Secondary Chondrosarcoma of the Lumbosacral Region: Are any Bones Spared in the Multiple Hereditary Exostoses?
Hemalatha Anantharamaiah1, R Kalyani2, Harendra Kumar M.L.3, Manohar P.V.4
1 Assistant Professor, Department of Pathology, Sri Devaraj Urs Medical College, Tamaka, Kolar 563101, Karnataka, India.
2 Professor, Department of Pathology, Sri Devaraj Urs Medical College, Tamaka, Kolar 563101, Karnataka, India.
3 Professor & HOD, Department of Pathology, Sri Devaraj Urs Medical College, Tamaka, Kolar 563101, Karnataka, India.
4 Professor, Department of Orthopaedics, Sri Devaraj Urs Medical College, Tamaka, Kolar 563101, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hemalatha A., Assistant Professor, Department of Pathology, Sri Devaraj Urs Medical College, Tamaka, Kolar – 563101, India. Phone No: 9972212324 Email: drhemashashi@gmail.com
Osteochondromas are the most common benign bone tumors. Usually solitary, multiple osteochondromas (exostoses) are seen in patients with Multiple Hereditary Exostoses (MHE). Chondromatous transformation of lumbar osteochondroma in a patient with multiple exostoses is a rare phenomenon. We present a rare case of secondary chondrosarcoma of lumbar exostoses with patient presenting with symptoms of pain in the right lumbar region and paresis of right lower limb. Patients with multiple exostoses are prone to develop chondrosarcoma early in life. These patients need long term follow up with regular clinical and radiological examination.
Osteochondroma, Multiple Hereditary Exosostosis, Secondary Lumbar Chondrosarcoma
INTRODUCTION
An osteochondroma is a cartilage capped bony projection which arises on the external surface of the bone, which contains a marrow cavity that is continuous with that of the underlying bone. The diagnosis of multiple exostoses (Multiple Hereditary Exostoses - MHE) must be considered when at least 2 osteochondromas of the juxta – epiphyseal region of the long bones are seen. MHE is an autosomal dominant inherited trait with a male preponderance and an incidence of 1 in 50,000 [1]. Occasionaly, these osteochondromas may grow aggressively or they may reactivate into a secondary chondrosarcoma. A malignant transformation occurs in 0.5-5% of the cases [2]. The involvement of the spine in MHE is a rare phenomenon. 0.1% of the osteochondromas occur in spines, as was found in a study which was done by Porter et al. [3] A chondrosarcomatous transformation of the lumbar spinal osteochondromas is a very rare phenomenon.
CASE REPORT
First Admission
A 22 year old male presented with multiple swellings. He had these swellings since childhood. His presenting complaint were an increase in the size of the swelling which was there on his right low back since 3 months, weakness and an inability in walking by using the right lower limb since 1 week. The patient also had pain on the right side of the lower back since 1 week. None of his family members had similar swellings. The local examination revealed a diffuse swelling on the right lower back, which extended from T12 to L5. The neurological examination revealed a motor power of 3/5 in the right lower back. The provisional diagnosis was multiple exostoses with a lower motor neuron type of weakness in the right lower limb, which was secondary to the mass in the right paraspinal region.
THE LABORATORY INVESTIGATIONS
The relevant haematological and biochemical investigations were normal except alkaline phosphatase, which was 592 IU.
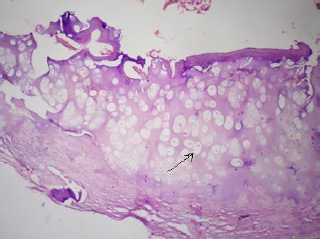
The radiological investigations (X-rays) of the dorsolumbar spine showed a bony growth with mature cortical bone and marrow with erosion of the cortex. The area of the erosion showed a mottled calcification. Ultrasonography of the mass showed exostoses which arose from the vertebrae, with calcification and compression of the right kidney. Fine needle aspiration cytology of the tumour showed the features of osteochondroma. The gross examination of the biopsy showed multiple bits of bone and cartilage, the largest measuring 2.5 x 1 x 0.5cms. The cut section was gritty. Microscopically, the section showed a mature, benign appearing, cartilaginous tissue [Table/Fig-1] with areas of ossification. Tumour cells with pleomorphic vesicular nuclei, which were arranged in sheets and lobules, were seen. At places, the lacunae showed more than two cells. Tumour giant cells with a high mitotic activity were seen. A histological diagnosis of osteochondroma with a malignancy was made. The patient was advised exicision, but he went home against medical advice.
Section studied shows chondrocytes with vacuolated cytoplasm H & E stain 100x
Second Admission
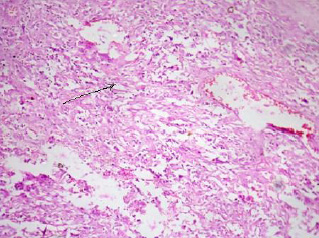
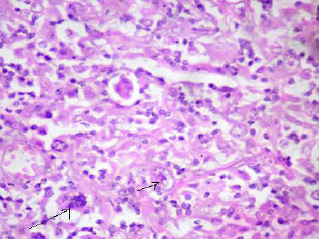
After 6 months, the patient presented with similar complaints. A provisional diagnosis of secondary chondrosarcoma – L3 L4 L5 was made. Per operatively, an ill-defined, highly friable mass with areas of necrosis and haemorrhage, which infiltrated into the soft tissue and which encroached L4 and L5 was seen. Only a biopsy was done, considering the marked local infiltration of the tumour. The biopsy showed an irregular, grey white to grey brown, friable, firm to hard tissue mass, which measured 2.5 x 1 x 0.5cms. The cut section was grey brown with areas of haemorrhage and necrosis, along with firm to hard areas and areas of cartilage. Microscopically, the tumour cells were found to be arranged in sheets. These cells were spindle shaped, with scanty cytoplasm [Table/Fig-2]. The nucleus was elongated hyperchromatic to vesicular with stippled chromatin. Binucleate and multinucleate forms were seen [Table/Fig-3]. Areas of haemorrhage and necrosis was seen. A histopathological diagnosis of chondrosarcoma, grade III, was made. The institutional ethical clearance was obtained for reporting this case.
Spindle shaped cells with scanty to moderate cytoplasm. H&E stain. 100x
Pleomorphic tumor cells with vesicular nucleus having stippled chromatin. Binucleate an multinucleate tumor cells seen. H & E stain 400x
The patient was lost for further follow up.
DISCUSSION
The first description of a patient of multiple hereditary exostoses was given by Hunter in his 1786 lectures on the principles of surgery [4]. Multiple hereditary exostoses has various synonyms such as diaphyseal aclasis, osteochondromatosis and multiple cartilaginous exostoses. A majority of the lesions are asymptomatic and they are located in the bones that develop from the cartilage, such as the long bones of the extremities around the knee joint, the pelvis and the trunk [1]. Being usually diagnosed in the first decade of life, the pain and the cosmetic deformities may be the main concerns for the patients [4]. The patients with the spine involvement tend to experience neurological deficits and myelopathy more frequently than the patients with solitary osteochondromas [2]. Our patient presented with pain and motor dysfunction of the right lower limb.
Numerous complications such as orthopaedic deformities and neurological and vascular complications have been described. The most dreaded of all the complications is the malignant transformation to secondary chondrosarcoma. The clinical signs of the malignant transformation include a sudden increase in the size of the tumour after puberty and pain [3]. An increase in the thickness of the cartilaginous cap of more than 1cm on X-rays should raise a suspicion of chondrosarcoma. Histologically, most of the patients have grade II chondrosarcoma [4]. Our patient presented with grade I chondrosarcoma. On the second admission, he developed grade III chondrosarcoma.
MHE is a familial neoplastic trait with a 2 hit model of patho genesis. A mutation of the EXT tumour suppressor gene was identified. The EXT1 mutation was seen in 40% of the patients. The EXT 2 mutation was seen in 40% of the patients and no mutation was seen in 15% of the patients. The diagnosis has to be confirmed after a mutational analysis of the genomic DNA which is extracted from blood or buccal swabs [1]. These studies could not be done in our patient, as he was lost for follow up. However, this patient could have had a sporadic mutation as his pedigree was normal.
The prognosis of secondary chondrosarcoma depends on its histological grade. The 10 year survival rates are 83% for chondrosarcoma grade I as compared to 29% for grade III. chondrosarcoma [5]. The involvement of the lumbar spine in multiple exosostos is rare. Only few cases of a chondromatous transformation of the lumbar exostoses have been reported [5].
A screening programme is recommended in patients with MHE, where the patients have to be followed up once in a year or two. A high index of suspicion is needed when the patient develops pain, a neurological deficit, and a sudden increase in the size of the swelling. Such patients have to undergo CT or MRI scans along with a biopsy of the swelling to rule out chondrosarcoma [2].
[1]. Bovée JV, Multiple osteochondromasOrphanet J Rare Dis 2008 3:3 [Google Scholar]
[2]. Porter DE, Lonie L, Fraser M, Dobson-Stone C, Porter JR, Monaco AP, Severity of the disease and the risk of a malignant change in hereditary multiple exostoses. A genotype-phenotype studyJ Bone Joint Surg 2004 86:1041-47. [Google Scholar]
[3]. Ahmed Refaat A, Tan Tai-Sheng MD, Unni K, Krishnan MB, A secondary chondrosarcoma in an osteochondroma: A report of 107 patientsClinical Orthop Related Res 2003 411:193-206. [Google Scholar]
[4]. Stieber JR, Dormans JP, The manifestations of hereditary multiple exostosesJ Am Acad Orthop Surg 2005 13(2):110-20. [Google Scholar]
[5]. Ali M, Firouz Ali Z Vahedi, The report of a rare case of multiple hereditary exostoses with vertebral and spinal cord compressions and a chondrosarcomatous differentiationNeurosurg. Q. 2007 17(1):29-32. [Google Scholar]