The pork tapeworm can cause 2 distinct forms of infection. The form that develops depends on whether humans are infected with adult tapeworms in the intestine (Taeniasis) or with larval forms in the tissues (cysticercosis). Humans are the only definitive hosts for T. solium; pigs are the usual intermediate hosts, although dogs, cats, and sheep may harbour the larval forms. The ensuing clinical disorder is named after the name of the larval stage, cysticercosis cellulosae. Cysticercosis is a diagnostic and therapeutic dilemma for the clinicians.
Material and Methods
The clinico-pathological data of proven cases of soft tissue cysticercosis cellulosae on histopathological examination were studied during the past 5 year period. A total of 6805 biopsies were included in the study. The data were analysed in respect to the site and clinical presentations.
Results
A total of 6805 biopsies from different organs were studied of which 21 definite cases of soft tissue cysticercosis were found. The various age and sex and their distribution pattern is shown in [Table/Fig-1]. The age of these patients ranged from 3 years to 68 years. Of the 21 cases, 14 occurred in females and 7 in males. The commonest site affected was the striated muscles in 11 (52.4%), followed by eye in 6 (28.6%), subcutaneous tissues in 2 (9.5%), tongue in 1 (4.7%) and breast in 1(4.7%) case. Among the striated muscles, rectus abdominis was involved in 7 (63.67%) cases. Of the 6 cases of ocular cysticercosis, conjunctiva was affected in 3 (50%) cases, extraocular muscles in 2 (33.3%) and the eyelid in 1 (16.7%) case. Tongue was involved in 1 case.
| Case no. | Age (yrs.) | Sex | Site | Presentation |
|---|
| Case 1 | 9 | F | Forearm | Solitary |
| Case 2 | 14 | F | Conjunctival cyst | Solitary |
| Case 3 | 11 | F | Anterior abdominal wall | Solitary |
| Case 4 | 68` | F | Upper eyelid | Solitary |
| Case 5 | 7 | M | Anterior Abdominal wall | Solitary |
| Case 6 | 26 | F | Right Triceps | Solitary |
| Case 7 | 35 | F | Breast | Solitary |
| Case 8 | 12 | M | Subconjunctiva | Solitary |
| Case 9 | 48 | F | Left neck cyst | Solitary |
| Case 10 | 40 | M | Right Chest wall | Solitary |
| Case 11 | 10 | M | Anterior Abdominal wall | Multiple |
| Case 12 | 7 | F | Anterior Abdominal wall | Solitary |
| Case 13 | 9 | M | Right eye conjunctiva | Solitary |
| Case 14 | 4 | F | Medial Rectus Muscle | Solitary |
| Case 15 | 27 | F | Right Upper Arm | Solitary |
| Case 16 | 9 | M | Medial Rectus Muscle | Solitary |
| Case 17 | 7 | F | Anterior abdominal wall | Multiple |
| Case 18 | 20 | F | Calf Muscle | Solitary |
| Case 19 | 35 | F | Anterior abdominal wall | Solitary |
| Case 20 | 3 | F | Anterior abdominal wall | Solitary |
| Case 21 | 12 | M | Tongue | Solitary |
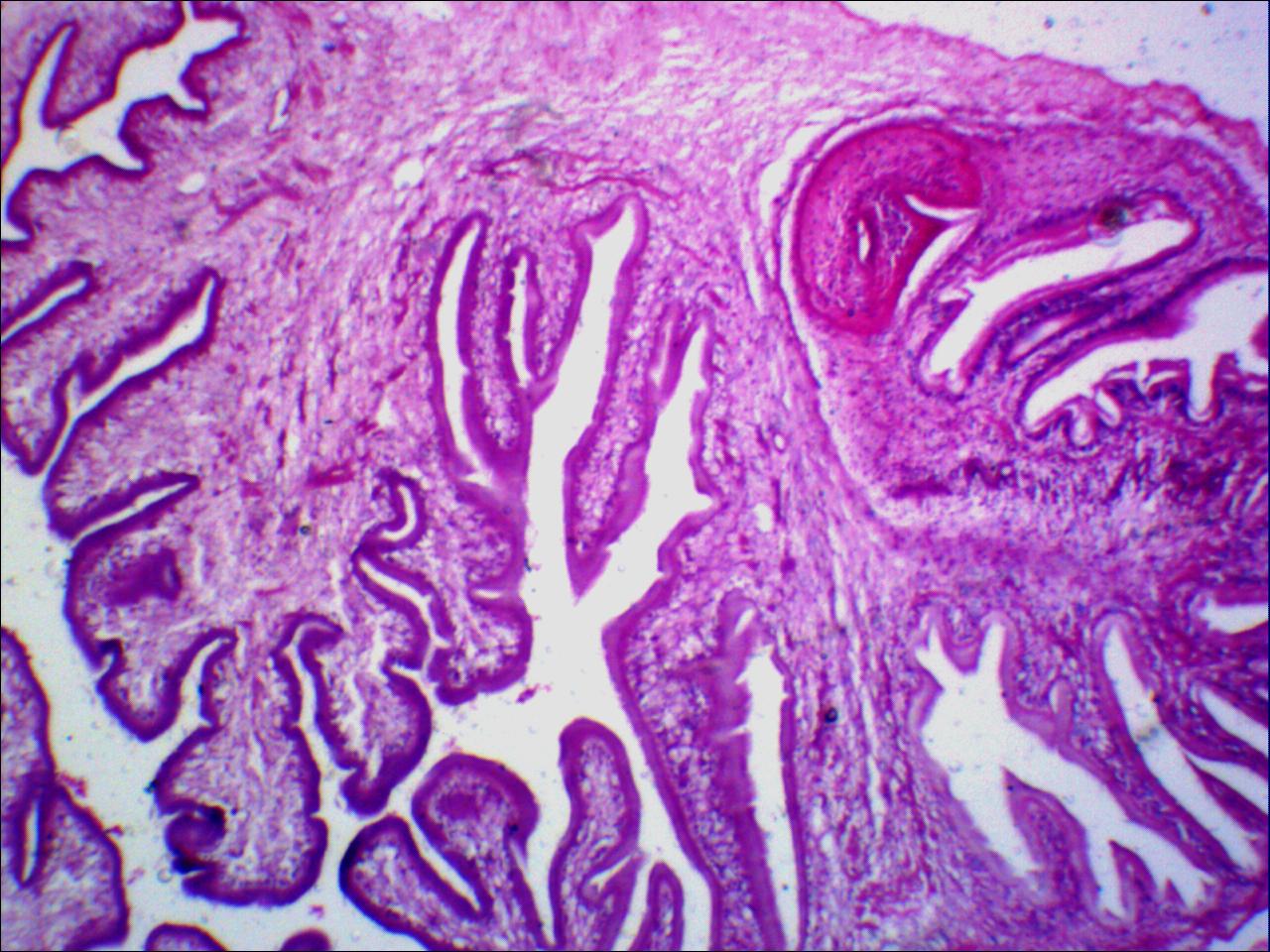
All the patients belonged to lower socio-economic status and were non-vegetarians. Only 2 (9.5%) cases had multiple lesions in the anterior abdominal wall. Twenty of the 21 cases presented as non-tender cysts. The subconjunctival cyst presented as a tender swelling. None of the patients had any other similar lesion anywhere else in the body other than the presenting organ. Excisional biopsy followed by histopathological examination confirmed the diagnosis in all the cases. The cross- section of the larva showed prominent wavy cuticular layer with aggravated subcuticular cells, prominent sucker and translucent hooklets [Table/Fig-2].
Discussion
Cysticercosis has been eradicated from most of the developed countries, but is still prevalent in Central and South America, South Asia, India and China [3]. It is likely that the disease is under reported in India because of lack of systematic population-based studies. There are great disparities within the country in geography, ethnicity, religious rituals, income, food habits, personal hygiene, level of education and standards of living, which influence the disease burden [3,4]. About 20-30% of the population is strictly vegetarian, but of the rest, only a minority eats meat products on a daily basis. A vast majority of the population (80%) are Hindus with varied beliefs and practices in different regions of the country and also between different castes in the same region. Consumption of beef (cow meat) is prohibited among Hindus and eating of pork is generally restricted to the lower socio-economic strata. Muslims constitute 14% of the population and they do not consume pork, whereas Sikhs, Jains, Buddhists, and Christians have differing dietary practices [1]. Cysticercosis appears to be more prevalent in the North especially Bihar, Uttar Pradesh and Punjab. There are only few reports from the State of Kerala probably due to the high level of education and standards of hygiene and from Jammu and Kashmir, India, a Muslim majority State due to prohibition of pork consumption by religion [2,5,6]. Toilet facilities are mostly limited to urban dwellers (30%) and it is estimated that only a quarter of the population has access to proper, hygienic toilets [5,7].
In cysticersosis the manifestations are different and depend on the location in the body, the number at a particular site and the associated inflammatory response or scarring. In 87% of cases cysticersosis presents as a solitary lesion [8]. In the present study 2 of the 21 cases had multiple involvement with anterior abdominal wall the affected site in both. Cysticercosis can occur anywhere in the human body, but has a known predilection for the nervous tissue, eyes, skeletal muscles and subcutaneous tissues. The basis of this selected tropism is still unknown. Involvement of the nervous tissue may cause severe morbidity as compared to the involvement of the subcutaneous tissue which mainly causes cosmetic problems. Neurocysticersosis may be associated with subcutaneous nodules comprised of extraneural cysts [2]. We restricted our study to involvement of soft tissue sites only so neurocysticercosis was not included in the present study. Presentation as subcutaneous nodule on upper arm, chest wall, eyes, abdominal wall and neck has been reported in this order of frequency [8-10]. It is very rare for cysticercosis to occur in the tongue muscle [8,11]. We came across a case of tongue involvement in a 21 years old hindu male who had an asymptomatic nodular swelling in the tongue and histopathological examination proved it to be cysticercosis.
Cross-section of larva showing cuticular layer, prominent sucker and translucent hooklets (H&E x 40).
Any site in the eye can be affected but the sub-retinal area and the vitreous humour are most commonly involved. Patients in the present study had varying ocular symptoms. Conjunctival involvement presented with blurring of vision while one patient had partial loss of vision especially during the night. One patient with subconjunctival lesion had tenderness. In the initial phase eye involvement may present clinically as scotoma and if the associated inflammation is severe, it may even cause loss of vision [10].
Cysticercosis of the muscles may cause severe ache, especially when the parasitism is heavy. None of the patients in the present study presented with severe pain. They had mild stretching pain or dull aching discomfort. The cysts in the striated muscles do not get the favourable environment and die early. After their death, they may calcify. Living parasites mostly do not elicit inflammatory reactions. When the parasite begins to involute, either naturally or after some anti-parasitic treatment, a surrounding granulomatous inflammatory response comprising predominantly of plasma cells, lymphocytes, eosinophils and macrophages occurs [12]. Later, in long standing cases, the dead cyst is surrounded by a dense layer of fibrosis or calcification.
Diagnosis of soft tissue lesions requires identification of the cysticercus in the involved tissue by histopathology, Computer Tomography (CT) and/or Magnetic Resonance Imaging (MRI). If the cyst has calcified, routine imaging (X-ray) can detect it. For soft tissue involvement, plain films may reveal multiple calcified “puffed-rice” lesions; however MRI gives specific findings [10]. X-Ray of the striated muscles showed soft tissue shadow in 2 cases only. MRI could be done in one case only where the parasite could be identified. All the cases in the present study were proved by histopathological examination. Grossly the cyst is oval, white to opalescent, upto 1.5cm long and contains invaginated scolex and hooklets. Many a times the whole parasite may not be visible and only the outer cuticular layer or areas of dead parasite with or without calcification were observed. Two of our cases posed similar diagnostic difficulty by way of the entire parasite not represented in histopathological section and only a part of the larva could be identified.
Asymptomatic patients with calcified soft tissue or neural lesions generally require no treatment. For symptomatic patients Praziquantel and/or Albendazole are effective. For ocular, ventricular and spinal lesions surgical resection is the best. Soft tissue lesion if symptomatic or cosmetically bad should be surgically excised.
Prevention
The major means of preventing infection is proper cooking of pork followed by minimizing the opportunities for ingestion of contaminated faeces by good personal hygiene and effective faecal disposal.
Conclusion
Cysticercosis is a global public-health problem, especially in developing countries including India. It is considered as a “biological marker” of social and economic development. Since cysticercosis is a preventable and eradicable disease, appropriate measures like health education, mass awareness, better medical facilities, mass treatment of T. solium carriers, and restriction on sale of contaminated pork may help to reduce the disease burden in the endemic areas. It is important to carry out a detailed medical evaluation in every case, in order to exclude the presence of the parasite at other sites especially while examining biopsies from the eye, striated muscles and soft tissues.