HIV and (in) fertility are associated in several ways and they share some common determinants like sexual exposure, contraceptive practices and reproductive tract infections. Each has significant adverse psychological and socio-cultural implications, especially in sub-Saharan Africa and other less developed countries. The predominant poverty compounds the already bad situation, as it is difficult, if not impossible, to access several treatment options for both HIV and infertility. Living with HIV/AIDS does not remove the desire to have children and it should not exclude a couple from the reproductive technology and the fertility treatments.
Despite the reportedly high tubal infertility rates and the prevalence of the HIV infection in sub-Saharan Africa, there is paucity of literature with regards to these two pathologies. Hysterosalpingography still remains the most accessible and affordable means of evaluating the fallopian tubes in Nigeria and in other less developed countries. This study evaluated and compared the tubal findings in HIV positive and negative individuals who presented for the hysterosalpingography assessment due to infertility.
MATERIALS AND METHODS
A year prospective study was conducted at a diagnostic centre at a cosmopolitan town of Lagos in 2011. All the patients of hysterosalpingography were counselled by a consultant and those who agreed to participate in the study were given a pre test counselling. The socio-demographic data and the gynaecological history were then obtained by using a structured questionnaire. The post test counselling and/or referral was done as found appropriate.
The hysterosalpingograpy was done and reported by the radiologist. The patients were allowed to opt out of the study at any stage. The statistical analysis was done by using SPSS.
RESULTS
[Table/Fig-1,2, 3,& 4]. A total of 5250 hysterosalpingographic studies were done at the centre in 2011, but only two thousand and two hundred women consented to participate in this study. The highest number of patients, one thousand and two hundred patients (54.5%) were in the age group of 31-40 years; and the least number of patients in the age categories of less than 20 years and greater than 57 years, were 2 (0.1%) and 3 (0.1%) respectively.
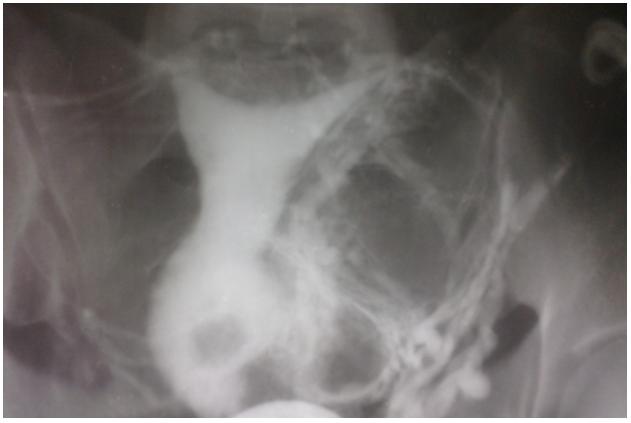
Hsg Showing Normal Uterus And Fallopian Tubes
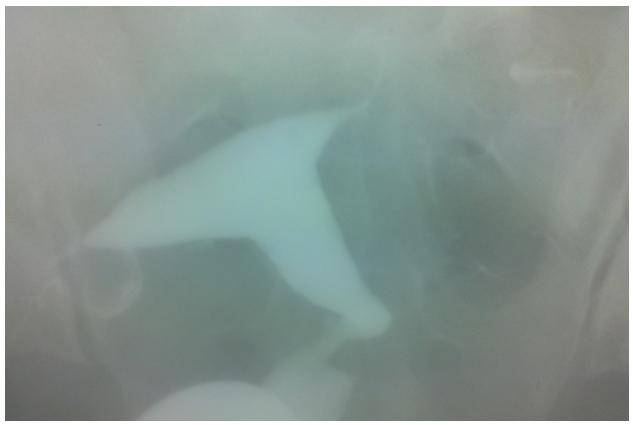
Hsg Showing an Abnormally Shaped(Spindle) and Small Sized Uterine Cavity Due to Synechiae; Both Fallopian Tubes are Normal and Patent

Hsg Showing Bilateral Distal Hydrosalpinges With Blockage

Hsg Showing Bulky Cervix With A Filling Defect Within It-Cervical Fibroid
Most of the patients were nulliparous, 1690 (76.8%) while 510 patients (23.2%) had a parity of one and above. 45% of the patients had primary infertility, while 55% had secondary infertility.
There was a positive history of induced abortions in 620 patients, 620 (28.2%). Four hundred and ninety one patients, 491 (22.3%) were positive for HIV, while one thousand, seven hundred and nine (77.7%) tested negative. About half (48.9%) of the HIV positive patients had a past history of induced abortions, while 22.2% of the HIV negative patients gave a similar history.
Uterine synechiae [Table/Fig-3] was seen in 26.5% and 9.6% of the HIV positive and negative patients respectively. A total of four thousand and four hundred fallopian tubes were evaluated (two thousand and two hundred patients); 48% (469, four hundred and sixty nine) of the nine hundred and eighty two (982) fallopian tubes in the HIV positive patients were normal, while 52%, ( 513, five hundred and thirteen) had abnormalities which ranged from distal occlusion ( a total of 137, 68 for the right and 69 for the left respectively); to proximal occlusion (a total of 137, 62 for the right and 75 for both respectively); to hydrosalpinx ( a total of 239; 120 and 119 for the right and left respectively).
In the HIV negative patients, a total number of 2,529 tubes (74%) were normal [Table/Fig-1], while the remaining 26% were abnormal, with abnormalities which ranged from distal occlusion (a total of 338, 139 and 199 for the right and left respectively); to hydrosalpinx [Table/Fig-3] (a total of 265, 111 and 154 for the right and left respectively).
DISCUSSION
Infertility is affecting a large number of couples in sub-Saharan Africa, with a prevalence of up to 29% in certain regions [1]. It has significant consequences in this region where a woman’s status and acceptance are solely dependent on her motherhood. The prevalence of poverty makes it impossible to afford the sparsely available advanced reproductive technologies and it compounds the woes of an infertile couple (or a woman).
The prevalence of the HIV infection in this region of Africa has been reported to be 23.3 million, which translates to 70% of the overall infections world wide [2].
Both these conditions exert adverse psychological and socio-cultural effects on the affected ones. With the advent of the Highly Active Anti-Retroviral therapy, and the ability to reconstitute the immune system and to keep the viral loads at undetected levels, the HIV positive individuals can live a healthy and reproductive life for years to decades after their diagnosis [3,4].
Also, it has been reported that it is unethical to withhold fertility services to these individuals or couples [5]. Despite the significance of these two pathologies, there is a scarcity of literature on the findings on hysterosalpingography in the patients with HIV.
A majority of the patients were between 31-40 years of age (54.5%), followed by the age group of 21-40 years (39.2%), while the least number of patients were found in the age groups of less than twenty years and greater than fifty years. 76.8% of the patients were nulliparous, while 55% presented with secondary infertility. Some of these findings are similar to previous reports which were made by Adesiyan Adesiyun et al., [6] who recorded the highest number of patients for HSG in the 30 to 39 years age bracket; though secondary infertility was also more common in their study, it was responsible for 84.1% patients as compared to 55% patients in this study. Similar studies have also reported the highest number of patients to be in the age group of 26-30 years, followed by the 31-35 years age group [7,8].
48.9% of the HIV positive patients had a previous history of induced abortions, while only 22.2% of the HIV negative patients gave a past history induced abortions. In the study which was reported by Adesiyun et al., [6], 49.3% of the patients had induced abortions in the past. The high rate of induced abortions is a direct reflection of the high rate of unprotected sex and multiple sexual partners in our environment, which are both predisposing factors to the HIV infection.
These induced abortions would have contributed significantly to the tubal factors in the infertile woman, due to the fact that the procedures were often performed by non qualified personnel because of their illegality [9]. Although, Ikechebelu et al., [10] reported only multiple sexual partners and previous sexually transmitted infections as statistically significant, the sexual behaviours in the infertile HIV positive women with blood transfusions and induced abortions were not statistically significant in the infertile HIV positive and negative women [10].
The tubal abnormalities were commoner in the HIV positive women (52% of the patients) as compared to the 26% tubal abnormality rate in the HIV negative patients.
Several authors have reported a high incidence of tubal abnormalities, generally in the infertile sub-Saharan African women and specifically in the HIV positive women [6,11–13].
In our study, all types of tubal abnormalities were commoner in the HIV positive than in the HIV negative women, with hydrosalpinx being responsible for the highest pathology.
There were temporal and complex relationships between tubal infertility, sexually transmitted infections, HIV, high risk sexual behaviours and induced abortions.
A high risk sexual behaviour often leads to pelvic inflammatory diseases which are either caused by sexually transmitted infections ( other than HIV) or by endogenous ( mostly vaginal) organisms and to illegally induced abortions which are done by quacks, with post abortal sepsis as the sequelae.
These often lead to a tubal damage and or the HIV infection. The ulcerative and non ulcerative sexually transmitted infections can act as co-factors in the sexual transmission of HIV [14,15], while HIV increases the susceptibility to other STIs and adversely influences their natural history.
HIV is also reported to reduce the fertility in women and men due to co-infection with the STIs, with resultant tubal factor infertility; weight loss related anovulation/amenorrhoea, male hypogonadism and impaired spermatogenesis [16].
Also, infertility is suggested to be a risk factor for the HIV acquisition, since the couples with a fertility problem are likely to face extramarital relationships, polygamous unions and divorce, which are all known risk factors for the HIV infection [10,17].
Ikechebelu et al., [10] recorded an average of 5 sexual partners in 86.2% of the HIV positive infertile women who were evaluated with laparoscopy, as compared to an average of two sexual partners in 38% of their HIV negative counterparts.
High HIV positivity rates of 22.3% and 36.6% were seen amongst the entire studied population and among the patients with tubal pathologies respectively. Similarly, high rates of HIV positivity had been reported amongst the infertile women. The HIV infection was found to be threefold higher among the infertile women than among their fertile controls [18], five fold higher among the women who had undergone a laparoscopy evaluation for infertility than among pregnant women 10 and three fold higher in the women with tubal infertility then among the general population.
CONCLUSIONS
In conclusion, this large sample size study has reported a high prevalence rate of HIV amongst the infertile women with a statistically significant history of induced abortions and tubal pathologies as compared to that among the HIV negative women.
There is a need to keep researching and to proffer a solution and treatment to infertility, considering the socio-cultural, psychological and the stigmatization effects on the infertile and or HIV positive women in our environment.