, leads to the accessory renal veins and the persistence of the posterior part of the renal collar gives rise to the retro aortic renal vein [12].
The present observation also showed that the upper pole of the right kidney was at the intervertebral disc between L1-L2, with the hilum facing anteriorly, instead of it facing anteromedially and it failing to reach the T11-T12 intercostal spaces, leading to a right ectopic kidney [Table/Fig-1]. The cases of ectopic kidneys and unilateral or bilateral anomalous renal vessels have been reported in the literature regularly, with a frequency of 1:500 to 1:110. There are various levels at which the kidneys can stop ascending or they may ascend at a higher level than the normal. A single kidney was observed to be 1:1000, a single pelvic kidney was observed to be one in 22,000, a unilateral pelvic kidney with one normal kidney was observed to be 1:3000, a crossed renal ectopia was observed to be 1:7000 and a migration to the thoracic region, leading to a thoracic kidney was observed to be 1:13,000. 3 Most of the individuals with ectopic kidneys are asymptomatic. They are identified during routine or unrelated investigations. Such cases are also associated with multiple renal vessels [2].
Among the renal ectopia, the pelvic kidney was very rare and was 1 in 2500 live births, with a common occurrence on the left side [13]. The kidneys can descend due to nephroptosis, but this can be differentiated from a congenital ectopic kidney by observing the length of the ureter. An ectopic kidney may present with pain, hydronephrosis, pyelonephritis, fistulae between the gut and the kidney, renal calculi or obstetric problems in females [3].
The probable reasons for the ascent of the kidney are diminution of the body curvature and the growth of the body in the lumbar and the sacral regions. The ectopic position of the kidney is due to the arrest of its ascent during its development. There is a strong correlation between the renal ascension and its vascularization. Any anomaly in the development of the renal arteries may delay the kidney migration, leading to ectopia and vice versa. In case of the renal veins, the variations are associated with the development of the inferior vena cava [13,14].
The knowledge of the renal vascular variation is of extreme importance for the surgeons who approach the kidneys from the retroperitoneal route for renal transplants [12]. The variations in the positions of the kidneys and the number of renal vessels and their positions are detected by a minimally invasive procedure, CT or CT angiography, to prevent damage to the renal vessels during renal or abdominal vascular surgeries. This helps in making an accurate diagnosis and in planning the right treatment [15].
CONCLUSION
Variations in the renal vasculature are common in the population and they are of importance not only for the surgeons, but also for the radiologists, especially in the interventional radiological approaches and during post-surgical complications. In such conditions, the risk of the kidney loss is higher in the cases with the multiple renal arteries as compared to the that in those with kidneys which have a single renal artery, as each additional artery may be supplying a segment of the kidney. These anomalies which are associated with renal ectopia are attributed to the developmental mishaps in the formation of the kidney and its vasculature. In the present study, there were 5 renal arteries on the right side and two arteries on the left side. The renal veins were three on the right side and there were 2 on the left side, with a retro aortic left renal vein. These were associated with a right renal ectopia. Therefore, a sound knowledge of the multiple renal vessel variations and the renal ectopia are important for the urologists and the radiologists during the performance of renal surgeries in kidney donors and in kidney transplantations, especially in the laparoscopic surgeries which are done on kidneys. These variations should also be kept in mind when renal vessel surgeries are performed by vascular surgeons for renal artery stenosis or aneurisms.
[1]. Zagyapan Ragiba, Pelin Can, Kürkçüoglu Ayla, A retrospective study on multiple renal arteries in Turkish populationAnatomy (International Journal of Experimental and Clinical Anatomy) 2009 3:35-39.Available at: www.anatomy.org.tr.Accessed February 25, 2012 [Google Scholar]
[2]. Zahoi Delia Elena, Miclaus G, Aurora Alexa, Dorina Sztika, Agneta Maria Pusztai, Mioara Farca Ureche, Ectopic kidney with malrotation and bilateral multiple arteries diagnosed using CT angiographyRJME 2010 51(3):589www.ncbi.n/m.nih.gov/pubmed; www.rjme.ro/RJME [Google Scholar]
[3]. Beslsare SM, Chimmalgi M, Vaidya SA, Sant SM, Ectopic kidney and associated anomalies -A case reportJournal of Anatomical Society of India 2002 51(2):236-38. [Google Scholar]
[4]. Susan Standring, Gray’s Anatomy - Anatomical Basis of clinical Practice 2005 39thElsevier Churchill Livingstone, Toronto: Elsevier Ltd.:1274 [Google Scholar]
[5]. Ugur Özkan, Levent Oguzkurt, Fahri Tercan, Osman Kýzýlkýlýç, Zafer Koç, Nihal Koca, Renal artery origins and variations: angiographic evaluation of 855 consecutive patients-Diagnostic and Interventional Radiology 2006 12(4):183-86.www.dirjournal.org [Google Scholar]
[6]. Gupta Anupma, Kumar Parveen, Soni Gargi, Shukla Lovesh, Double precaval right renal artery associated with multiple left renal arteries – A Case ReportIJAV 2011 4:137-38. [Google Scholar]
[7]. Coen LD, Raftery AT, Anatomical variations of the renal arteries and renal transplantationClinical Anatomy 1992 5(6):425-32. [Google Scholar]
[8]. Gurses Ilke Ali, Kale Aysin, Gayretli Ozcan, Bayraktar Bulent, Usta Ahmet, Kayaalp Mahmut Enes, Bilateral variations of renal and testicular arteriesIJAV 2009 2:45-47. [Google Scholar]
[9]. Moore Keith L., Persaud TVN, The Developing Human, Clinically oriented Embryology 2003 7thTorontoW.B.Saunders Company:292-96. [Google Scholar]
[10]. Madhyastha Sampath, Suresh R, Rao Ramesh, Multiple renal variations of renal vessels and ureter. A Case ReportIndian journal of urology 2001 17(2):164-65. [Google Scholar]
[11]. Su Li Ming, Ratner LE, Robert AM, Jarrett TW, Trock BJ, Vladimir Sinkov, Laparoscopic live donor nephrectomy - Trends in donor and recipient morbidity following 381 consecutive casesAnn. Surg. 2004. August 240(2):358-63. [Google Scholar]
[12]. Fernandes RMP, Conte FHP, Favorito LA, Abidu-Figueiredo M, Babinski MA, Triple Right Renal Vein: An Uncommon VariationInt. J Morphol. 2005 23(3):231-33. [Google Scholar]
[13]. Reddy CK, Syed NA, Satyanarayana N, Phukon MJ, Dutta R, Sunitha P, Left ectopic kidney with non-rotation: A Case ReportNepal Med Coll J. 2010 12(2):123-24. [Google Scholar]
[14]. Govindarajan A, Meenakshisundaram J, Right ectopic kidney with rare vascular variations Right ectopic kidney with rare vascular variationsInternational Journal of Anatomical Variations 2011 4:12-14. [Google Scholar]
[15]. Zahoi DE, Miclaus G, Alexa A, Sztika D, Pusztai AM, Farca Ureche M, Ectopic kidney with malrotation and bilateral multiple arteries diagnosed using CT angiographyRom J Morphol Embryol. 2010 51(3):589-92. [Google Scholar]