The Neurobehavioural Evaluation in Schizophrenics: A Comparative Study
Kamini Ramdas Ilamkar1
1 Assistant Professor, Department of Physiology, Government Medical College, Nagpur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kamini Ramdas Ilamkar, 9, Parth Apartment, S.E. Railway Colony-2, Telecom Nagar, Nagpur-440022, Mahrastra, India.
Phone: 9890597505
E-mail: Kamini_ilamkar@yahoo.co.in
Background: The simple reaction time task assesses the ability of the subject to respond to an external cue and to retrieve a reward. The reaction time provides an indirect index of the processing capability of the central nervous system and a simple means to the determined sensory and the motor performances, which is a neurobehavioural evaluation. A general slowness in the latency in the reaction time tasks and a disengagement deficit in the visual and the hearing oriented tasks were seen in schizophrenics.
Aims: In order to clarify the feature of the attention disorders in schizophrenia, a simple reaction time task was given to schizophrenics.
Methods and Materials: Schizophrenics (34 males and 20 females, n=54) and healthy controls (40 males and 21 females, n=61) with a mean age of 35±7, who were individually matched for gender and age, were included in the study, by using a response analyser to evaluate the reaction time.
Statistical analysis: The performances were expressed in mean ± standard deviation of the reaction time by using the unpaired ‘t’ test.
Results and Conclusions: The schizophrenic patients performed poorer than the healthy controls, which indicated a difficulty in sustaining attention and this was statistically very highly significant (p<0.000). The results suggested that the schizophrenics showed inattentiveness in the clinical settings and an emotional disturbance in interpersonal situations. The increased reaction time as compared to that in healthy controls, might be due to the impairment of the psychomotor poverty, disorganization and reality distortion which were associated with the deficits in the cortical neurological functions, such as planning, coordination and sequencing of the motor acts, which showed a greater involvement of the frontal lobe and temporal lobe dysfunction.
Schizophrenics, Slowness in latency, Attention disorder, Fronto-temporal lobes dysfunction, Simple reaction time
INTRODUCTION
Simple Reaction Time is the time interval between the onset of a stimulus and the initiation of aresponse under the condition that the subject has been instructed to respond as rapidly as possible [1]. A reaction time provides an indirect index of the processing capability of the central nervous system and a simple means of determining the sensorimotor performances, which is a neurobehavioural evaluation. Simple reaction Time is considered as a measure of the perceptual, motor and the psychomotor speed [2]. The sensorimotor ability and coordination requires the brain to process and synchronize the function of the interrelated muscles. Alterations in the functions such as motor coordination, muscle strength, and motivation serve as the indicators of the gross alterations in the central nervous system. Such alterations need to be assessed and taken into account when any behavioural procedure is planned; in some cases, the results may preclude the specific cognitive tests. The tasks in this module focus on the overall gross motor function, the sensorimotor integration, and the exploration [3]. Attentional deficits have been seen as a fundamental feature of the schizophrenic psychopathology since Bleuler, a scientist, first described these 80 years ago. However, the impaired performance which is frequently observed when schizophrenics perform attentional tasks, could also reflect deficits in the motivation or the organization of the motor activity [4]. In schizophrenia, there is disturbance in a cortical striatal thalamic circuit, which results in deficits in filtering and attentional behaviour schizophrenic patients pay too much attention to concrete stimulus characteristics. As a result, they have more difficulty in developing an automatic and a fast reaction to varying stimuli. This leads to problems when they have to perform on information tasks.
AIMS & OBJECTIVES
This study was designed to evaluate the effect of the reaction time on schizophrenics. The Simple Reaction Time was measured in both schizophrenics and healthy controls and this was compared their reaction times [Mean±SD] to reach any statistical difference.
MATERIALS AND METHODS
This study was conducted in the Department of Physiology, in association with the Department of Psychiatry, Government Medical College and Hospital Nagpur, with due permission of the ethical committee and Head of the Department of Medicine, under whom the Psychiatry Department is working. The Simple Reaction Time was measured in both schizophrenics and controls after taking the informed consents of all of them and the reaction time was noted in the presence of their relatives . According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria, newly diagnosed schizophrenics (34 males and 20 females, n=54) and from the random population, healthy controls (40 males and 21 females, n=61) with a mean age 35±7, who were individually matched for gender and age were included in this study, by using a response analyser to evaluate the reaction time.
The inclusion criteria for schizophrenics included:
Newly diagnosed schizophrenics who gave their informed consents and who were not on any treatment.
Any psychiatric illness or any other central nervous system disorders that could interfere with the memory and the psychomotor functions, except schizophrenia.
Normal hearing and vision.
The exclusion criteria for schizophrenics included:
The schizophrenics who were unable to cooperate or to understand the instructions.
The inclusion criteria for the controls included:
Normal hearing and vision.
The exclusion criteria for the controls included:
A psychiatric disorder or a first degree relative with such a history.
Measurement of the Reaction Time
The auditory and the visual reaction times of all the subjects in the present study were measured by using a reaction time instrument [a response analyzer] by the Yantrashilpa System, Pune, in a quiet room with good visibility conditions. The subjects were asked to sit comfortably on chairs in front of the table on which the response analyzer was placed. They were then explained about the details and the procedure of the test. All the subjects in the study were right handed and they responded with their right hands.
For recording the auditory reaction time, an audio mode was switched on, the required time interval for applying the stimulus was adjusted and then, the sound was set at a low frequency or a high frequency as required. The display was reset to zero by using a reset switch. The subjects were instructed to respond as soon as he/she heard the sound, by pressing the response key with the index finger already on it [5]. The sound stimulus was applied from the side and the subjects responded by pressing the response key. An auto display on the analyzer indicated the reaction time of the individual to the auditory stimulus. Sufficient trials were given for a proper understanding and to alleviate any fear or apprehensions, pre-performance the education, trials and training. Three readings for a low frequency sound were recorded and then, the average of the three readings was considered as the auditory reaction time for a low frequency sound [6]. The same procedure was then applied for a high frequency sound. Thus, the auditory reaction time was recorded for a low frequency sound and a high frequency sound separately.
For recording the visual reaction time, the visual mode was switched on. Then, the required colour light (i.e. red or green) was set on the visual stimulus box. The display was set to zero by using a reset switch. The subjects were instructed to respond as soon as he/she saw the glow, by pressing the response key with the index finger already on it [5]. The visual stimulus was applied from the front side and then the subjects responded by pressing the response key. The auto-display on the analyzer indicated the reaction time of the individual to the visual stimulus e.g. the red coloured light. Three readings were taken and their average was considered as the visual reaction time for the red coloured light [6]. The same procedure was applied for the green light. Thus, the visual reaction times were recorded for the red and green lights separately.
OBSERVATIONS AND RESULTS
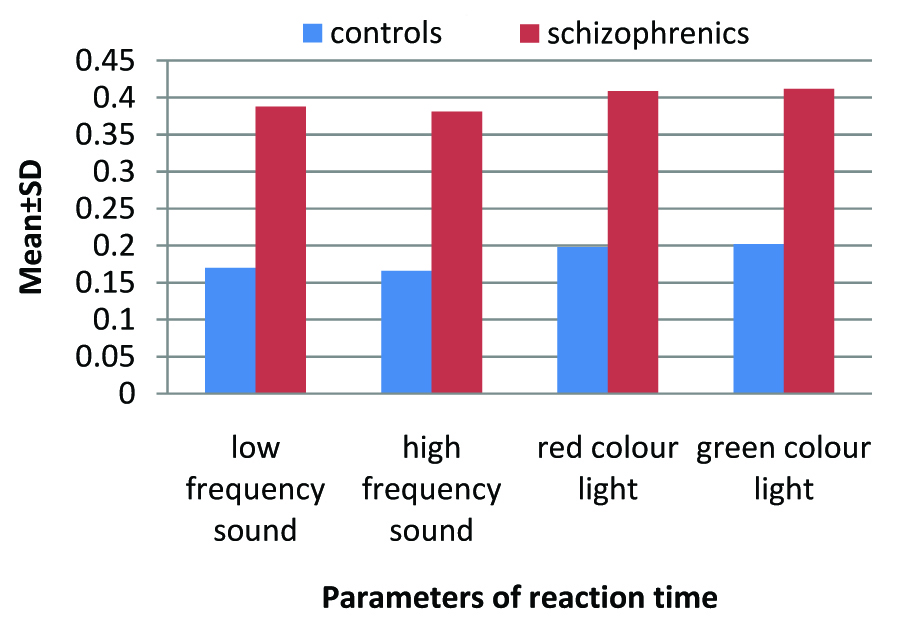
The reaction time was measured by using the following parameters: For the auditory reaction time, a low frequency sound and a high frequency sound were included and for the visual reaction time, a red coloured light and a green coloured light were included [Table/Fig-1 & 2].
Showing that mean values with standard deviation of schizophrenics arehigher than those of controls and was statistically very highly significant.
| Parameters | Controls Mean±Sd) | Schizophrenics (Mean±Sd) | P value |
| Auditory reaction time (secs) | Low frequency sound | 0.170±0.011 | 0.388±0.187 | p=0.0000 |
| High frequency sound | 0.166±0.007 | 0.381±0.187 | p=0.0000 |
| Visual reaction time (secs) | Red colour light | 0.198±0.014 | 0.409±0.186 | p=0.0000 |
| Green colour light | 0.202±0.013 | 0.412±0.185 | p=0.0000 |
Showing comparison and analysis between Controls and Schizophrenics for reaction time
DISSCUSION
Marked deficits in the attention in schizophrenics suggested a reduction in the processing capacity or a temporary disruption of the automatic as well as the attention-demanding processes [7–9].The significant impairment in the stimulus discrimination [10] and the distractability [11] might be due to deficits in the cortical neurological functions; such as the planning, coordination and the sequencing of the motor acts. These are specifically related to the disorganization and the psychomotor poverty syndromes which strengthen the validity of the three syndrome concept of schizophrenia, thus suggesting a greater involvement of the frontal lobe functions [12,13]. The response-selection was selectively impaired in the first onset in the patients, thus indicating a disconnection between the frontal and the posterior areas [14–18]. The neurological dysfunctions in schizophrenia, which are often referred to as ‘soft neurological signs’, appear to reflect the impairment of the integration of the complex sensory units and the coordination and sequencing of the motor activity [19–22]. There may be disturbances in a central monitor system which may mediate between the external demands (stimulus attention) and the internal aims (willed intention) and connect both with the ongoing behaviour (a coronary discharge or a re-afference copy of the present action) physiologically. The central monitor is implemented as a functional loop between the dorsolateral prefrontal cortex, the anterior cingulated cortex, the supplementary motor area and the basal ganglia [23]. The monoaminergic and the cholinergic systems have independent but complementary roles in the attentional function. These functions which are predominantly under the control of the prefrontal cortex striatum [24], may be involved in schizophrenics and there might also be volume reduction and an altered sulco-gyral pattern of the orbitofrontal cortex in a first-episode schizophrenia [25], thus suggesting an involvement of frontal lobe. Giora (1975) had proposed that the principal dysfunction in schizophrenia was a delay in the temporal processing of verbal information: the possible antecedent of the symptomatology of early schizophrenia is a disturbance in the auditory-verbal modality in information processing [26].
CONCLUSION
Thus, the reaction time is an indirect index of the processing capability of the central nervous system and a simple means for determining the sensory motor association and the performance of an individual i.e. a neurobehavioural evaluation. The quickness of the response to an external stimulus has been a subject of extensive research in clinical medicine, sports medicine and other skilled works e.g. pilot, astronauts, driving etc. In today’s competitive world, individuals can make conscious efforts to improve their reaction time, striving for giving the best performance and as we know, record breaking events in Guinness book. The reaction time may also be employed to determine the effects of the therapy in patients of schizophrenia. It may provide an adjunct to the tests for the psychological functioning and a crucial aid to the diagnosis.
[1]. Teichner WH, Recent studies of simple reaction timePsychol Bull. 1954 51:128-49. [Google Scholar]
[2]. Lofthus GK, Sensory motor performance and limb preferencePercepts Motor Skills 1981 52:688-93. [Google Scholar]
[3]. Neurogenetics and Behavior centerDepartment of Psychological and Brain Sciences 2009 Johns Hopkins University [Google Scholar]
[4]. Nuechterlein KH, Dawson ME, Information processing and attentional functioning in the developmental course of schizophrenic disordersSchizophrenia Bulletin 1984 10(2):161-203. [Google Scholar]
[5]. Misra N, Mahajan KK, Maini BK, Comparative study of visual and auditory reaction time of hands and feet in males and femalesIndian J Physio Pharmacol 1985 29(4):213-18. [Google Scholar]
[6]. Shenvi D, Balasubramanian P, A comparative study of visual and auditory reaction times in males and femalesIndian J Physiol Pharmacol 1994 38(3):229-31. [Google Scholar]
[7]. Baribeau-Braun J, Picton TW, Gosselin JY, Schizophrenia: a neurophysiological evaluation of abnormal information processingScience 1983 4586(219):874-76. [Google Scholar]
[8]. Jones SH, Hemsley DR, Gray JA, Contextual effects on choice reaction time and accuracy in acute and chronic schizophrenics. Impairment in selective attention or in the influence of prior learning?British Journal of Psychiatry 1991 159:415-21. [Google Scholar]
[9]. Davalos DB, Kisley MA, Ross RG, Deficits in auditory and visual temporal perception in schizophreniaCognitive Neuropsychiatry 2002 7(4):273-82. [Google Scholar]
[10]. Birkett P, Sigmundsson T, Sharma T, Toulopoulou T, Griffiths T, Reveley A, Murray R, Reaction time and sustained attention in schizophrenia and its genetic predispositionSchizophrenia Research 2007 1(95):76-85. [Google Scholar]
[11]. Malathi A, Parulkar VG, Dhavale HS, Pinto C, A preliminary study of reaction time in schizophrenicsIndian J Physiol Pharmac 1990 34(1):54-56. [Google Scholar]
[12]. Liddle PF, Schizophrenic syndromes, cognitive performance and neurological dysfunctionPsychological Medicine 1987 16:49-57. [Google Scholar]
[13]. Malla A, Norman RMG, Williamson P, Three syndrome concepts of Schizophrenia : a factor analytic studySchizophrenia Research 1993 10:143-15. [Google Scholar]
[14]. Malla AK, Norman RMG, Aguilar O, Carnahan H, Cortese L, Relationship between movement planning and psychopathology profiles in schizophreniaBritish Journal of Psychiatry 1995 167:211-15. [Google Scholar]
[15]. Carter Cameron S, Barch Deanna, Cohen Jonathan D, Disturbed language processing disorganization, and attentional impairment in schizophreniaSchizophrenia Research 1997 1–2(24):130 [Google Scholar]
[16]. Highleya JR, Esiria MM, McDonalds B, Cortina-Borjab M, Cooperc SJ, Herrond BM, Anomalies of Schizophrenia Research cerebral asymmetry in schizophrenia interact with gender and age of onseta post-mortem study 1998 1(34):13-25. [Google Scholar]
[17]. Krieger S, Lis S, Gallhofer B, Cognitive subprocesses and schizophrenia. A reaction time decompositionActa Psychiatr Scand. 2001 104(suppl.408):18-27. [Google Scholar]
[18]. Suwa H, Matsushima E, Ohta K, Attention disorders in schizophreniaPsychiatry and Clinical Neurosciences 2004 58:249-56. [Google Scholar]
[19]. Turner TH, A diagnostic analysis of the case books of Tilehurst House AsylumPsychological Medicine, Monograph Supplement 21 1992 New YorkCambridge University. Press:1845-90. [Google Scholar]
[20]. Ngan Elton TC, Liddle Peter F, Reaction time, symptom profiles and course of illness in schizophreniaSchizophrenia Research 2000 2(46):195-201. [Google Scholar]
[21]. Heinrichs DW, Buchanan RW, Significance and meaning of neurological signs in schizophreniaAmerican Journal of Psychiatry 1988 145:11-18. [Google Scholar]
[22]. Levander S, Jensen J, Grawe R, Tuninger E, Schizophrenia – progressive and massive decline in response readiness by episodesActa Psychiatr Scand. 2001 104(suppl. 408):65-74. [Google Scholar]
[23]. Liddle F, Friston KJ, Frith CD, Hirsch SR, Jones T, Frackowiak RSJ, Patterns of cerebral blood flow in schizophreniaBritish Journal of Psychiatry 1992 160:179-86. [Google Scholar]
[24]. Chudasama Y, Robbins TW, Psychopharmacological approaches to modulating attention in the five choice serial reaction time task : implications for schizophreniaPsychopharmacology 2004 1:86-98. [Google Scholar]
[25]. Yoichiro Takayanagiabe, Tsutomu Takahashia, Lina Orikabebc, Naohisa Masudabc, Yuriko Mozued, Kazue Nakamuraa, Yasuhiro Kawasakia, Masanari Itokawabe, Yoko Satof, Hidenori Yamasuec, Kiyoto Kasaic, Yuji Okazakib, Michio Suzukia, Volume reduction and altered sulcogyral pattern of the orbitofrontal cortex in first- episode schizophreniaSchizophrenia Research 2010 1(121):55-65. [Google Scholar]
[26]. Salvatore Mannuzza, Cross-Modal Reaction Time and Schizophrenic Attentional Deficit: A Critical ReviewSchizophrenia Bulletin 1980 4(8):654-75. [Google Scholar]