Irrespective of the vast progress which has been made in the identification of the aetiology and the treatment of cardiovascular diseases, people are still becoming prey to these diseases in developing countries like India. It was observed by the World Health Organization, that by the year 2020, coronary heart disease and stroke would occupy the first and fourth places as the leading causes of disability and mortality. It was estimated that the incidence of coronary vascular diseases would increase from 2.90 crore in 2002 to about 6.40 crore in 2015. Tobacco is patho-genetically a cholesterol dependent risk factor and it acts synergistically with other risk factors for the causation of coronary heart disease. Thus, a strong synergistic interaction exists between hyper cholesterolaemia and tobacco consumption in the genesis of coronary heart disease. The aetiology of coronary heart disease is multifactorial, among which there are non preventable and preventable risk factors. The possible mechanisms of tobacco consumption in the pathogenesis of coronary heart disease are:
Among the components of the gaseous phase are carbon monoxide, carbon dioxide, nitric oxide, nitrogen dioxide, dinitro trioside, ammonia, hydrogen cyanide, volatile sulphur containing compounds, volatile aldehydes (formaldehyde, acetaldehyde and acrolein) alcohols and ketones. Tobacco smoke also contains various types of nitrosamines.
All these nitrosamines are formed from various alkaloids which are present in tobacco, i.e., nictotine, nornicotine, anabasine and anatabine by nitrozation. These nitrosamines are potential carcinogenic substances and they are capable of alkylating the DNA. The actual content of nicotine in tobacco varies between 1-2%.
MATERIALS AND METHODS
This study was conducted on 3 groups of male subjects who were 25-35 years of age and who weighed 50-70 kgs. Each group contained 25 subjects. The subjects with diabetes, hypertension, obesity, renal diseases lipid metabolism disorders and coronary diseases were excluded.
Group-I: Non smokers and Non chewers: These were taken as the control group.
Group-II: Smokers and Non chewers: These were the individuals who had been smoking 11 to 20 cigarettes for the past 10 years.
Group-III: Chewers and Non Smokers: These were the individuals who had been consuming tobacco in the form of chewing 3 to 4 leaves per day for the past 10 years. The subjects were instructed to fast overnight. Their heart rates and blood pressures were recorded while they were at rest.
The blood samples are collected after an overnight fasting for about 14 hours. 5 ml. of whole blood was collected from each subject and the serum was separated. The serum lipid profiles were studied and the lipid levels were calculated. The readings which were obtained are shown in the tables. Estimation of the total cholesterol by the Zak method [1]. Estimation of Triglycerides by the HANTZSCH condensation reaction, Estimation Of HDL Cholesterol. LDL, VLDL and chylomicrons were precipitated by polyanions in the presence of metal ions (Phosphotung-state/Mg) to leave HDL in the solution. The complete lipid profile measures the serum total cholesterol, HDL and the triglycerides. LDL and VLDL were calculated by using Freidewald’s formula, provided the triglyceride levels were below 400mg. per dl.
VLDL cholesterol= trigly-ceride/5
LDL cholesterol=Total
cholesterol – (VLDL
Cholesterol + HDL
Cholesterol)
RESULTS
The mean serum total cholesterol, VLDL, LDL and the serum triglyceride levels in the subjects of Group III and Group II showed a significant increase than the levels in the Group I subjects [Table/Fig-1,2,3,4,5 & 6]. The mean serum HDL levels in the subjects of Group III and Group II showed a significant decrease than the levels in the Group I subjects [Table/Fig-7].
Comparison of Mean Serum Lipoprotein Values in Non Smokers Non Chewers and Smokers Non Chewers
| Smokers Non Chewers | Non Smokers Non Chewers | P value |
| Heart Rate | 78.96 | 70.40 | <0.01 |
| SBP | 125.40 | 113.70 | <0.01 |
| DBP | 82.80 | 75.60 | <0.001 |
| LDL | 113.80 | 84.52 | <0.001 |
| Triglycerides | 117.60 | 92.20 | <0.001 |
| HDL | 54.92 | 60.88 | <0.01 |
| VLDL | 23.52 | 18.44 | <0.01 |
| T. Cholesterol | 191.60 | 163.80 | <0.001 |
Comparison of Mean Serum Lipoprotein Values in Non Smokers Non Chewers and Non Smokers Chewers
| Smokers Non Chewers | Non Smokers Non Chewers | P value |
| Heart Rate | 74.88 | 70.40 | <0.01 |
| SBP | 127.70 | 1170 | <0.01 |
| DBP | 77.36 | 75.60 | >0.01 |
| LDL | 114.40 | 84.52 | <0.001 |
| Triglycerides | 113.60 | 92.20 | <0.001 |
| HDL | 53.68 | 60.88 | <0.01 |
| VLDL | 22.52 | 18.44 | <0.01 |
| T. Cholesterol | 190.50 | 163.80 | <0.001 |
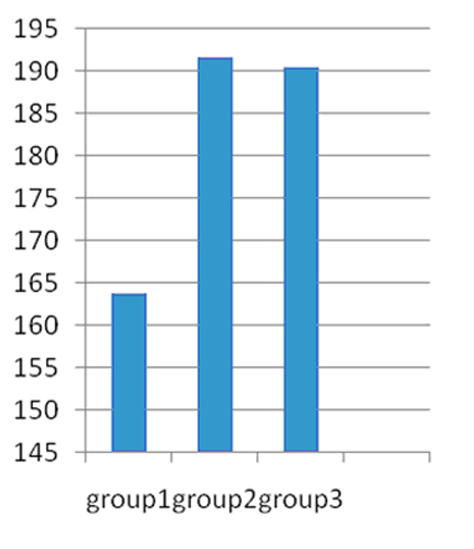
Comparison of Mean Serum total Cholesterol Values of Non Smokers Non Chewers (Group-1), Smokers Non Chewers (Group-2) and Chewers Non Smokers (Group-3)
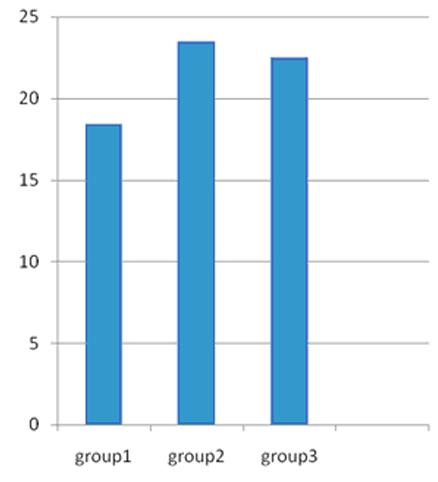
Comparison of Mean Serum Vldl Cholesterol Values of Non Smokers Non Chewers (Group-1), Smokers Non Chewers (Group-2) and Chewers Non Smokers (Group-3)
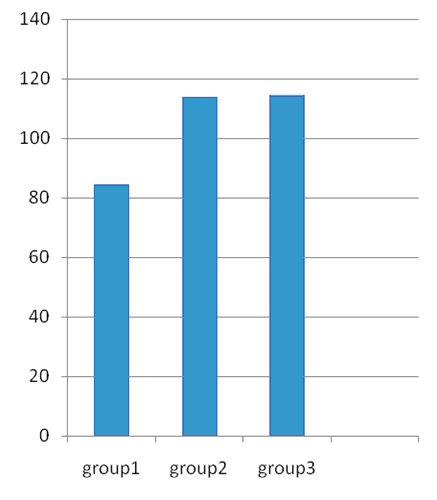
Comparison Of Mean Serum Ldl Cholesterol Values Of Non Smokers Non Chewers (Group-1), Smokers Non Chewers (Gro-Up-2) And Chewers Non Smokers (Group-3)
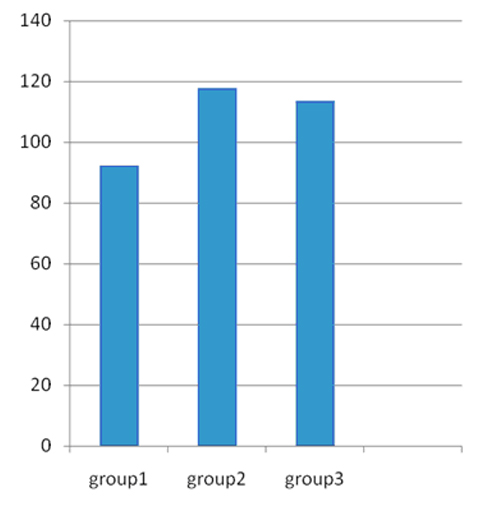
Comparison Of Mean Serum Triglycerides Values Of Non Smokers Non Chewers (Group-1), Smokers Non Chewers (Group-2) And Chewers Non Smokers (Group-3)
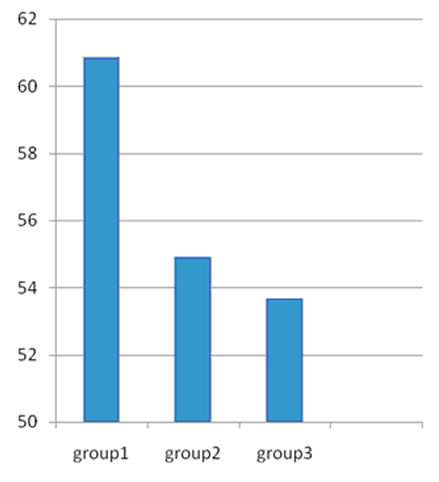
Comparison Of Mean Serum Hdl Cholesterol Values Of Non Smokers Non Chewers (Group-1), Smokers Non Chewers (Group-2) And Chewers Non Smokers (Group-3)
DISCUSSION
Tobacco has been recognized as a major risk factor for the development of ischaemic heart disease and it may lead to alteration of the normal plasma lipoprotein pattern [2].
It has long been established that tobacco contains nicotine and that it has a considerable influence on the increasing levels of lipids in the blood.
Batic-mujanovic O[3] et al., observed decreased levels of HDL cholesterol and increased levels of total cholesterol, LDL cholesterol and triglycerides in smokers as compared to those in non smokers. The same observation was found in our study also.
Neki NS [4], during his study on the association between the lipid profile and chronic smoking, found very low levels of HDL, with an increase in the levels of TC, LDL, VLDC and TG in smokers. This was in agreement with the findings of our study.
Krishnaswami S, et al., [5] studied the association between cigarette smoking and coronary artery disease. They found that the prevalence of CAD was higher among smokers than among nonsmokers, which is in agreement with the results of our study.
In the present study, it was found that cigarette smoking was associated with depressed levels of HDL, which was concurrent with the observation of Stanford BA, et al., [6].
Nnno Dim John Kennedy [7] observed increased levels of total cholesterol, triglycerides and LDL-C, which was in accordance with the findings of our study. Garrison et al., [8] measured the HDL cholesterol levels in smokers and they noticed a negative association between the number of cigarettes which were consumed and the HDL levels, which was in concurrence with the findings of our study.
Our study revealed that there was an inverse correlation between the HDL levels and the tobacco users, which was also found in the study which was done by Yadav BK, Bade AR, Singh J and Jha B [9] serum total cholesterol, tryglicerides, LDL Cholesterol levels and decreased levels of HDL Cholesterol observed by Guedes DP et al., [10] is in accordance with our study. Saengdith P [11] studied the serum lipid levels and found an increase in the levels of the triglycerides, which was in concurrence with the findings of the present study.
Khurana M et al., [12] compared the lipid profile of smokers and tobacco chewers and observed a rise in the levels of TG, LDL and VLDL with a decrease in the HDL level in smokers and chewers, which was in concurrence with the results of the present study. The high triglyceride value which was found in the smokers as compared to that in the non-smokers in our study, was in concurrence with the findings of the study of Waheeb DM [13].
The total cholesterol, LDL-C and the triglyceride levels were increased in our study, which coincided with the results of the study of Gosset LK, Johnson HM, Piper ME, et al., [14].
Cigarette smoking increases the cholesterol, LDL-C and the triglyceride levels and it decreases the HDL-C levels, as was observed in the present study, which was in agreement with the findings of Demosthenes B et al., [15].
Arslan E et al., [16] observed increased LDL, VLDL and triglyceride levels and decreased HDL levels, which was consistent with the findings of the present study. Loic de Parscau et al., [17] studied the plasma cholesterol levels in smokers and found decreased HDL levels and increased LDL levels, which was in agreement with the findings of our study.
In our study, an increase in the levels of TG, LDL and VLDL was observed with a decrease in the HDL level in smokers, which was in concurrence with the findings of the study of Campbell SC et al., [18].
Svenchrenger [19] found low HDL-C levels in smokers than in the non smokers, which was consistent with the findings of the present study. Ritesh Gupta [20] observed increased cholesterol and triglyceride levels and decreased levels of HDL cholesterol, which were in agreement with the findings of our study.
Hajmouhamed D et al., [21] observed decreased levels of HDL cholesterol and increased levels of total cholesterol, LDL cholesterol and triglycerides in Tunisian smokers as compared to the levels in non smokers. The same observation was found in our study also.
SUMMARY
As the saying goes, ‘To err is human’; it only speaks of human weaknesses or the human tendency to commit mistakes. Because, the statistics do not accept this as in any particular study of any error. This is only a small percentage of error; besides, humans also learn the hard way. Hence, in spite of the vast knowledge experienced warning day by day, yet the incidence of smoking is growing along with the population. But in the educated sector, the incidence is receding. The statistics does clearly show us the impending danger on the smoking population of the developing countries.
Smoking, or if we say more carefully, tobacco, has a very bad influence on the total health system of the human beings, not only effecting the arteries or the lung but almost all the functional systems of the body, from cell to cell.
The nicotine in tobacco causes a decrease in the HDL cholesterol level (good cholesterol) with an increase in the LDL cholesterol level (bad cholesterol) and also an increase in the VLDL cholesterol level, with an accumulation of lipids in the arterial wall. This is responsible for the greater risk of developing atherosclerosis in the tobacco users than in the non-tobacco users.
Once again, let us remember that old is gold; that prevention is better than cure. This has a very applicable role as far as smoking is concerned.