Although diabetes has been considered to be a risk factor for the cognitive impairment, the cognitive function of the diabetic patients is not usually evaluated in the routine clinical care. Cognitive impairment might be another factor which is associated with a poor diabetes control and also with the bad adherence of the patients to educational approaches such as diet orientations [5]. When it is detected early; by various means like a proper diabetic control, drugs, cognitive training, etc., dementia can be prevented in the later life.
Mini Mental State Examination (MMSE) which was devised by Folstein et al., in 1975, is the most widely used screening test for cognition impairment in the world [6]. The Modified Mini-Mental State Examination (3MS) was developed by Teng and Chui in 1987, to overcome the shortcomings of the Mini-Mental Status Examination, specifically its narrow range of possible scores and ceiling effects. The 3MS is a significantly better predictor of the functional outcome than the MMSE and it has been found to have a higher sensitivity in detecting dementia [7].These tests require no specialized equipment and they need less time, thus making them inexpensive and portable.
The role of variables like the duration of diabetes, the diabetic control and the microvascular complications in the causation of a cognitive decline, in patients with type 2 diabetes, has not been well studied [8]. In this study, we assessed the cognitive status of diabetics and non diabetics by doing MMSE and 3MS and also found a correlation of age, sex, the duration of diabetes and HbA1C with the cognitive status among the diabetics.
Materials and Methods
After obtaining clearance from the human ethics committee of the PSG Institute of Medical Sciences and Research, a cognition assessment was done in 30 diabetics and in 30 non diabetics. An informed consent was obtained from both the groups. Thirty patients who were diagnosed to have diabetes mellitus according to the WHO criteria were selected as the cases and 30 non diabetics were taken as the controls, which included both males and females above the age of 50 years. Both the groups had educational qualifications of high school level and above. The patients with a poor control of diabetes, those with other metabolic abnormalities and those who had psychiatric problems and stroke, were excluded from our study. A detailed relevant history regarding the diabetes and its treatment and the investigations which were done, was obtained. Detailed general and systemic examinations were done. The MMSE and the 3MS tests were conducted on both the diabetics and the non diabetics. The MMSE is a fully structured scale that consists of 30 points which are grouped into 7 categories: orientation to the place (state, country, town, hospital and floor), orientation to the time (year, season, month, day and date), registration (immediately, repeating three words), attention and concentration (serially subtracting 7, beginning with 100, or, alternatively, spelling the word world backward), recall (recalling the previously repeated three words), language (naming two items, repeating a phrase, reading aloud and understanding a sentence, writing a sentence, and following a three-step command), and visual construction (copying a design) [9].
The cognition scoring was corrected for age and the educational qualifications in MMSE. The MMSE score was out of 30. The normal range of the scores depended on the education. The low-normal cut off was estimated by Crum et.al (1993) to be 19 for uneducated people, 23 for the graduates of elementary or junior high school, 27 for the high school graduates and 29 for the college graduates [10]. Since, our subjects were of high school education and above, we used the MMSE scores of 27 and above as the cut off limit for a normal cognition.
More recently, Folstein, McHugh, and Fanjiang.(2001) recommended the following cutoff scores for the classification of the cognition impairment . The MMSE scores of ≥27 revealed a normal cognition, those of 21–26 revealed a mild cognitive impairment, those of 11–20 revealed a moderate cognitive impairment and those of ≤10 revealed a severe cognitive impairment. We used these cut off scores to grade the cognition level.
The criteria which were created by Crum et al., (1993) were used to compare our patients’ MMSE scores with a reference group, based on their ages and educational levels [10]. Our diabetic patients fell within the age group of 50-70 years and they had high school education and college education. The normal cutoff for the people with a high school education in the age group of 50-70 years was 28 and for those with a college education, it was 29. A score which was lesser than this, was taken as an impaired cognition. The MMSE scores were corrected for the age and the educational qualification, according to this.
A Modified Mini Mental Status Examination (3MS) was done along with the MMSE. It is a 15 item extension of the MMSE, that assesses the orientation (self, time, place), attention (simple, complex), memory (recall and recognition, a second recall after a longer delay), language (naming, verbal fluency, repetition, following commands, writing), construction and executive functioning (similarities) [11]. These modifications are designed to sample a broader variety of cognitive functions, to cover a wider range of difficulty levels, and to enhance the reliability and the validity of the scores. The 3MS retains the brevity, ease of administration, and the objective scoring of the MMSE, but it broadens the ranges of the scores from 0-30 to 0-100 [12]. For example, the item that requires the individuals to copy the interlocking pentagons is scored as 0 (incorrect) or 1 (correct) on the MMSE, but it is given a 0 to 10 point range on the 3MS. The 3MS was found to have a higher sensitivity than the MMSE and a similar specificity. The 3MS was a significantly better predictor of the functional outcome than the MMSE. In the large community samples, the cut off score for the cognitive impairment typically was 77 [13,14]. The interpretation for the 3MS was: 78–100 - normal cognition, ≤ 77 - moderate cognitive impairment and ≤ 49 – severe cognitive impairment. One of the advantages of the 3MS modification is that both a 3MS and an MMSE score can be derived from a single administration [15].We used this to do the scoring for the MMSE and the 3MS among the diabetics and the nondiabetics. These tests took about 15 minutes only.
The analysis was done by using the SPSS software, version [13]. The unpaired t test and one way ANOVA were used for various analyses. A p value of < 0.05 was considered to be statistically significant.
Results
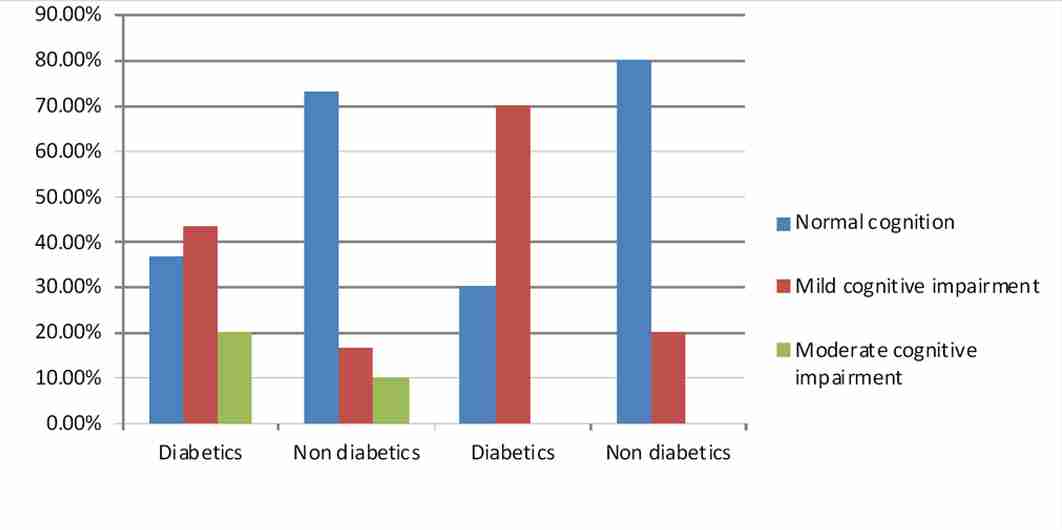
The decrease in the MMSE and the 3MS scores in the diabetics as compared to those in the non diabetics was highly significant (p < 0.001) as per the unpaired t test [Table/Fig-1]. The percentage of the diabetic persons with various levels of cognition, considering the MMSE scores, were as follows: 11 persons (36.67%) had normal cognition (MMSE scores of ≥ 27), 13 persons (43.33%) had a mild cognition impairment (MMSE scores of 21–26) and 6 persons (20%) had a moderate cognition impairment (MMSE scores of 11–20). A severe cognition impairment (MMSE scores of ≤ 10) was seen in none of the diabetic persons. Considering the MMSE in the non diabetics, 22 persons (73.33%) were found to have normal cognition, 5 persons (16.67%) had a mild cognition impairment and 3 persons (10%) had a moderate cognition impairment. None had a severe cognition impairment [Table /Fig-2].
The percentage of the diabetic persons with various levels of cognition, considering the 3MS scores, were as follows: 9 (30%) had normal cognition with the 3MS scores of 78–100, 21(70%) had a moderate cognition impairment with the 3MS scores of ≤ 77 and a severe cognitive impairment with the 3MS scores of ≤ 48 was seen in none. In the non diabetics, considering the 3MS, 24 (80%) were found to have normal cognition and 6 (20%) had a moderate cognitive impairment [Table/Fig-2]. 63.33% of the diabetics and 26.67% of the non diabetics were found to have an impaired cognition by the MMSE test. 70% of the diabetics and 20% of the non diabetics were found to have an impaired cognition by the 3MS test.
The 30 diabetics were of the age group of 50–70 years. Eleven had high school education and 19 had college education. On making the correction for age and educational qualification for the MMSE scores, it was found that all the 11 with a high school education had a decreased cognition (MMSE scores of < 28) and that among the graduates, 13 had a decreased cognition (MMSE scores of < 29) and that 6 had normal cognition (MMSE scores of ≥ 29). Only 20% had normal cognition and 80% had reduced cognition when a correction was made for age and the educational qualifications, as per Crum et.al’s criteria [10]. Among the non diabetics, 13 had high school education and 17 had graduation. It was found that 22 persons (73.33%) had normal cognition and 8 persons (26.67%) had decreased cognition on making a correction for the age and the educational qualifications.
Comparison of MMSE and 3MS scores among diabetics and non diabetics
| Test | Group | Mean ± SD | p value |
|---|
| MMSE | Non diabetics | 27.89 ± 3.62 | 0.001 |
| | Diabetics | 24.48 ± 3.97 | |
| 3MS | Non diabetics | 90.28 ± 10.88 | 0.001 |
| Diabetics | 73.23 ± 13.25 | |
Percentage of diabetics and nondiabetics with normal cognition, mild and moderate cognitive impairment by MMSE and 3MS test
Regarding the correlation of the age of the diabetics with the 3MS scores, the diabetics were divided into 3 age groups: 50-56 years - 5 persons, 57-63 years - 14 persons and 64-70 years - 11 persons. The analysis was done by using one way ANOVA. The difference between the 3MS scores between the 3 age groups was not statistically significant (p=0.101).
The comparison of the 3MS scores between the males and females was done by the unpaired t test. There were 18 males and 12 females. The mean ± SD of the 3MS scores in males was 72 ± 9.60 and in females, it was 75.17± 17.91. There was no statistically significant difference between the males and females, considering the 3MS scores(p=0.526). Regarding the correlation of the duration of diabetes with the 3MS scores, the diabetic persons were divided into 3 groups as follows: the duration of diabetes of 1-4 years - 11 patients, the duration of diabetes of 5-9 years - 11 patients and the duration of diabetes of > 9 years - 8 patients. The analysis was done by using one way ANOVA. The difference between the 3MS scores among the 3 groups was not statistically significant (p= 0.202). Regarding the correlation of HbA1C with the 3MS scores, the diabetic persons were divided into 3 groups, HbA1C of < 7% (2 patients), HbA1C of 7-8% (18 patients) and HbA1C of >8% (10 patients). The analysis was done by using one way ANOVA. The difference between the 3MS was not statistically significant (p= 0.188).
Discussion
Dementia is one of the most common and the most devastating diseases of late life; approximately 4.6 million new cases of dementia are estimated to occur worldwide every year and the number of people who are affected have been predicted to double every 20 years, 42 million by 2020 and 81 million by 2040. Diabetes mellitus increases not only the risks of the mild cognitive impairment but also the risk of the progression from such an impairment to dementia. The prediction of the progression to the dementia conversion is of considerable clinical importance [16].
Diabetes is considered as an epidemic disease nowadays, with about 173 million diabetic people all over the world [5]. Diabetes is a chronic disease which leads to long term complications, which include the risk of cognitive changes [17,5]>. A preserved cognitive status is essential for the understanding of the treatment and its compliance [5].
The validity of the MMSE as a screening tool for detecting dementia has been extensively studied [18]; its ability to detect the changes in the cognitive function for non-demented individuals has been documented mainly in the elderly [19]. Many intact individuals achieve total scores of near 30 and a cut off score of 23 on MMSE, has been shown to have adequate sensitivity and specificity (86% and 91% respectively) for detecting dementia in a community sample [20].
We assessed the cognition status of diabetics and nondiabetics by using the MMSE and the 3MS tests. Since our subjects had educational qualifications of high school graduation and above, we used a cut off of 27 for MMSE [10].There was a highly significant decrease in the MMSE and the 3MS scores in the diabetics as compared to the nondiabetics (p<0.001). This finding was consistent with those of various studies, which showed a cognition impairment in diabetics. As compared to the people without diabetes, the people with diabetes had a greater risk of a cognitive decline [21], especially in the memory and the executive functions [22].
63.33% were found to have a cognition impairment by MMSE and 70% had a cognition impairment by 3MS. The 3MS shows a slightly higher percentage of the impairment, as it involves an additional number of tests and a finer discrimination of the scoring. So, we used the 3MS test for finding the correlation between the age, sex, the duration of diabetes and the HbA1C values among the diabetics. 26.67% of non diabetics showed a cognition impairment by MMSE and 20% showed it by 3MS. This might be due to benign senescent forgetfulness, depression, metabolic disorders, vascular dementia, Alzheimer’s disease, hormonal diseases, etc.
Diabetes might accelerate the cognitive decline and the conversion to dementia through a number of potential mechanisms. These include the insulin resistance syndrome, the disturbances in the insulin homeostasis in the brain, hyperinsulinaemia, interplay with the insulin degrading enzyme which is involved in both insulin and amyloid proteolysis or the effects of insulin which signal on the tau metabolism and the generation of the advanced products of glycosylation. Whatever the mechanism, with an expected increase in the prevalence of diabetes in people of all ages, which include the older adults, the risk of developing dementia may increase [23]. A diabetes-induced cognitive decline may be induced via the disruption of the neurovascular coupling, not only with vascular disorders but also with the impairment of the astrocytic trafficking [24]. It was observed in our study, that the educational qualification affected the MMSE and the 3MS scores. The people with graduation scored better in the cognition tests, as was observed in various studies. The median MMSE score was 29 for the individuals with at least 9 years of schooling, it was 26 for those with 5 to 8 years of schooling, and it was 22 for those with 0 to 4 years of schooling [10].
Various studies which were done for the correlation of age, sex, the duration of diabetes and HbA1C on the cognition impairment showed contradictory results. The patients with a longer duration of diabetes achieved a lower score test and the glycaemic control which was measured by HbA1C, had no association with the MMSE score and possible dementia in the evaluation period [5,25]. We used 3MS to correlate the age, sex, the duration of diabetes and HbA1C with the cognition impairment. Even though males had decreased scores than the females, it was not statistically significant (P=0.526). The cause might be the small sample size, the small number of persons in each group, etc.
There was an inverse relationship between the MMSE scores and age, which ranged from a median of 29 for those who were 18 to 24 years of age, to 25 for the individuals who were 80 years of age and older [10]. There was no correlation of the age and the duration of diabetes with the cognition status in the diabetics in our study, as the p values were 0.101 and 0.202 respectively, as per one way ANOVA. There was no correlation between HbA1C and the cognition scores (p=0.188) in our study, as per one way ANOVA. There was no correlation of the age, sex, the duration of diabetes and HbA1C with the cognition impairment in our study. The association of the independent variables such as the duration of diabetes, the control of diabetes, the complications of diabetes, the other vascular risk factors and comorbid conditions such as depression with the cognitive decline in diabetics was negative [26].
The early implementation of mini-mental, which is a simple method of execution, can be done to detect the early stages of dementia. This test could be an important tool for assessing the ability of the patients in understanding their disease and treatment [5]. By treating the comorbid medical condition, by behavioural therapy and by cognitive training, dementia can be prevented.
The limitations of our study were that we assessed the cognition only by two tests. The other tests which are available are the Montreal cognitive assessment, the Queen square screening test, the Wechsler memory scale, the Trail making test, etc. The causes for the primary and secondary dementia were not ruled out. The early dementia which was caused by the metabolic and the structural causes was not excluded. Investigations like the lipid profile, vitamin B12, TSH, CT scan, and MRI have to be included in the study to find the other causes of dementia.
As a continuation of this study, the cognition tests can be repeated after a certain period and the impairment can be found. Other tests for the cognition assessment can be included in the study. Future studies can be done to identify the risk factors for the cognitive dysfunction and to elucidate its relationship with diabetes.
Conclusion
Diabetic patients have a decreased cognition as compared to the non diabetics. There is no correlation of age, sex, the duration of diabetes and the HbA1C values with the cognition impairment among the diabetics. The routine assessment of the diabetic complications should include the evaluation of the cognition status. By an early implementation of MMSE, we can detect even a mild cognitive impairment, so that the adequate treatment can be given, to prevent dementia.