Dens Invaginatus (DI) is a rare developmental anomaly which affects the tooth, which shows an infolding of enamel and dentine which extends into the pulp chamber and sometimes into the root. The aim of this case report was to describe its radiographic findings, to emphasize the bizarre morphology and the difficulties which are encountered in the diagnosis by using conventional radiographic techniques and the importance of computed tomography as a valuable diagnostic aid. Dens Invaginatus is clinically significant due to the possibility of an early pulpal involvement and the chronic periapical lesions are often associated with this anomaly without any clinical symptoms. Difficulties are encountered during the endodontic treatment, owing to the complex root canal anatomy; therefore, a proper radiologic evaluation by using different imaging modalities, is essential for its successful treatment.
Introduction
Dens invaginatus or Dens in dente is a rare developmental anomaly of the calcified dental tissues, in which the enamel and the dentine invaginate inside the pulp. This invaginatus may be limited to the pulp chamber or it may extend up to the root apex. This is also known as ‘tooth within a tooth’ and it has a tendency of early pulpal necrosis and subsequent periapical pathoses. However, due to the complex root canal anatomy in this anomalous tooth, an endodontic treatment is difficult, especially when conventional radiography is used. Hence, we advocated the use of a 3 dimensional computed tomography scan, like a small Field of View (FOV) Cone Beam CT for the selected cases which were otherwise difficult to treat [1].
Case Report
A 42 year old woman reported to the dental hospital with the complaint of pain and swelling in the anterior maxillary region since the past 4 days. Her history revealed that she had a similar painful swelling in the same region 2 years back, which had subsided on medication. On examination, a diffuse extra-oral swelling was seen in the right maxillary anterior region, which was seen to obliterate the nasolabial sulcus. Intra-orally, a thick bulbous maxillary right lateral incisor with a shallow central groove was seen, without any clinical sign of dental caries, with a well circumscribed swelling in the periapical region, which obliterated the labial vestibule. The swelling was soft and fluctuant in consistency and tender on palpation. The tooth was tender to vertical percussion, slightly extruded from the socket and had grade II mobility. The Electric Pulp vitality tests elicited no response.
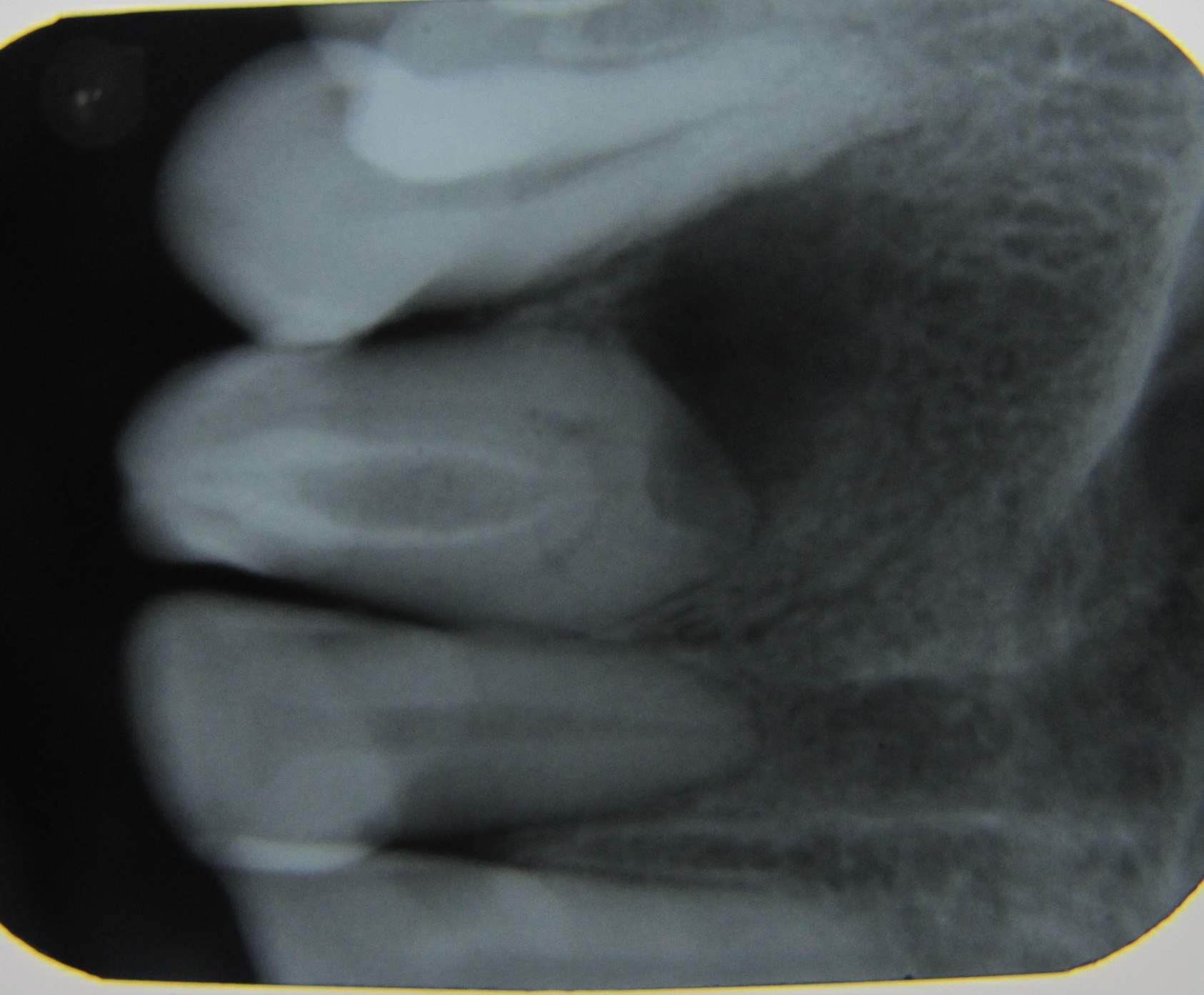
A periapical radiograph revealed the presence of a radiopaque invagination inside the pulp chamber which extended till the root apex, with a large radiolucent pulp space in it. Around the radiopaque invagination, radiolucent lines which were suggestive of root canals were seen both mesially, as well as distally. The entire root appeared bulbous and enlarged; the root apex could not be appreciated and there was the presence of an ill-defined, periapical radiolucency [Table/Fig-1] which was suggestive of an Oehler’s Type III B dens Invaginatus with a dento-alveolar abscess. An endodontic treatment could not be carried out since the patient did not wish to keep the mobile and painful tooth. However, the tooth specimen was kept for further analysis.
Intra-oral periapical radiograph of maxillary right side showing presence of a radiopaque invagination of the enamel and dentine extending till the root apex with a large radiolucent pulp space in it with periapical rarefaction.
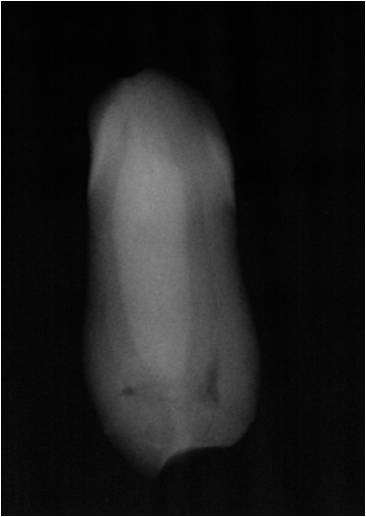
A file was inserted through the apical foramen of the extracted tooth specimen and it was ensured that it reached till the crown. Since the pulp chamber and the root canal anatomy could not be properly appreciated by conventional radiography, a non-ionic iodine based contrast media, “Omnipaque” was infused through the apical foramen and then radiographs were taken, with the tooth specimen being placed at different angles on the film. It was seen that the pulp space in the invaginated portion of the tooth had turned radiopaque, but that the radiolucent lines around the radiopaque invagination still remained, showing that the pulp spaces of the tooth and that of the invagination were not in contact with each other [Table/Fig-2].
The extracted tooth specimen on infusion of radiopaque contrast media showing that the pulp space of the invagination (radiopaque) not communicationg with pulp spaces (radiolucent lines) of the tooth.
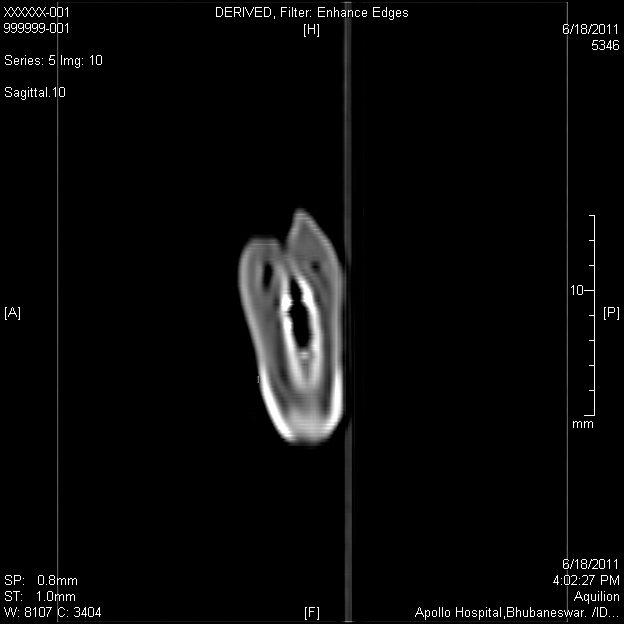
Since a 2-dimensional imaging could not provide a proper understanding of the root canal morphology, a helical Computed Tomography (CT) scan was done and the tooth was imaged in the different planes to evaluate the type of invagination and the root canal morphology. As it was an extracted tooth specimen, a helical CT scan was performed. It was observed that the hyperdense enamel had invaginated inside the pulp space and that it had extended deep inside the root till the apex [Table/Fig-3]. The enamel of the invaginatus was more hyperdense than the enamel and the dentine of the crown [Table/Fig-4]. The CT numbers or the Hounsefield units of the normal enamel and the dentine i.e. of the tooth were 2000 and 1200 respectively, while those of the invagination were 4000. This unique finding in the CT prompted us to submit the tooth for a histologic evaluation.
C.T. scan of the tooth specimen coronal view showing hyperdense enamel invaginated inside the pulp space extending deep inside the root till the apex and the pulp spaces of the invagination and that of the tooth are not communicating with each other.
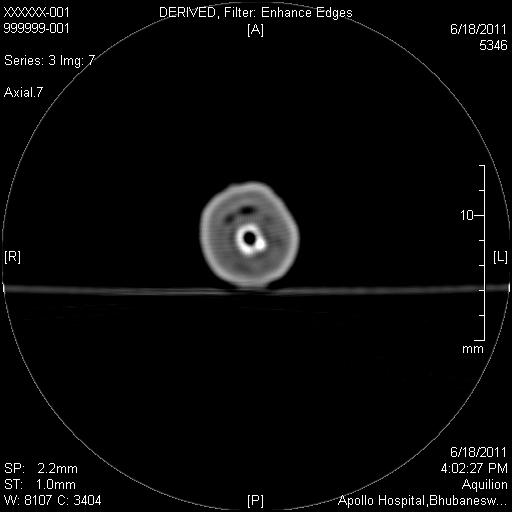
C.T. scan of the tooth specimen axial view showing two concentric hyperdense rings, the outer tooth enamel and the inner invaginated enamel, also that the invaginated enamel is hyperdense compared to that of the tooth.
The tooth was sectioned longitudinally into 2 equal halves [Table/Fig-5], one half was decalcified and a hematoxylin-eosin stained section was prepared; the other half was sectioned by using a hard tissue microtome and a ground section was obtained.
Tooth specimen showing necrotic pulp, layer of dentine sandwiched between two layers of enamel.

The ground section revealed a layer of dentine which was sandwiched between 2 layers of enamel. The outer enamel covering showed straight, parallel running enamel rods, predominantly at the middle and the cervical thirds. At the incisal third, however, the course of the enamel rods was wavy and tortuous and it appeared as gnarled enamel. Few enamel tufts and enamel lamellae were present at the Dentinoenamel Junction (DEJ) and at the surface of the enamel respectively. The incremental lines of Retzius were not so obvious. One of the characteristic features was that the absence of a single layered, scalloped DEJ, rather than that of a multi layered, fish scale like DEJ was seen [Table/Fig-6].
Ground section of tooth showing multiple layered, fish scale like dentinoenamel junction between outer enamel layer and dentin (100X)
The dentine appeared to be normal in most of the coronal and the middle third, showing the normal S-shaped curvature of the dentinal tubules. However, dead tracts were present abundantly throughout, indicating empty dentinal tubules, thereby implying dead odontoblasts. But the apical third of the dentine showed more amounts of interglobular dentine and globular dentine areas, suggesting a defect in the normal mineralization process of the dentine. Many accessory pulp spaces, along with projecting accessory lateral canals, were also evident. A few pulp spaces which were surrounded by enamel appearing tissues were seen, which were indicative of a severe disturbance during the odontogenesis. The arrangement of the dentinal tubules was more haphazard at the apical third portion, again relating to a delayed defect in the dentinogenesis. The Tome’s granular layer was seen close to the cement-dentinal junction. The cementum appeared to be normal and it contained incremental lines of salter and many cementocytes which were embedded in the lacunae.
The inner invaginated enamel showed irregularly arranged enamel rods with no striae of Retzius and many focal areas showed the criss cross appearance of the rods. The inner invaginated enamel appeared hypomineralized. A definite DEJ which separated the dentine and the invaginated enamel was absent.
Discussion
Dens invaginatus or Dens in dente is a rare developmental dental anomaly which was first reported by Baume in 1874. The exact cause of this anomaly is still unknown, though a proposed aetiology is focal growth retardation/stimulation in or localized external pressure on some areas of the tooth bud, resulting in an infolding of the enamel organ into the dental papilla during the morphodifferentiation, prior to the calcification. The most extreme form of this anomaly is referred to as a ’dilated odontome’. It occurs with a frequency of about 0.04–10% [2, 3]. There is a 3:1 female predilection. DI commonly affects the maxillary lateral incisors. It also affects the central incisors, premolars, canines, and the molars in the decreasing order of the frequency. Sometimes, even a bilateral occurrence is seen and it may be associated with other dental anomalies [4]. The malformation shows a broad spectrum of morphologic variations and it often results in an early pulp necrosis if it is left undiagnosed and hence untreated.
Although a clinical examination may reveal a deep pit or a fissure on the lingual surfaces of the anterior teeth, a radiographic examination is the gold standard for the diagnosis of DI. The classic radiographic appearance of the coronal DI is a pear shaped invagination of the enamel and the dentine, with a narrow constriction at the opening on the surface of the tooth. The DI closely approximates the pulp chamber. The infolding of the enamel lining is more radiopaque than the surrounding tooth structure and it can be identified easily, as was seen in our case. If the coronal invagination is extensive, the crown is almost always malformed [5].
Oehlers et al., grouped the coronal DI into 3 types according to their radiographic appearances: (1) those invaginations that are enamel lined and confined within the crown of the tooth; (2) those that extend towards the root but do not cross the cemento-enamel junction; and (3) those that penetrate the surface of the root and ’burst’ apically or laterally to produce a second foramen in the root.
In the conventional radiographs, it is not always possible to determine, with great precision, the relationship between the invaginated portion of the tooth with the chamber and/or the root canals. In the present case, the tomographic images made it possible to observe an invagination which was communicating with the periodontal space, resulting in a large periapical lesion, which permitted us to classify the condition as type III DI [6].There was a bulbous root, but there was the presence of a single apical foramen. Though conventional radiography has been used for the diagnosis of DI in the past; however, the recent cases have been imaged with the help of CT, thus emphasizing the importance of the 3D imaging for unusual tooth anatomies. The tomographic images also make it possible to determine whether the invagination was communicating with the periodontal ligament space [7]. We are the first to report about the unusually hyperdense enamel of the invagination, and there was no histologic correlation for it.
Few of the histologic findings of the present case were in accordance with the findings of A. Piattelli and P. Trisi [8]. But in our case, we also observed a multiple layered, fish scale like DEJ, numerous pulp spaces which were lined by an enamel like tissue and a hypomineralized globular and a granular dentine at the apical third of the root. All these features were unique to the present case.
The management of DI with pulpal or periapical pathoses generally involves periapical surgery with a retrograde filling and because of the irregular anatomy and the limited access, the complete debridement of the root canal system seems impossible [9].However, even the conventional conservative endodontic therapy has been successfully performed in many cases [10,11].
Conclusion
It is essential that the dental surgeons be aware of this anomaly when they are presented with a case of pulpitis or periapical lesions, in the absence of any history of trauma or a clinical evidence of caries or restorations. The diagnostic pitfalls in the conventional radiography ought to be kept in mind and a CT scan, preferably a small Field of View (FOV) Cone Beam CT, can not only help in the diagnosis but it can also serve as an important aid in the treatment planning and in ensuring successful results. The root canal therapy may present severe problems in the cleaning and shaping, because of the complex anatomy of the teeth, as in our case.
[1]. Vier-Pelisser FV, Pelisser A, Recuero LC, Só MV, Borba MG, Figueiredo JA, The use of cone beam computed tomography in the diagnosis, planning and the follow up of a type III Dens invaginatus caseInt Endod J 2012 45:198-208. [Google Scholar]
[2]. Alani A, Bishop K, Dens invaginatus. Part 1: classification, prevalence and aetiologyInt Endod J 2008 41:1123-36. [Google Scholar]
[3]. Hülsmann M, Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerationsInt Endod J 1997 30:79-90. [Google Scholar]
[4]. Nallapati S, Dens invaginatus on a geminated tooth: A case ReportJ Endod 2004 30(10):726-31. [Google Scholar]
[5]. Alani A, Bishop K, Dens invaginatus. Part 2: Clinical and radiographic features and management optionsInt Endod J 2008 41:1123-36. [Google Scholar]
[6]. Neves FS, Bastos LC, Almeida SM, Norberto F, Dens invaginatus: a cone beam computed tomography case reportJ Health Sci Inst. 2010 28(3):249-50. [Google Scholar]
[7]. Kaneko T, Sakaue H, Okiji T, Suda H, The clinical management of Dens invaginatus in a maxillary lateral incisor with the aid of conebeam computed tomography – a case reportDental Traumatology 2011 27:478-83. [Google Scholar]
[8]. Piattelli A, Trisi P, Dens invaginatus: a histological study of undermineralized materialEndod Dent Traumatol 1993 9:191-95. [Google Scholar]
[9]. Silberman A, Cohenca N, Simon JH, An anatomical redesign for the treatment of Dens invaginatus type III with open apexes: A literature review and a case presentationJ Am Dent Assoc 2006 137:180-85. [Google Scholar]
[10]. Shadmehr E, Farhad AR, The clinical management of Dens invaginatus type 3: A case reportIranian Endodontic Journal 2011 6:129-32. [Google Scholar]
[11]. Monteiro-Jardel CC, Alves FRF, Type III Dens invaginatus in a mandibular incisor: A case report of a conventional endodontic treatmentOral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology 2011 111:e29-e32. [Google Scholar]