The Papillon Lefevre syndrome is an autosomal recessive disorder which is characterized by various dermatological manifestations and periodontitis as a manifestation of a systemic disease. Its aetiopathogenesis is thought to be secondary to the mutation of the Cathepsin C gene. Various studies have shown that the immune related cells like the polymorphonuclear leucocytes and the macrophages and their precursors were affected.
This report elicits about an edentulous male with this syndrome, who was treated with a modified complete denture prosthesis (hollow, maxillary, complete denture), considering his young age and low socioeconomic status.
INTRODUCTION
The Papillon Lefevre syndrome was first described by Papillon and Lefevre in 1924 [1]. The clinical manifestations include palmoplantar hyperkeratosis with a rapidly progressive periodontal disease that results in the premature exfoliation of both the dentitions [2].
The incidence of the Papillon lefevre syndrome is 1 to 4 per million, with no sex predilection. A genetic predisposition with a greater frequency of occurrence in consanguineous offsprings has been noted in approximately one-third of the cases. It manifests during the first 4 to 5 years of age, affecting the primary dentition with a periodontal involvement, leading to an early exfoliation of the primary dentition. As the permanent teeth erupt, the same sequence of events recurs, leading to the exfoliation of the same. Palmoplantar keratosis which varies from a mild psoriasiform scaly skin to overt hyperkeratosis is characteristic, which may also affect other sites such as the elbows and the knees [3].
Here, we are describing a case report of a young edentulous patient with the Papillon Lefevre syndrome, who was treated with a modified complete denture prosthesis.
CASE REPORT
A 25 year old, completely edentulous male patient of a low socioeconomic status, reported to the Department of Prosthodontics, Govt. Dental College and Hospital, for oral rehabilitation. His past dental history revealed that his deciduous teeth had erupted normally but that they had been exfoliated by the age of four years. All his permanent teeth had been lost by the age of 17 years, despite their normal eruptions. Some of his teeth were extracted by a local dentist as they had grade 3 mobility and because of the poor prognosis due to periodontitis, while the remaining teeth had got exfoliated by themselves, suggesting periodontitis, which in this case, was a manifestation of a systemic disease, which was the Papillon Lefevre syndrome. His family history was not significant, as the other members of his family were not affected by any such complaints of periodontitis or skin lesions, thus suggesting the sporadic nature of occurrence of his condition.
His physical examination showed symmetric, well demarcated, yellowish, keratotic, confluent plaques which affected the skin of his palms and soles [Table/Fig-1]. The plaques extended onto the dorsal surfaces, which had occurred at the age of three years and had progressed to the present state. The lesions would become worst during winter, with fissuring and bleeding.
Dermatologic manifestations in the form of hyperkeratosis of palms and soles

His intraoral examination showed completely edentulous upper and lower arches with resorption of the residual ridges [Table/Fig-2]. The mucosa and the salivary flow were normal. His panoramic radiograph showed completely edentulous upper and lower arches with a reduced alveolar bone height. His routine blood investigations and liver function tests like the serum transaminase levels, total bilirubins and alkaline phosphatase were carried out and they were found to be within the normal range.
Intra Oral View showing edentulous jaws

Based on his intra oral and extra oral findings, as well as his radiographic features, the diagnosis of the Papillon Lefevre syndrome was made. The patient was referred to a dermatologist for the treatment of his skin lesions. The dental treatment included a set of a hollow complete denture prosthesis with a modified technique, considering his young age, the residual alveolar ridge resorption that had already taken place and his low socioeconomic status.
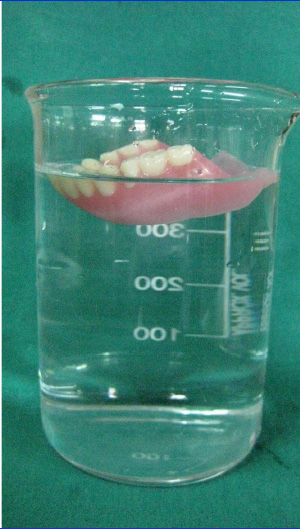
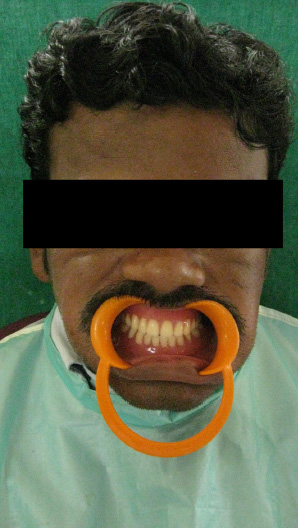
Selective pressure impressions were made by using a light body elastomeric impression material (Reprosil) [Table/Fig-3]. The vertical dimension of the occlusion was kept low. Due to the excessive ridge resorption, the monoplane and the narrow posterior teeth were selected. A hollow maxillary denture for the upper arch was planned, as it reduces the weight of the prosthesis by making the denture base hollow by using silicon putty as one of the weight reduction approaches [Table/Fig-4]. The complete maxillary and the mandibular dentures were delivered and the patient was recalled for a follow up and the necessary adjustments [Table/Fig-5].
Impressions taken with selective pressure impression technique

IHollow maxillary denture using silicone putty as a weight reduction approach
Patient with specially modified complete dentures
DISCUSSION
The Papillon Lefevre syndrome was originally described by 2 French physicians, Papillon and Lefevre in 1924. This syndrome is inherited as an autosomal recessive trait with a prevalence of 1 to 4 cases per million [1].
The precise aetiopathogenesis of the Papillon lefevre syndrome is vague; several authors have proposed immunologic, microbiologic, and genetic causes for this syndrome. The causative organisms which have been demonstrated in this syndrome are Actinobacillus actinomycetemcomitans, Porphyromonas gingivalis, Fusobacterium nucleatum and Treponema denticola. A neutrophil dysfunction in the form of decreased chemotactic and phagocytic activities has also been suggested. Recent studies have suggested that the inactivation of the cathepsin C gene was responsible for the skin and the dental abnormalities of this syndrome. Hence, the treatment of this syndrome is very difficult [1].
This disorder is characterized by palmoplantar hyperkeratosis with severe early onset periodontitis, premature loss of the primary and the permanent teeth and hyperkeratosis of the elbow and the knee [2].
In the present case, the dermatological findings and the history strongly suggested it to be the Papillon Lefevre syndrome. Although the physical characteristics of the patient were typically suggestive of the Papillon Lefevre syndrome, the laboratory findings of the blood picture and the liver function tests were not altered [2].
The differential diagnosis of this syndrome includes acrodynia, hypophosphatasia, and cyclic neutropaenia. It differs from acrodynia or mercury poisoning by the presence of erythocyanosis, insomnia, muscle pain, tachycardia, psychic disturbances, and teeth erupting, prematurely with dystrophic enamel. The clinical features of knock-knee, bowing of the femur and the tibia, enlarged wrists, hypoplastic teeth and increased amounts of phosphoethanolamine in the urine differentiates hypophosphatasia from this syndrome. In cyclic neutropaenia, the palmoplantar hyperkeratosis is absent. The other conditions that can be included in the differential diagnosis are the Howel-Evans syndrome, Greither’s syndrome and keratosis punctata. Even though all these entities are associated with palmoplantar hyperkeratosis, periodontopathy is not seen in them [2].
The treatment planning of this syndrome should include a team of dermatologists and dental surgeons. Oral retinoids like acitretin, etretinate, and isotretinoin are used to treat both the cutaneous and the dental defects in the Papillon-Lefevre syndrome [2].
The review of the literature showed that certain modifications were necessary during the fabrication of the complete denture prosthesis in the patients with the Papillon Lefevre syndrome. The various modifications which were used during the fabrication of the complete dentures were the use of selective pressure impressions, keeping the vertical dimension of the occlusion low and the use of a monoplane and the narrow posterior teeth and a hollow maxillary denture for the upper arch [4–9]. The prosthodontic management strategy for young edentulous patients in general, must include the preservation of the alveolar ridge, preferably by using an implant prosthesis [10–13]. However, the rehabilitation by using implants could not be employed due to the financial constraints in the present case. Instead, a conventional complete denture was planned with modifications, such as the use of the selective pressure impression technique, a low vertical dimension at the occlusion, narrow posterior teeth, a balanced occlusion and a hollow maxillary denture by using a silicone putty as a weight reduction approach [4,8,9]. The complete maxillary and mandibular dentures were delivered to the patient and post insertion instructions were given. The patient was advised recall visits to make the necessary adjustments. A follow-up was done for one year at 3 monthly intervals and it revealed that the patient did not have any problem with the dentures, that the ridge resorption was minimal with moderate retention and that the patient was able to eat both solid and liquid foods.
The reports on the cases of the Papillon Lefevre syndrome in the daily prosthodontic practice are rare and one should keep this disorder in mind whenever young edentulous patients are encountered.
CONCLUSION
The Papillon lefevre syndrome debilitates the patient socially and psychologically and also his/her aesthetic well being at a very young age, due to the associated cutaneous involvement and the partial or complete edentulism. Thus, an oral rehabilitation in such patients may play a very important role. An initial prosthetic replacement with a complete or a partial denture is necessary, with a future consideration for an implant supported prosthesis.
[1]. Singla A, Sheikh S, Jindal SK, Brar R, The Papillon Lefevre syndrome: a bridge between a dermatologist and a dentistJ Clin Exp Dent. 2010 2(1):e43-46. [Google Scholar]
[2]. Nagaveni NB, Suma R, Shashikiran ND, Subba Reddy VV, The Papillon-Lefevre syndrome: a report of two cases in the same familyJ Indian Soc Pedod Prev Dent. 2008 26:78-81. [Google Scholar]
[3]. Hattab FN, Rawashdeh MA, Yassin OM, Al-Momani AS, Al-Ubosi MM, The Papillon-Lefevre syndrome: A review of the literature and a report of 4 casesJ Periodontol. 1955 66:413-20. [Google Scholar]
[4]. Mallik CN, Gaurav R, The distal extension impression technique (an impression technique for distal extension in removable partial dentures)Archives of Dental Sciences 2010 1(1):84-86. [Google Scholar]
[5]. Kimoto S, Gunji A, Yamakawa A, A prospective clinical trial which compared a lingualized occlusion to a bilateral balanced occlusion in complete dentures: a pilot studyInt J Prosthodont. 2006 19:103-09. [Google Scholar]
[6]. Yoneyama Y, Tojyo T, Ohkubo C, Hosoi T, The pressure distribution in a mandibular complete denture with the use of soft lining materialsInt Chin J Dent. 2010 10:17-21. [Google Scholar]
[7]. Luthra RP, Gupta R, Vashisht D, Sharma N, Gupta R, An unemployed residual ridgeIndian Journal of Dental Sciences 2011 1(3):4-5. [Google Scholar]
[8]. Holt RA Jr, A hollow complete lower dentureJ Prosthet Dent. 1981 45:452-54. [Google Scholar]
[9]. Jhanji A, Stevens ST, The fabrication of one-piece hollow obturatorsJ Prosthet Dent. 1991 66:136-38. [Google Scholar]
[10]. Hegde R, Reddy R, The Papillon-Lefevre syndrome: A report of two casesJ.Indian Soc. Pedo. Dent. 2002 20(1):9-11. [Google Scholar]
[11]. Uelbro C, Crossner CG, Leindgren T, Stalblad PA, Renvert S, Osseointegrated implants in a patient with the Papillon-Lefevre syndrome A 4 ½ year follow upJ Clin Periodontal. 2000 27:951-54. [Google Scholar]
[12]. Osman EA, Murat U, Bulent K, The treatment of a patient with the Papillon-Lefevre Syndrome by using short dental implants: A case reportImplant Dentistry 2010 19(5):394-99. [Google Scholar]
[13]. Woo I, Brunner DP, Yamashita D-DR, Le BT, Dental implants in a young patient with the Papillon-Lefevre syndrome: A case reportImplant Dentistry 2003 12(2):140-44. [Google Scholar]