A Case of Flax Seed Induced Rhabdomyolysis
Anushre Prasad1, Ritesh Kumar2, Harini Ramanan3, Nalini Khandige4, Krishnananda Prabhu5
1 Assistant Professor, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India.
2 M.Sc Student, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India.
3 M.Sc Student, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India.
4 Additional Professor, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India.
5 Associate Professor, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Krishnananda Prabhu, Associate Professor, Department of Biochemistry, Kasturba Medical College, Manipal University, Manipal-576104, India. Fax: 91 0820 2571927
E-mail: krishnakunj2000@yahoo.com
Rhabdomyolysis is a clinical and a biochemical syndrome that occurs due to a skeletal muscle injury. The main cause of rhabdomyolysis is a muscle crush injury, toxins, ischaemia and metabolic disorders. Rare cases of rhabdomyolysis have been reported which had been caused by drugs and after insect stings. The breakdown products of the damaged muscle cells are released into the bloodstream; some of these, such as the protein myoglobin, are harmful for the kidneys and they may lead to kidney failure. The symptoms of rhabdomyolysis depend on the severity of the condition. The milder forms of rhabdomyolysis may not cause any muscle symptoms, and the diagnosis is based on abnormal blood tests. The most reliable test in the diagnosis of rhabdomyolysis is the blood level of Creatine Kinase (CK) which is released by the damaged muscles. Here in, we report an unusual case of flax seed induced rhabdomyolysis to alert the medical community about this rare complication.
Rhabdomyolysis, Acute renal failure, Flax seeds (Linum usitatissimum)
INTRODUCTION
Rhabdomyolysis is a clinical and a laboratory syndrome that is caused by various aetiologies and which involves the skeletal muscle. It is characterized by the leaking of myoglobin and other intracellular proteins and electrolytes into the circulation [1]. Acute renal failure occurs in 33-50% of the patients with rhabdomyolysis [2]. The main cause of rhabdomyolysis is a muscle crush injury which is caused by trauma, [3] excessive muscle activity [4], toxins, ischaemia, metabolic disorders, drugs [5], alcohol, cocaine and infections. However, the drug induced rhabdomyolysis is rare. But high doses of statins [6], Diabetes and hypothyroidism may cause rhabdomyolysis. Rare cases of rhabdomyolysis have been reported after insect stings [7] (ex-stings of wasps, bees and ants).
Here in, we report an unusual case of flax seed induced rhabdomyolysis to alert the medical community about this rare complication.
CASE
A 35 year old male was admitted to the Kasturba Medical College Hospital, Manipal University, Karnataka, India, which is a tertiary care hospital, with a history of generalized muscle pain and weakness of three days. He was a diabetic with hypertriglyceridaemia, who was on treatment for the past 2 years. He had not travelled recently and had not done strenuous exercises; there was no premorbid illness, chest pain, or abdominal pain and there was no relevant history which was suggestive of a muscle injury. He was a nonalcoholic and a nonsmoker and he had no history of kidney disorders. There was no family history of a muscle disease or kidney disorders. Since three months, he had stopped all the drugs which had been prescribed by his physician and at that time, his triglyceride level was 473 mg/dl. He had controlled his diet and had started taking flax seeds (Linum usitatissimum), approximately 6-10gm daily once in the morning after breakfast, since the past three months, to control his triglyceride levels. After 75 days, his triglyceride levels had come down to 148mg/dl.
At the time of admission, he had a pulse rate of 80 beats/minute, a blood-pressure of 160/90 mm Hg and a respiration rate of 16 breaths/minute and his arterial blood gas analysis was normal.
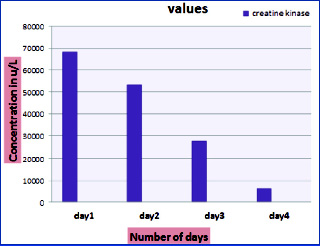
His laboratory data on admission included: urea - 17 mg/dl; creatinine - 0.9 mg/dl; total bilirubin - 0.4 mg/dl; direct bilirubin - 0.2 mg/dl; total protein - 7.8 g/dl; albumin - 4.8g/dl; globulin - 3.0 g/ dl; Aspartate Transaminase (AST) - 1564 u/l; Alanine Transaminase (ALT) - 424 u/l; Alkaline Phosphatase (ALP) - 61 u/l; Creatine Kinase (CK) - 61818 u/l and Creatine Kinase-MB (CK-MB) - 71 u/l. His urine myoglobin was positive and his urine protein was 1 +. The patient’s sample was negative for leptospirosis, hepatitis B and hepatitis C. Alkaline diuresis was started and his renal function, liver enzymes and creatine kinase were monitored during the hospital stay. At the time of his discharge, his renal function was normal; his creatine kinase was 6,244, his AST was 436 and his ALT was 418 units/l respectively. The patient was discharged as he felt symptomatically better and advised to report in two weeks [Table/Fig-1].
Shows serial estimation of creatine kinase levels
DISCUSSION
Rhabdomyolysis is a condition in which the damaged skeletal muscle tissue breaks down rapidly. The breakdown products of the damaged muscle cells are released into the bloodstream; some of these, such as the protein myoglobin, are harmful for the kidneys and may lead to kidney failure. The symptoms may include muscle pains, vomiting and confusion. The symptoms of rhabdomyolysis depend on the severity of the condition. The milder forms of rhabdomyolysis may not cause any muscle symptoms, and the diagnosis is based on abnormal blood tests. The most reliable test in the diagnosis of rhabdomyolysis is the blood level of Creatine Kinase (CK) which is released by the damaged muscle, and the levels above 5 times the Upper Limit of the Normal (ULN) levels indicate rhabdomyolysis [8,9].
Flax, which is also known as common flax or linseed (Linum usitatissimum), is a member of the genus, Linum in the family linaeceae. It is grown both for its seeds and its fibres. Flax seeds are the source of linseed oil, which is an edible oil. Flax seeds are a good source of dietary fibre, vitamins and minerals [10]. One hundred grams of flax seeds supply about 450 kcal; 41g of fat, 28g of fibre, and 20g of protein. Flax seeds have been shown to lower the serum cholesterol levels, especially in women [11] and they have been shown to have some benefits in the individuals with certain types of breast and ovarian cancers [12]. Due to its rich fibre content, it may be used as a laxative. Studies have shown that its lignan extract lowers the plasma cholesterol levels and the glucose concentrations in hypercholesterolaemic subjects. Its cholesterol lowering effect has not been clearly understood, but it has been suggested that lignans may lower the plasma cholesterol levels by modulating 7-alpha hydroxylase and acyl CoA cholesterol transferase, both of which are involved in the cholesterol metabolism. Lignans also increase the fatty acid oxidation and they downregulate the hepatic lipogenic enzymes; thereby, decreasing the fatty acid availability for the triacylglycerol synthesis and for the secretion from the liver [13]. In this case, the highly elevated creatine kinase values, along with the myoglobinuria in the absence of any muscle injury, pointed to the possibility of rhabdomyolysis. However, we could not comment on the marginally elevated liver enzymes. Some of the lipid lowering drugs have known to cause hepatotoxicity, myopathy and rhabdomyolysis, but the incidence of this is less than 0.1%. In this case, the creatine kinase level was more than 20 times the upper limit of the normal level, strongly suggesting that this was a case of rhabdomyolysis.
[1]. Pasqualetti G, Bini G, Tognini S, Polini A, Monzani F, Clarithromycininduced rhabdomyolysis: a case reportInt J Gen Med 2012 5:283-85. [Google Scholar]
[2]. Stella JJ, Shariff AH, Rhabdomyolysis in a recreational swimmerSingapore Med J. 2012 Feb 53(2):e42-4. [Google Scholar]
[3]. Alavi-Moghaddam M, Safari S, Najafi I, Hosseini M, Accuracy of the urine dipstick method in the detection of the patients who were at risk for crush-induced rhabdomyolysis and acute kidney injuryEur J Emerg Med 2011 Nov 11 [Epub ahead of print] [Google Scholar]
[4]. Kiberd M, Campbell S, Delayed-onset rhabdomyolysis after an intense exerciseCMAJ 2011 Nov 8 183(16):E1222 [Google Scholar]
[5]. Ramaiah R, Lollo L, Brannan D, Bhananker SM, The Propofol infusion syndrome in a super morbidly obese patient (BMI = 75)Int J Crit Illn Inj Sci 2011 Jan 1(1):84-86. [Google Scholar]
[6]. Abrams J, Tiu S, The reversal of drug-induced rhabdomyolysis on bone scansClin Nucl Med 2011 Aug 36(8):e101-02. [Google Scholar]
[7]. Almeida RA, Olivo TE, Mendes RP, Barraviera SR, Souza Ldo R, Martins JG, Hashimoto M, Fabris VE, Ferreira Junior RS, Barraviera B, Africanized honeybee stings: how to treat themRev Soc Bras Med Trop 2011 Nov-Dec 44(6):755-61. [Google Scholar]
[8]. Elsayed EF, Reilly RF, Rhabdomyolysis: a review, with emphasis on the pediatric populationPediatr Nephrol 2010 Jan 25(1):7-18. [Google Scholar]
[9]. Lima RS, da Silva Junior GB, Liborio AB, Daher Ede F, Acute kidney injury which was caused by rhabdomyolysisSaudi J Kidney Dis Transpl 2008 Sep 19(5):721-29. [Google Scholar]
[10]. Singh KK, Mridula D, Rehal J, Barnwal P, Flaxseed: a potential source of food, feed and fiberCrit Rev Food Sci Nutr. 2011 Mar 51(3):210-22. [Google Scholar]
[11]. Patade A, Devareddy L, Lucas EA, Korlagunta K, Daggy BP, Arjmandi BH, Flaxseed reduces the total and the LDL cholesterol concentrations in native American postmenopausal womenJ Womens Health (Larchmt) 2008 Apr 17(3):355-66. [Google Scholar]
[12]. Donaldson MS, Nutrition and cancer: a review of the evidence for an anti-cancer dietNutr J 2004 Oct 20 3-19. [Google Scholar]
[13]. Zhang W, Wang X, Liu Y, Tian H, Flickinger B, Empie MW, The dietary flaxseed lignan extract lowers the plasma cholesterol and the glucose concentrations in hypercholesterolaemic subjectsBr J Nutr. 2008 Jun 99(6):1301-09. [Google Scholar]