An intussusception is the invagination of a segment of the proximal bowel (intussusceptum) into the lumen of the distal bowel i.e. intussuscipiens. Majority (90%) of the intussusceptions are ileocolic, while the remaining 10 % are of the ileoileal or the colocolic types [1].
An idiopathic intussusception is the most common cause of the small intestinal obstructions in the infant-toddler age group, with a peak incidence between 6 months to 3 years of life [1,2]. The incidence of the intussusceptions outside this peak age group should always be observed suspiciously for the presence of some pathologic lead points such as enlarged lympnodes, ileo-ilial intussusceptions, Meckel’s diverticulum, swollen Payer’s patches, polyps, etc. [1–3].
The purpose of our study was to ascertain the usefulness of an ultrasound guidance in the hydrostatic reductions of intussusception in children and thus to save them from the exposure to ionizing radiations which are associated with barium enema and the risk which is associated with surgery and post-operative complications.
Materials and Methods
The study group comprised of children with the complaints of diarrhoea, blood or blood clots in stool, lethargy, pain and swelling in the abdomen, who were referred to the Department of Radiology of a tertiary health care centre during the period from March 2006 to July 2009. A total of 41 children were evaluated with ultrasonography for the confirmation of the presence of intussusceptions and they were further evaluated with colour Doppler studies to rule out ischaemia.
Seven children who had a scattered vascularity or who had no vascularity were excluded from the study, to avoid complications like perforation of the bowel and in 4 children with the ileo-ileal type of intussusceptions, hydrostatic reductions were not done. The inclusion criteria which were considered were children with symptoms for less than 48 hours, the presence of blood flow in the affected segment of the bowel on colour Doppler studies, no history of a previous abdominal surgery, absence of the signs of perforation or peritonitis and the absence of a generalized toxicity [4].
Procedure
The children who fulfilled the inclusion criteria were taken to the Paediatric Intensive Care Unit (PICU) for hydrostatic reductions after a fluid resuscitation and correction of the dehydration. The procedure was explained in detail to their parents and an informed consent was obtained from them. Simultaneously, a surgical support was also kept ready. Under a short general anaesthesia with the use of Ketamine [I.V, 0.5 to 1 mg / kg], a well lubricated Foleys catheter [16-18 F] was introduced per rectally for 6-9cm, with the child in the left lateral position. The bulb of the Foleys catheter was inflated with 25-30 ml of distilled water and its position was confirmed with ultrasonography.
An enema-can filled with 500 ml of normal saline which was at room temperature, was kept at a height of 100-120 cm above the table-top. With the child in the head low position, the normal saline from the enema-can was instilled into the rectum and the movement of the fluid column was followed up to the mass (intussusceptions) under ultrasound guidance. The reduction of the intussusceptum was studied under the guidance of ultrasonography by using a 5-10 MHz transducer (GE, Logiq book, USA). The movement of the tip of the intussusceptum was constantly observed up to the caecum and the ilio-caecal valve until a complete hydrostatic reduction of the intussusception was achieved. While this procedure was performed, the upper limit of the normal saline which was instilled was 1000 ml and the maximum duration before which the procedure was abandoned was kept as 30 minutes, provided the vital statistics of the patients remained stable.
After the complete hydrostatic reduction of the intussusception, the normal saline which was instilled in the large bowel was allowed to drain back into the enema-can. Before removing the Foley’s catheter, an ultrasound examination was carried out to confirm the complete reduction of the intussusception and to rule out the leakage of fluid into the peritoneum, the presence of any lead point and the status of the bowel peristalsis. After the procedure, the children were kept nil orally and under observation for 4 hours in the PICU. A follow up ultrasound study was performed after 24 hours to rule out any recurrence.
Results
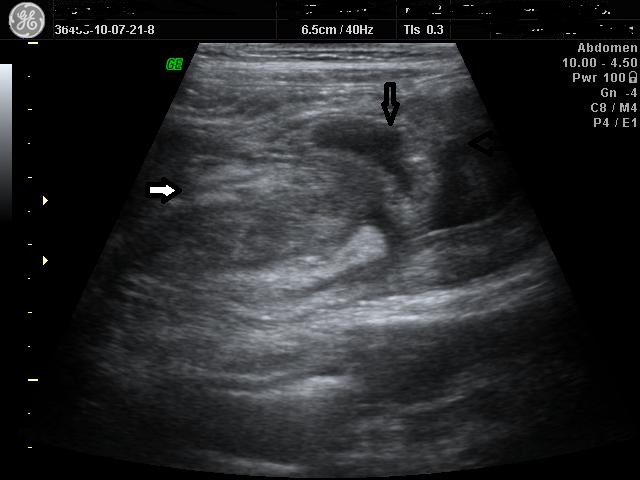
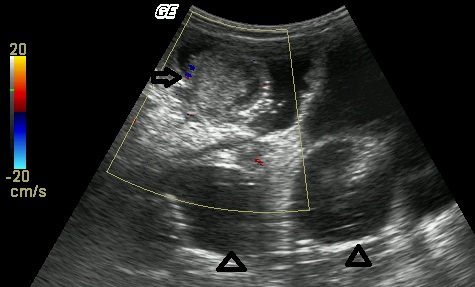
In the present study group of 41 ultrasound confirmed cases of intussusceptions, ultrasound guided hydrostatic reduction was attempted in 30 children. The mean age of the children in the present study was 15 months, with majority of the children belonging to the age group of 6 to 24 months (66%) [Table/Fig-1]. There was a preponderance of males (66%), with a male-female ratio of 2:1. The commonest symptom which was observed was diarrhoea with a bloody stool (80%), followed by cold-cough (40%) and pain in the abdomen (30%). The most common site of the intussusception was the transverse colon near the hepatic flexor of the colon (90%). Complete reductions of the intussusception is achieved in 26 out of the 30 patients, while in 4 patients, only partial reductions were possible, with a success rate of 87%. The partial reductions were observed with real-time ultrasonography during the procedure of the hydrostatic reduction, where due to the pressure of the fluid column on the intussusceptum, it was seen to gradually reduce and move from the transverse colon to the ascending colon, but reductions up to the caecum were not achieved. On ultrasound, this residual intussusception appeared as a complex, multilayered, mixed, echogenic mass lesion which was just proximal to the caecum, with the fluid column of the normal saline proximal to it [Table/Fig-2]. This fluid didn’t move distal to the mass even after a wait of 30 minutes after the instillation of the normal saline (upto 1000 cc). The postevacuation ultrasound showed a persistent pseudokidney lesion.
In the cases with successful reductions, no post procedure complication or recurrence was found. Four cases which could not be reduced hydrostatically, underwent surgery, out of which 2 patients had enlarged lymphnodes, one patient had Mickel”s diverticulum and one patient had a polyp in the ascending colon as the lead point. The amount of normal saline which was used, ranged from 500-1000 ml (average 700 ml) and the mean reduction time was 14 minutes (minimum 3 minutes, and maximum up to 30 minutes).
Discussion
Intussusceptions are the second most common cause of acute intestinal obstructions in children. Once they are diagnosed, they should be treated as early as possible. Though their exact causes are not known in most of the cases, swollen Payer’s patches, enlarged lymph nodes, polyps, Meckel’s diverticulum and duplication cysts have been suggested as few of the common aetiological factors [1–4].
Ultrasonography is very useful investigation that can be used for the diagnosis of intussusceptions, which has a high sensitivity [98-100%] and specificity [88-100%] [5]. The absence of blood flow in the lesion on Colour Doppler study correlates significantly with the high incidence of the complications and the irreducibility which are seen in non-surgical methods [4,6]. The various diagnostic points of the intussusceptions which are seen on ultrasound and on colour Doppler [Table/Fig-3 and 4] studies [2] have been enumerated in [Table/Fig-5]. An ultrasound guided hydrostatic reduction with the use of normal saline is believed to be one of the most promising methods for the non-surgical treatment of paediatric intussusceptions [4,5]. It is a simple, effective, economical and a less time-consuming procedure which is coupled with fewer complications (a very low perforation rate), no radiation hazards and a minimal hospital stay.
Age and gender wise distribution of various subjects among the study group
| Age of the subjects | Number of subjects (n= 30) | Males | Females |
|---|
| < 6 months | 03 (10 %) | 2 | 1 |
| 6 months - 2 years | 18 (66%) | 10 | 8 |
| 2 years- 5 years | 08 (20.7%) | 7 | 1 |
| >5 years | 01 (3.3%) | 1 | – |
| Total | 30 | 20 | 10 |
Complex mixed echogenic mass lesion of intussuscep-
tions (white arrow). Fluid column is seen proximal to it (black arrows)
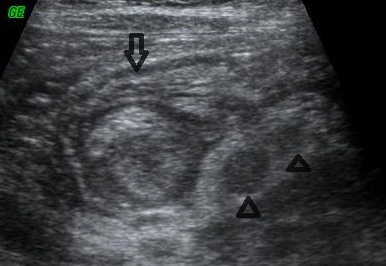
Ultrasound- T.S.-Target lesion of intussusceptions (open arrow) with few enlarged lymphnodes
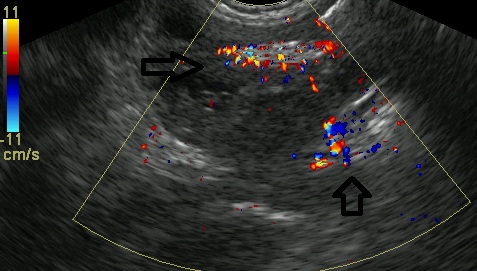
Pseudokidney lesion with internal vascularity on Colour Doppler Study
Diagnostic points of intussusception on ultrasound with colour Doppler study
| Oval pseudokidney mass lesion with central echoes on longitudinal imaging |
| Sonolucent donought or target lesion configuration in cross sectional imaging |
| Various layers and concentric rings may represent mesentry and bowel wall that has been drawn into the intussusception |
| Sonolucent periphery is due to oedematous wall of intussuscepted intestinal head |
| fluid,enlarged lymph nodes, dilated adjacent loop |
| On colour Doppler study blood flow within the mass suggests bowel wall viability while scattered or no blood flow suggests impared vsacularity |
| Presence of other soft tissue / cystic mass suggests a pathological lead point |
Instillation of normal saline up to intussusception (arrows)
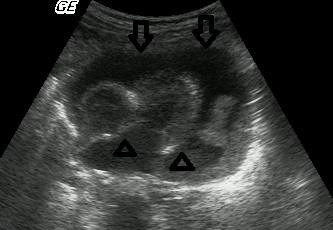
Reducing intussusceptum (arrow) with surrounding fluid filled loops (arrow heads)
It is also associated with less morbidity i.e. there is no incidence of a pseudo-reduction as is seen in the fluoroscopic guided procedures; there is no fluctuation in the intra-colonic pressure as is seen in air enema; even if a perforation occurs, there are minimum chances for chemical peritonitis as it occurs with barium enema; there is no tension in the pneumo-peritoneum as is seen in air enema; there is no chance for fluid shifts as has been linked with hypertonic contrast medium solutions or tap water. The mortality rate is also nil i.e. there is no reported case of death as in air enema [4,6,7].
The real time ultrasound shows the whole process of the reduction and hence, there remains no confusion about it [Table/Fig-6 and 7] however, the oedematous ileocaecal valve sometimes mimics a residual intussusception. Further, a pathological lead point may be identified and even a recurrence can also be treated by the same method.
The contraindications for hydrostatic reductions include an absent or a scattered vascularity within the lesion on colour Doppler studies, evident signs of perforation and peritonitis, ascites, multiple intussusceptions and recurrent intussusceptions with known pathological lead points. However, a minimal free fluid without any signs of perforation or peritonitis is not a contraindication for a hydrostatic reduction of an intussusception.
In the present study, the clinical findings like the age and the sex of the patients, the site of the intussusception, and the mean time of the reduction were comparable to those of other studies which have been mentioned in the references [4]. A history of gastroenteritis and upper respiratory tract infection has been reported in 20% of the patients, but in our study, the concurrence of these infections with intussusceptions was observed in 80% and 40% of the cases respectively.
In our case series, complete ultrasound guided hydrostatic reduction of the intussusceptions was achieved in 26 out of the 30 patients, with a success rate of 87%. This was similar to the findings of Krishnakumar et al., [4] and Del Pozo G et al., [5] where the success rate of the ultrasound guided hydrostatic reductions was more than 80%, which was somewhat more that the success rate of 78% of SA Alamdaran et al., [8] and that of 73% which was achieved in the study of Chan KL et al. [9]. Our results further suggest that age, duration of the symptoms, and the site of the intussusception are not the contraindications for a non-surgical reduction.
Though this technique is very useful in the recent onset intussusceptions which present within 48 hrs, the longer time lapses in the presentation should not be a contraindication in trying this method in the absence of abdominal or systemic complications [2,4,6]. The assessment of the affected bowel loop with colour Doppler ultrasound for the presence of vascularity is an added advantage in deciding the prognostic outcome.
Conclusion
Ultrasound with colour Doppler studies plays a promising role in both the diagnosis as well as the guided reduction of intussusceptions by using hydrostatic pressure with normal saline enema, as we can directly visualize the whole process of the reduction with real time ultrasound. A hydrostatic reduction of an intussusception under ultrasound guidance is a very simple and a safe method for the reduction of intussusceptiona in children with hardly any complications. However, a complete reduction is not possible in the cases where a pathological lead point is present; still, the introduction of normal saline enema helps in a partial reduction of the intussusception and the surgery can be planned accordingly.