Nifedipine, Haemodialysis
Introduction
Uncontrolled hypertension can progress to a hypertensive crisis which is defined as a systolic blood pressure of >180 mm Hg or a diastolic blood pressure of >120 mm Hg. A hypertensive crisis can be further classified as a hypertensive urgency or a hypertensive emergency, depending on an end-organ involvement which includes cardiac, renal, and neurologic injuries [1]. The seriousness of the emergency, the rapidity with which the BP should be lowered and the selection of the drug, are the keys. The prevalence of hypertension in the patients who are on dialysis is as high as 90% [2]. The hypertensive emergencies in haemodialysis require an immediate therapy, usually by parenteral drug administration; however, the sublingual medications may have a potential in this special condition.
Nifedipine is a dihydropyridine calcium antagonist. An L-type calcium channel blocker, nifedipine, increases the DMT-1-mediated cellular iron transport 10- to 100-fold at the concentrations which are between 1 and 100 microM. Mechanistically, nifedipine causes this effect by prolonging the iron-transporting activity of DMT-1 [3]. Its main uses are as an antianginal (especially in Prinzmetal’s angina) and as a antihypertensive. It works by relaxing the blood vessels, so that the heart does not have to pump as hard. It also increases the supply of blood and oxygen to the heart.
A prospective, non randomized, case control study was carried out to know the effectiveness and the safety of a single dose of 5mg Nifedipine(sublingual) in this subset of patients.
Materials and methods
This study was carried out at Adesh Institute of Medical Sciences and Research between January 2010 to January 2011.
Inclusion Criteria
All the cases of chronic renal failure who were hypertensive, who were maintained on regular haemodialysis, who were aged 18 years and above, who had high systolic and diastolic blood pressures of more than >220 systolic and >125 diastolic respectively during haemo dialysis, were included in the study.
Exclusion Criteria
The patients who were:-Haemo-dynamically unstable
Known cases of Coronary Artery Disease
Aged below 18 years
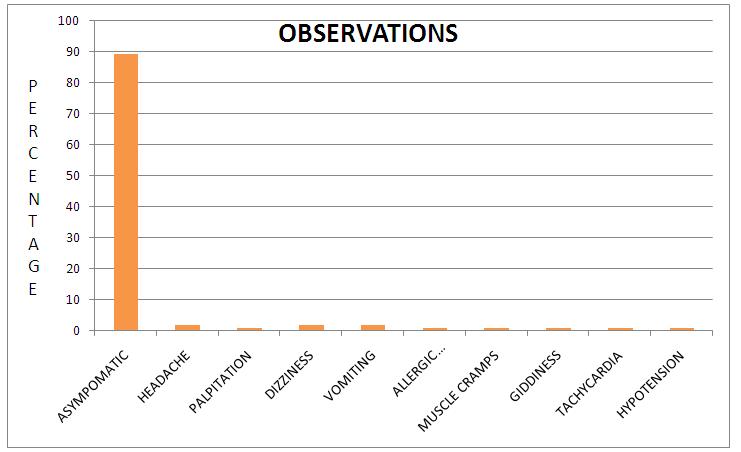
The patients were monitored for 5 hours. They were treated with a single dose of nifedipine (5mg sublingual route). They were closely monitored for possible side effects. The patients had high blood pressure during haemodialysis and were already on antihypertensives. A single dose of 5mg nifedipine was given to control the blood pressure. The extended release formulations of nifedipine were asked to be taken on an empty stomach, and the patients were warned not to consume anything which contained grapefruit or grapefruit juice, as they raised the blood nifedipine levels [4]. The side effects of the drug were closely monitored. The side effects such as headache, palpitation, dizziness, hot flushes, vomiting, chest pain, allergic reactions, muscle cramps, giddiness, tachycardia, hypotension, etc were witnessed.
Results and Observation
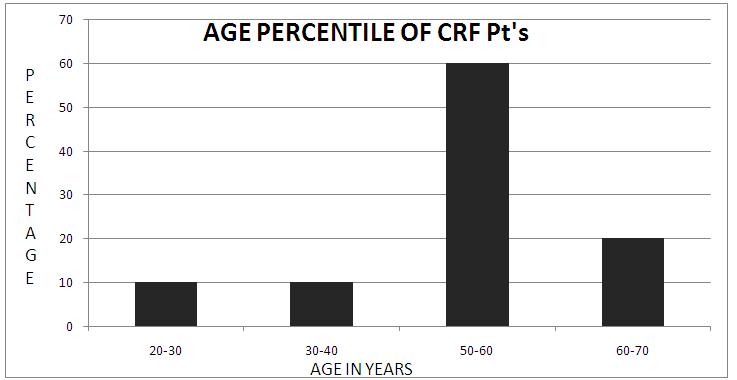
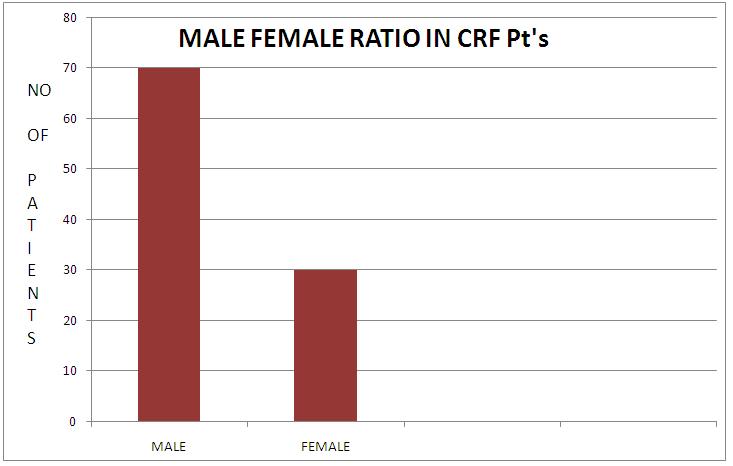
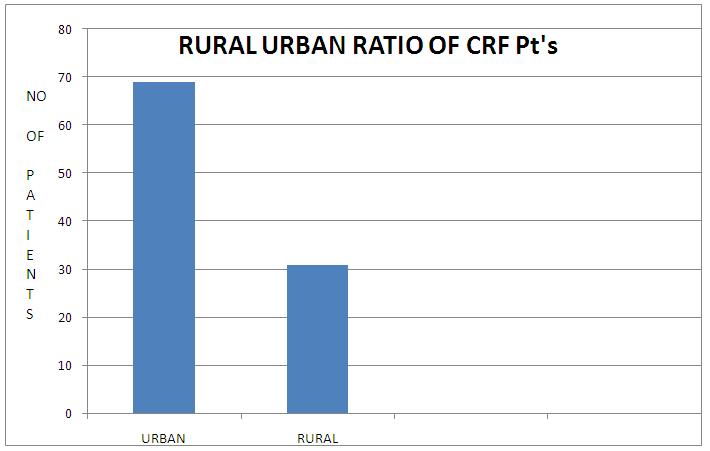
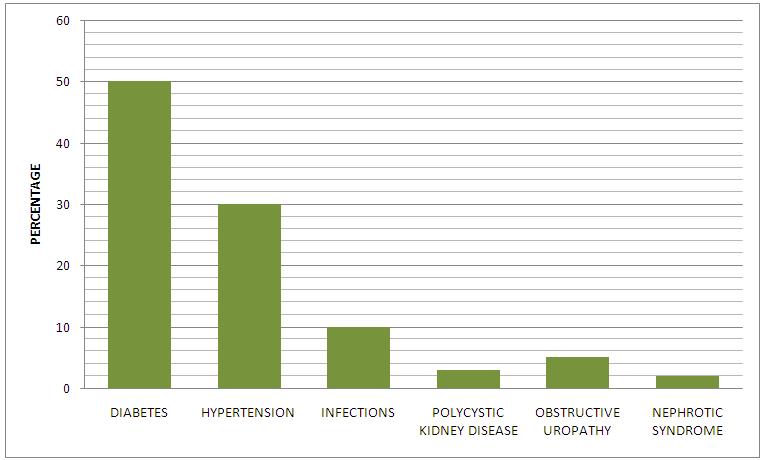
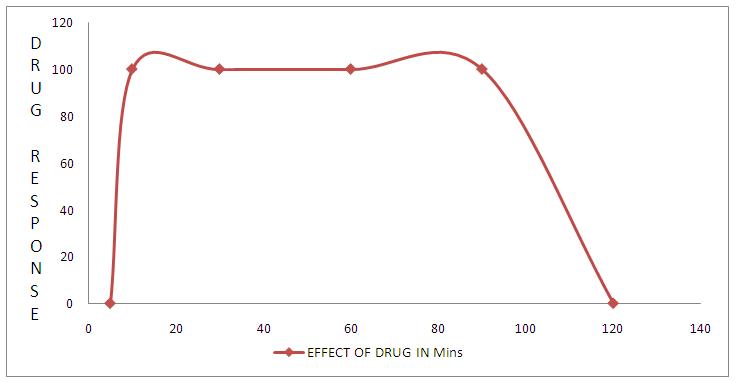
During the study period, about 100 patients of hypertension were on haemodialysis and they were observed, whose results have been shown in [Table/Fig-1] and in the [Table/Fig-2,3,4,5,6 & 7]. These patients were in the age group of 20-70 years. The maximum number of patients was seen in the 50-60 years age group [Table/Fig-2]. Out of the 100 patients, 30% were females and the rest (70%) were males [Table/Fig-3]. The chronic renal failure patients were more from the urban population than from the rural population [Table/Fig-4]. A maximum number of patients suffered from diabetes, followed by hypertension [Table/Fig-5]. Eighty nine patients were asymptomatic [Table/Fig-1] and [Table/Fig-2,3,4,5,6, 7]. The drug response can be seen in [Table/Fig-7].
| Headache | 2 (2%) |
| Palpitation | 1 (1%) |
| Dizziness | 1 (1%) |
| Hot flushes | 0 |
| Vomiting | 2 (2%) |
| Chest Pain | 0 |
| Allergic Reaction | 1 (1%) |
| Muscle cramps | 1 (1%) |
| Giddiness | 1 (1%) |
| Tachycardia | 1 (1%) |
| Asymptomatic | 89 (89%) |
| Hypotension | 1 (1%) |
Age Percentile of Crf Pt’s
Male Female Ratio in Crf Pt’s
Rural Urban Ratio of Crf Pt’s
Prevelance of Chronic Renal Failure
Discussion
Hypertensive emergencies require an immediate lowering of the blood pressure in a controllable and a predictable manner. The initial goal of the treatment was to reduce the mean arterial pressure by no more than 25%, to reach a goal blood pressure of 160/100 mm Hg within 2 to 6 hours, or to decrease the diastolic blood pressure to 10-15% or to approximately 110mm Hg within 30-60 minutes [5,6]. A rapid fall in the blood pressure in patients with severe hypertension may result in a permanent ischaemic damage due to the disturbances in the auto-regulation of the cereberal blood flow [7]. In this circumstance, it is recommended that the blood pressure may not be lowered. Nifedipine has been widely used via an oral or sublingual administration in the management of hypertensive emergencies, severe hypertension which is associated with chronic renal failure, perioperative hypertension, and pregnancy induced hypertension [8,9]. A significant decrease in the blood pressure is usually observed 5–10 minutes after the nifedipine administration, with a peak effect in between 30 and 60 minutes and a duration of action of approximately 6–8 hours [10].
Sublingual nifedipine causes blood-pressure lowering through a peripheral vasodilation. It can cause an uncontrollable decrease in the blood pressure, reflex tachycardia, and a steal phenomenon in certain vascular beds. There have been multiple reports in the medical literature of serious adverse effects with sublingual nifedipine, which include cerebral ischaemia/infarction, myocardial infarction, complete heart block and death. Furberg et al., reported that in patients with coronary disease, the use of a short-acting nifedipine in moderate to high doses causes an increase in the total mortality [11]. As a result of this, The Cardiorenal Advisory Committee of the US Food and Drug Adminsitration has concluded that the practice of administering sublingual/oral nifedipine should be abandoned, because this agent is neither safe nor efficacious [12-17].
However, this drug is not banned in India and it is widely used in a subset of patients like in those with pre-eclampsia, eclampsia and hypertensive emergencies and urgencies. We found that a low dose of sublingual Nifedipine (5mg) was very effective in controlling the blood pressure during haemodialysis and we also noticed that this drug had very minor side effects. Similarly, Samad and Shareef reported that sublingual nifedipine effectively and promptly lowers the elevated B.P. in a hypertensive crisis and that should it should be preferred over the costly cumbersome 1/V regimens which are used in hypertensive crisis [19-24].
Conclusions
It can be concluded that sublingual nifedipine was effective and that it seemed to have less side effects. It may be an excellent drug for the urgent treatment of hypertensive emergencies in haemodialysis. If we administer an IV drug, it will add on to the fluid overload and decrease the blood pressure very rapidly, because the bio availability of a drug is almost 100 percent through the IV route. By the intramuscular and the oral routes, the effect will take 45 minutes to 1 hour to take place and so that was why we concluded that sublingual nifedipine was a better option for this subset of patients.
[1]. Rodriguez MA, Kumar SK, De Caro M, Hypertensive crisisCardiol Rev 2010 18(2):102-07.Mar-Apr [Google Scholar]
[2]. Horl MP, Horl WH, Hemodialysis-associated hypertension: pathophysiology and therapyAm J Kidney Dis 2002 39:227-44. [Google Scholar]
[3]. Ludwiczek S, Theurl I, Muckenthaler MU, Jakab M, Mair SM, Theurl M, Ca2+ channel blockers reverse iron overload by a new mechanism via divalent metal transporter-1Nat Med 2007 13(4):448-54.Apr; Epub 2007 Feb 11. [Google Scholar]
[4]. Odou P, Ferrari N, Barthélémy C, Brique S, Lhermitte M, Vincent A, Grapefruit juice-nifedipine interaction: possible involvement of several mechanismsJ Clin Pharm Ther 2005 30(2):153-58.Apr; [Google Scholar]
[5]. Aggarwal M, Khan IA, Hypertensive crisis: hypertensive emergencies and urgenciesCardiol Clin 2006 24(1):135-46. [Google Scholar]
[6]. Varon J, Treatment of acute severe hypertensionDrugs 2008 68(3):283-97. [Google Scholar]
[7]. Bertel O, Conen D, Radü EW, Müller J, Lang C, Dubach UC, Nifedipine in hypertensive emergenciesBr Med J (Clin Res Ed) 1983 286(6358):19-21.January 1; [Google Scholar]
[8]. Komsuoglu SS, Komsuoglu B, Ozmenoglu M, Ozcan C, Gurhan H, Oral nifedipine in the treatment of hypertensive crises in patients with hypertensive encephalopathyInt J Cardiol 1992 34:277-82. [Google Scholar]
[9]. Diker E, Erturk S, Akgun G, Is sublingual nifedipine administration superior to oral administration in the active treatment of hypertension?Angiology 1992 43:477-81. [Google Scholar]
[10]. Furberg CD, Psaty BM, Meyer JV, Nifedipine. Dose-related increase in mortality in patients with coronary heart diseaseCirculation 1995 92(5):1326-31.Sep 1 [Google Scholar]
[11]. Levy JH, Treatment of perioperative hypertensionAnesthesiol Clin North Am 1999 17:569-70. [Google Scholar]
[12]. Samad A, Shareef M, Sublingual Nifedipine in Acute Hypertensive CrisisPak heart J 1983 16(3) [Google Scholar]
[13]. Nifediac package insert, TEVA Pharmaceuticals, Sellersville, Pennsylvania, August, 2009. [Google Scholar]
[14]. Baselt, Randall C. (2008). Disposition of Toxic Drugs and Chemicals in Man. Foster City, CA: Biomedical Publications. pp. 1108–1110. ISBN 0-9626523-7-7. [Google Scholar]
[15]. Hypertension: management of hypertension in adults in primary care. Clinical guideline CG34. National Institute for Health and Clinical Excellence (NICE), June 2006. Full text index. ISBN 1-86016-285-1. [Google Scholar]
[16]. Varon J, Marik PE, Clinical review: The management of hypertensive crisesCritical care (London, England) 2003 7(5):374-84. [Google Scholar]
[17]. Grossman E, Messerli FH, Grodzicki T, Kowey P, Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies?JAMA 1996 276(16):1328-31.Oct 23-30 [Google Scholar]
[18]. Walker JJ, Bonnar J, Dunlop W, Advances in the management of severe pre-eclampsia and anti-hypertensive therapyRecent Advances in Obstetrics and Gynaecology 1999 London, EnglandRoyal Society of Medicine Press Ltd.Vol 23. [Google Scholar]
[19]. Rubenstein E, Escalante C, Hypertensive crisisCrit Care Clin 1989 5:477-95. [Google Scholar]
[20]. Schillinger D, Nifedipine in hypertensive emergencies: a prospective studyJ Emerg Med 1987 5:463-73. [Google Scholar]
[21]. Cohan JA, Checcio LM, Nifedipine in the management of hypertensive emergencies: report of two cases and review of the literatureAm J Emerg Med 1985 3:524-30. [Google Scholar]
[22]. Kuwajima I, Ueda K, Kamata C, A study on the effects of nifedipine in hypertensive crises and severe hypertensionJpn Heart J 1978 19:45-67. [Google Scholar]
[23]. Beer N, Gallegos I, Cohen A, Klein N, Sonnenblick E, Frishman W, Efficacy of sublingual nifedipine in the acute treatment of systemic hypertensionChest 1981 79:571-74. [Google Scholar]
[24]. Bertel O, Conen D, Radü EW, Müller J, Lang C, Dubach UC, Nifedipine in hypertensive emergenciesBr Med J (Clin Res Ed) 1983 286(6358):19-21.January 1 [Google Scholar]