The development of the urinary system takes place from the intermediate mesoderm along the posterior wall of the abdominal cavity [1]. This growth begins around the 4th post conception week and it is complete by the 12th week [1,2].
Routine antenatal ultrasonography (USG) has become a part of the obstetric care and it is being increasingly used to detect the malformations of the foetal urinary system [3–10]. Foetal Magnetic Resonance Imaging (MRI) is a useful complimentary tool which can demonstrate the foetal urinary tract anomalies in excellent anatomic detail [11–13].
Though both USG and MRI are valuable examination tools, a foetal autopsy after the termination of a pregnancy, is essential to confirm the findings and to arrive at a definite diagnosis. There are only a few studies in the literature which have evaluated the type of urinary anomalies in aborted human foetuses [9,14]. A foetal autopsy can give significant additional information and it is helpful in identifying the cause of the foetal loss. It is also essential for genetic counselling. In the present study, we analyzed the incidence and type of the urinary anomalies in aborted foetuses by performing foetal autopsies.
Methods
This study was done in the Department of Anatomy, Government Medical College and Hospital, Chandigarh, India, on human foetuses which were sent by the Department of Obstetrics and Gynaecology of the same institute for routine autopsies. This study was conducted over a period of around 4 years (since January 2008 till date) after getting a clearance from the ethics committee of the institute. A total number of 226 foetal autopsies were done; among which 29 were afflicted with urinary abnormalities. These foetuses included spontaneous abortions, missed abortions, stillbirths, intra-uterine deaths and therapeutic abortions, after the recognition of the congenital malformations on ultrasonography. All the autopsies were done after providing the information on them and after taking a written consent of either the parents or the relatives. Each foetus was examined according to a pre-designed proforma, which included a comprehensive review of the maternal medical and/or the obstetrical history, which included the antenatal laboratory and the ultrasonography reports, the family history, the delivery record and the gross examination, followed by the autopsy.
The foetal weight and the general morphometric data were recorded. The abdomen was opened by making a midline incision and the intestines were removed. This exposed the kidneys, the pelviueteral system and the urinary bladder. The anomalies which were related to these structures were recorded. The foetuses were divided into five groups on the basis of their different gestational ages. The detected anomalies were classified and photographed.
Results
Incidence
A total of 226 aborted foetuses were autopsied and examined for urinary mal-development. Overall, 29 (12.83%) foetuses were found to have one or more urinary anomaly. Gender wise, 15 (12.82%) male foetuses were found to have urinary abnormalities, while 14 (12.84%) female foetuses were detected to have urinary anomalies. The renal agenesis demonstrated a male/female ratio of 1.5:1, while the anomalies which were related to the dilated pelviureteral system showed a male to female ratio of 3.6:1. On the other hand, the incidences of the polycystic and the horseshoe kidneys were more in the females, with the male/female ratio of 1:2.6. The gestational ages of the foetuses with the urinary anomalies ranged from 16 to 29 weeks. The mean weight of these foetuses was 365.46 gm (range: 123gm to 822 gm).
A total of 34 different urinary anomalies were found in the 29 foetuses. Four had more than one anomaly, while 25 had a single anomaly. The single most frequent abnormality which was seen was renal agenesis, which was seen in 11 cases. This accounted for 32.35% of all the urinary anomalies. Polycystic kidneys were detected in 8 foetuses, while horseshoe kidneys were found in 4. Taken together, the urinary anomalies which were related to the renal parenchyma accounted for 67.65% of all the anomalies of the urinary system. The anomalies which were related to the pelvi-ureteral system and the urinary bladder, were present in 7 foetuses. The pelvi-ureteral and the bladder anomalies constituted 20.59% of all the urinary defects. Renal agenesis was present in 37.93% of the foetuses with the urinary anomalies. 79.3% of the foetuses had anomalies which were related to the renal parenchyma, while the anomalies which were related to the pelviureteral system were present in 13.8% of the foetuses with urinary anomalies.
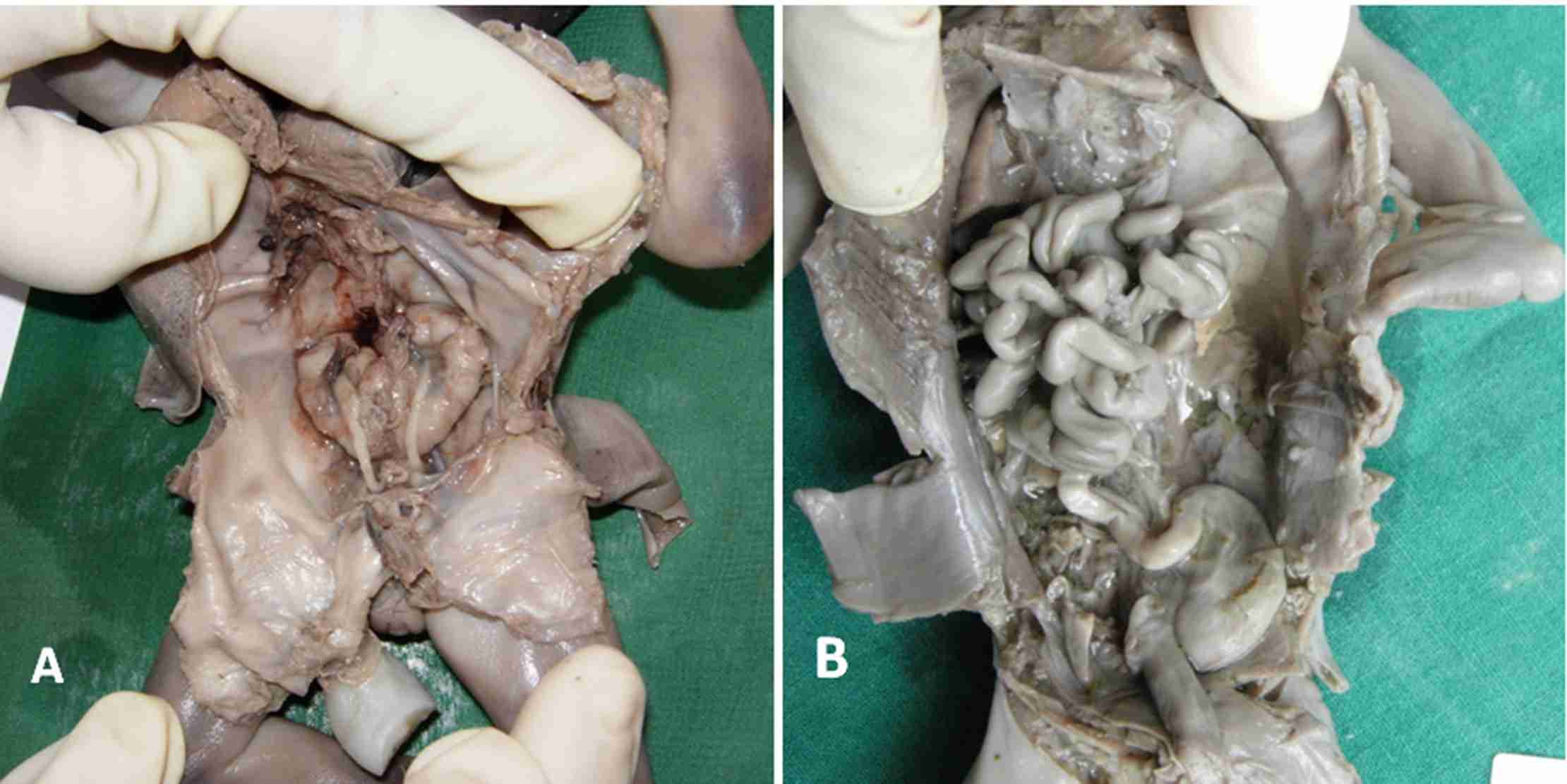
Photographs of aborted fetuses demonstrating a horse shoe kidney (A) and renal agenesis (B)
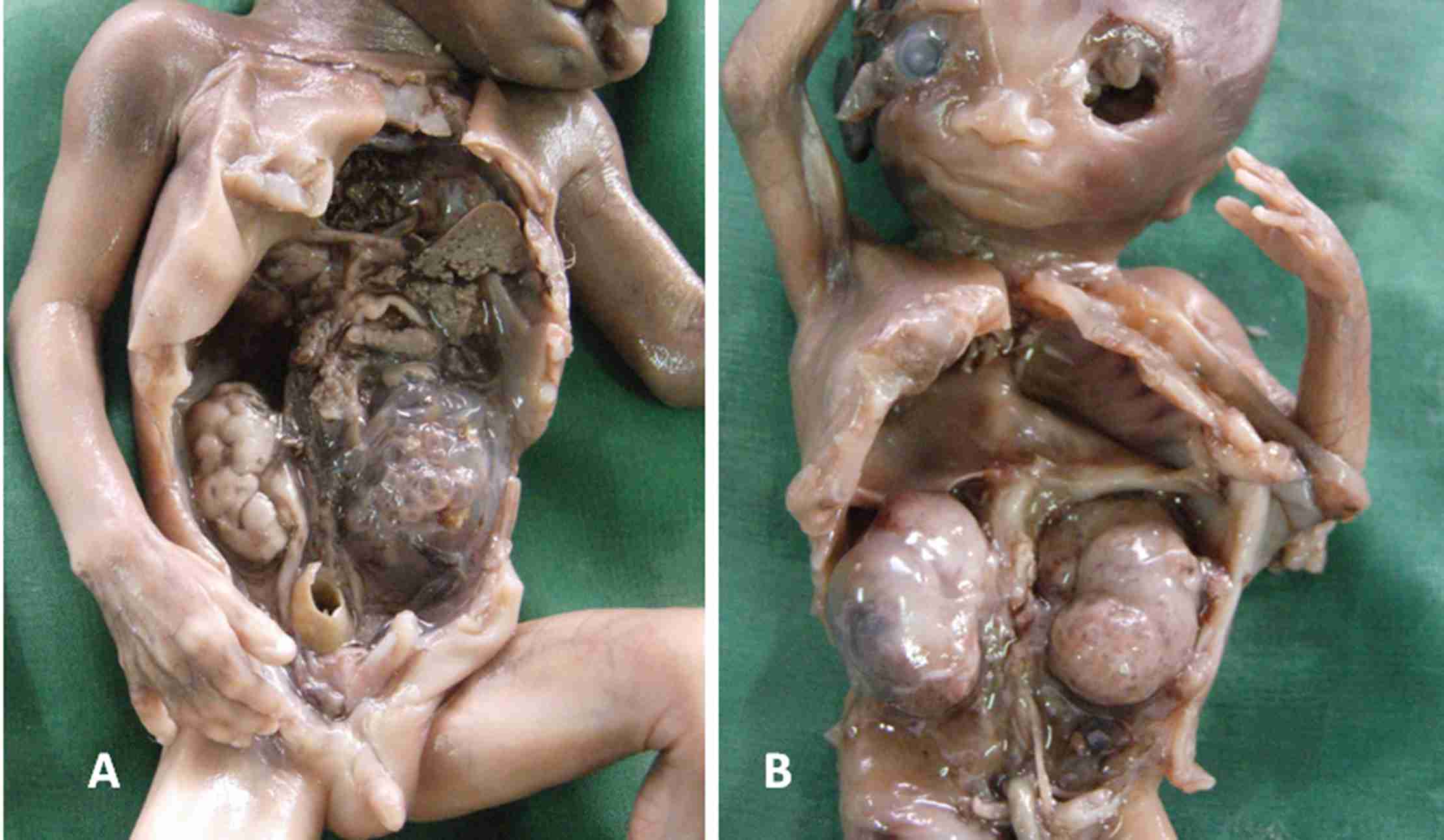
Photographs of aborted fetuses with unilateral (A) and bilateral (B) polycystic kidneys.
Four foetuses had more than one urinary anomaly. One foetus had a combination of polycystic kidneys and a dilated pelvis and a ureter, with hydronephrosis. Another had a polycystic kidney with renal agenesis. The third foetus had a combination of a dilated pelvi-ureteral system and an absent urinary bladder, while the fourth had a polycystic kidney and a dilated pelvis and a ureter along with oligohydraminos.
The Gestational Ages of the Foetuses with Urinary Anomalies [
Table/Fig-3]
The abnormalities in the development of the urinary system could be detected as early as 16-18 weeks post gestation. In this period, 4.43% of the foetuses which were examined were found to have urinary anomalies. All the anomalies could be detected by 28-30 weeks of gestation and the total incidence was 12.83% at this age.
The maximum incidence of the urinary anomalies was found in the foetuses which were between 22-24 weeks of gestation. The renal anomalies were more frequent in the 16th-24th weeks of gestation, while the pelvi-ureteral and the bladder anomalies were found to be more in the 24th-27th weeks of gestation.
The Associated Anomalies
The following associated anomalies were found in the foetuses with the urinary defects: those of the gastrointestinal tract – 7 foetuses; those of the central nervous system – 7 foetuses; those of the cardiovascular system – 4 foetuses; the hand foot genital syndrome -1foetus; those of the musculoskeletal system – 5 foetuses and cloacal dysgenesis – 1 foetus.
Discussion
The incidences of the urinary tract anomalies, as were detected antenatally by routine ultrasonic examinations, were reported to vary among 0.1%-2% of the foetuses [15–19]. In one of the largest screening programs for the detection of renal malformations, which was conducted in India, renal congenital malformations were detected in 0.19% of the pregnancies [4]. In another study which was performed to evaluate the prevalence of the prenatal ultrasonic diagnosis for renal anomalies in 20 registries of 12 European countries, at least one type of renal malformation was diagnosed in 1130 infants and foetuses among a total of 709,030 live births, still births and induced abortions [6]. The antenatal detection rates for the urinary malformations vary in different studies due to the diverse policies which are used for the antenatal screening, which may be related to the ethical and the religious backgrounds. It is not possible to comment on the prevalence of the urinary malformations in this foetal autopsy study, as we had the data of only those pregnancies which were terminated.
The incidence of the detection of the foetal urinary anomalies was also dependent on the time of the examination. In the foetuses which were examined in the present study, this incidence was 4.43% in the foetuses which were between 16-18 gestational weeks and this increased to 12.83% by 28-30 gestational weeks [Table/Fig-4]. Many of these anomalies could therefore be missed if only a single scan was done at 16-18 weeks of gestation. During a screening program on renal foetal malformations which was held in Sweden, only 9% renal abnormalities were detected by 17 weeks of gestation, while 91% could be detected by 33 weeks of gestation [20]. In our study, all the anomalies which were related to the urinary system could be detected by 30 weeks of gestation. Others have also reported that 95% of the foetal kidneys could be identified on ultrasonography by 22 weeks of gestation [4,21].
The joint study group on foetal anomalies recommended 2 scans, 1 dating scan at 16 weeks of gestation and the second anomaly scan at 20 weeks of gestation [22]. However, as per the findings of our study as well as those of others’ studies [19, 20], it is advisable to have an additional antenatal ultrasound between 28-36 weeks of gestation, to be able to detect all the urinary malformations. This is necessary for an early diagnosis and management in the post natal period before an irreversible renal damage has taken place.
Distribution of different types of urinary anomalies at varying gestational ages of aborted fetuses
| Age groups | Renal agenesis | Polycystic kidney | Horse shoe kidney | Oligohydraminos | Dilated pelvis & ureter | Absent bladder |
|---|
| 16–18 wks | 6 | 3 | | 2 | | |
| 19–21 wks | 2 | 2 | 1 | 1 | 1 | |
| 22–24 wks | 3 | 3 | 2 | 2 | 3 | 1 |
| 25–27 wks | | | | | 1 | |
| 28–30 wks | | | | | 1 | |
| Total | 11 | 8 | 4 | 4 | 4 | 3 |
Incidence of urinary anomalies in the aborted fetuses
| Age groups (n) | No of fetuses with Urinary anomalies (%)* | No. of Urinary anomalies | Cumulative incidence of fetuses with anomalies (%) |
|---|
| 16–18 wks (57) | 10 (17.54%) | 11 | 4.43 % |
| 19–21 wks (64) | 07 (10.93%) | 07 | 7.52 % |
| 22–24 wks (38) | 10 (26.32%) | 14 | 11.95 % |
| 25–27 wks (20) | 01 (5%) | 01 | 12.39 % |
| 28–30 wks (06) | 01 (16.67%) | 01 | 12.83 % |
| Total | 29 (12.83%) | 34 | |
Percentage was calculated out of total no. of fetuses in that age group.
The incidence of the sexual dimorphism varies in different series; Cortes et al., [18] found that the urinary anomalies in the male foetuses were twice as that in the female foetuses. A similar (2:1) male preponderance was reported by the Northern Region Foetal Abnormality Survey [23], while Sanghvi et al., [4] reported a male to female ratio of 3.3:1. In our study, the male/female ratio for all types of urinary malformations was almost 1:1. However, interestingly, we found that the gender ratio varied with the types of anomalies which were detected. A relatively higher male preponderance was seen with the anomalies which were related to the dilated pelvi-ureteral system. Sanghvi et al., [4], also reported a much higher male incidence (M: F=5.4:1) for the anomalies which were related to the dilated renal system. On the other hand, the incidences of the polycystic and the horseshoe kidneys were more in females.
Renal agenesis is one of the most frequent renal abnormalities, with an incidence between 1/200–1/4000 births [24]. In another study where a routine antenatal sonography was performed, an empty renal fossa was detected in 8/27 babies with renal malformations, while the anomalies which were related to the pelvicalyceal system were seen in 13 babies [19]. In our study, renal agenesis was present in 37.93% of the foetuses with urinary anomalies. Overall, 79.3% of foetuses had anomalies which were related to the renal parenchyma (agenesis, polycystic renal disease and horse shoe kidney), while the anomalies which were related to the pelviureteral system were present in 13.8% of the foetuses with urinary anomalies. The anomalies which were related to the dilated renal system alone were seen in 60% foetuses, while the renal parenchymal anomalies were present in 33% of the foetuses, with an antenatal diagnosis of a renal malformation [4]. Dicke et al., [7] reported a renal pelvis dilatation in 66.4% of the 342 foetuses with a sonographically detected foetal renal disorder. An observation in the present study was that the anomalies which were related to the renal parenchyma were detected in the relatively younger foetuses as compared to the gestational age of the foetuses with the pelviureteral and the bladder anomalies. Thus, the gestational age at the time of the detection could be the major reason behind the different frequencies of the various types of urinary anomalies in the reported results. Wiesel et al., [6] also found that the anomalies of the dilatation of the upper urinary tract were seen late in the pregnancy.
The detection of the associated anomalies is important. This could also give a clue about the cause of the abortion. Wiesel et al., [6] reported that 29% of the pregnancies with the antenatally detected renal anomalies were terminated. The terminations of the pregnancies were performed in 67% of the detected bilateral renal agenesis cases and only in 4% of the unilateral multicystic dysplastic renal malformation cases. The anomalies which were related to the other systems were seen in 45% of the foetuses with renal anomalies. In the antenatal care, the detection of the associated congenital anomalies is necessary, so as to decide whether to continue with the pregnancy or to proceed with the termination of the pregnancy. This decision is also dependent on the type and the severity of the urinary anomaly. The oligohydramnios which is associated with the urinary anomalies may lead to pulmonary hypoplasia [25]. An inadequate renal function may lead to lethal uraemia and the retention of urine can cause degeneration of the functional units of the kidney. All these have to be taken into account while the decision is being made. An intrauterine kidney puncture or a shunt procedure may delay the deterioration of the kidney function. The antenatal detection of the urogenital anomalies results in an earlier postnatal diagnosis and therapeutic management.
A wide range of genetic and chromosomal anomalies may be responsible for or may be associated with the foetal urinary abnormalities. Renal agenesis is associated with the autosomal dominant, the autosomal recessive, as well as the X-linked syndromes. Cystic kidneys may be seen as a component of the Bardel-Biedi syndrome, the Fryns syndrome or the Meckel-Gruber sundrome. Chromosomal anomalies such as trisomy 1q, mosiac trisomy 7, 8 or 9, trisomy 13, 18 or 21 and the Turner’s syndrome also result in urinary and renal developmental defects [26]. Gribouval et al., [27] reported a spectrum of mutations in the renin-angiotensin system genes in the autosomal recessive renal tubular agenesis. There is also accumulating evidence that the histone deacetylases can cause epigenetic modifications and that these may have a role in the regulation of the kidney development [28]. Therefore, the detection of the urinary anomalies in the foetuses warrants a complete investigation to define the genetic syndromes and the chromosomal defects and an early management.