A Rare Case of a Giant Epidermoid Cyst of the Ovary
Nidhi Sharma1, Manimekalai2, Sulochana Sonti3, Meenakshisundarum4
1 Department of Gynecology,
2 Department of Gynecology,
3 Department of Pathology,
4 Department of Pathology Saveetha Medical College,No.162 Poonamalle High Road , Tamil nadu PIN 600042, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nidhi Sharma, Department of Gynecology, No 5 Jayanthi street, Seethapathy Nagar Velachery, Chennai, Tamil nadu PIN 600042, India.
Phone: 919445560392
E-mail: drbonuramkumar@yahoo.co.in
Epidermoid cysts of the ovary are rare benign lesions and they are usually an incidental finding in hysterectomy specimens. We are presenting the largest reported case of an epidermoid cyst of the ovary which measured 17x10x10 cm, in a 50 year old lady with a preoperative diagnosis of a fibroid uterus.
Epidermoid cyst, Monodermal teratoma, Surface epithelial ovarian tumour
Introduction
Epidermoid cysts of the ovary are exceptionally rare benign lesions [1,2] which are filled with flakes of keratin and are lined exclusively by mature, stratified, squamous epithelium. They differ from mature cystic teratomas of the ovary by the absence of hair follicles and sebaceous glands after a thorough sampling.
The possibility that some of these lesions are surface epithelial ovarian tumours, cannot be totally discounted. Several cases of epidermoid cysts of the ovary have been reported in the literature, but none of them were giant epidermoid cysts. Some authors have cited epidermoid cysts occurring in combination with surface epithelial ovarian tumours [3]. One case of epidermoid has been described in combination with a monodermal teratoma [4].
Case Report
A 50 year old, postmenopausal lady presented with the complaint of a gradual and a painless abdominal distension for the past six months. She had attained menopause 7 years ago. She had no history of vomiting, diarrhoea, dysuria or fever. She had no history of menorrhagia or dysmenorrhoea in her previous menstrual cycles. Ultrasonography of the pelvis and the abdomen revealed that she had a large degenerated fibroid in the posterior wall of the uterus, which measured 17x10 cm. The ovaries could not be visualized. Computed tomography of the abdomen and the pelvis was suggestive of a posterior wall uterine fibroid with degeneration.
She was taken up for an elective hysterectomy with the diagnosis of a degenerating fibroid uterus. An infraumblical midline laparotomy incision was made. Intraoperatively, the uterus and the right ovary were unremarkable and a large cyst was seen, which had adhered to the posterior surface of the uterus.
The left ovary and tube could not be defined. The patient underwent total abdominal hysterectomy, right salpingo-oopherectomy and cystectomy. The specimen was sent for a histopathological examination.
The gross examinations of the uterus and the cervix were unremarkable. The posterior surface of the uterus was covered with white flakes [Table/Fig-1].
Gross histopathological features of cut open uterus specimen

The cut open cyst measured 17x10x10 cm [Table/Fig-2]. The walls were thickened. The external surface was smooth. The internal surface was covered with white flakes of keratin. There were no septations. There were no solid areas or papillary projections. Hair follicles were not seen.
Gross histopathogical features of cut open epidermoid cyst of left ovary showing outer and inner surface

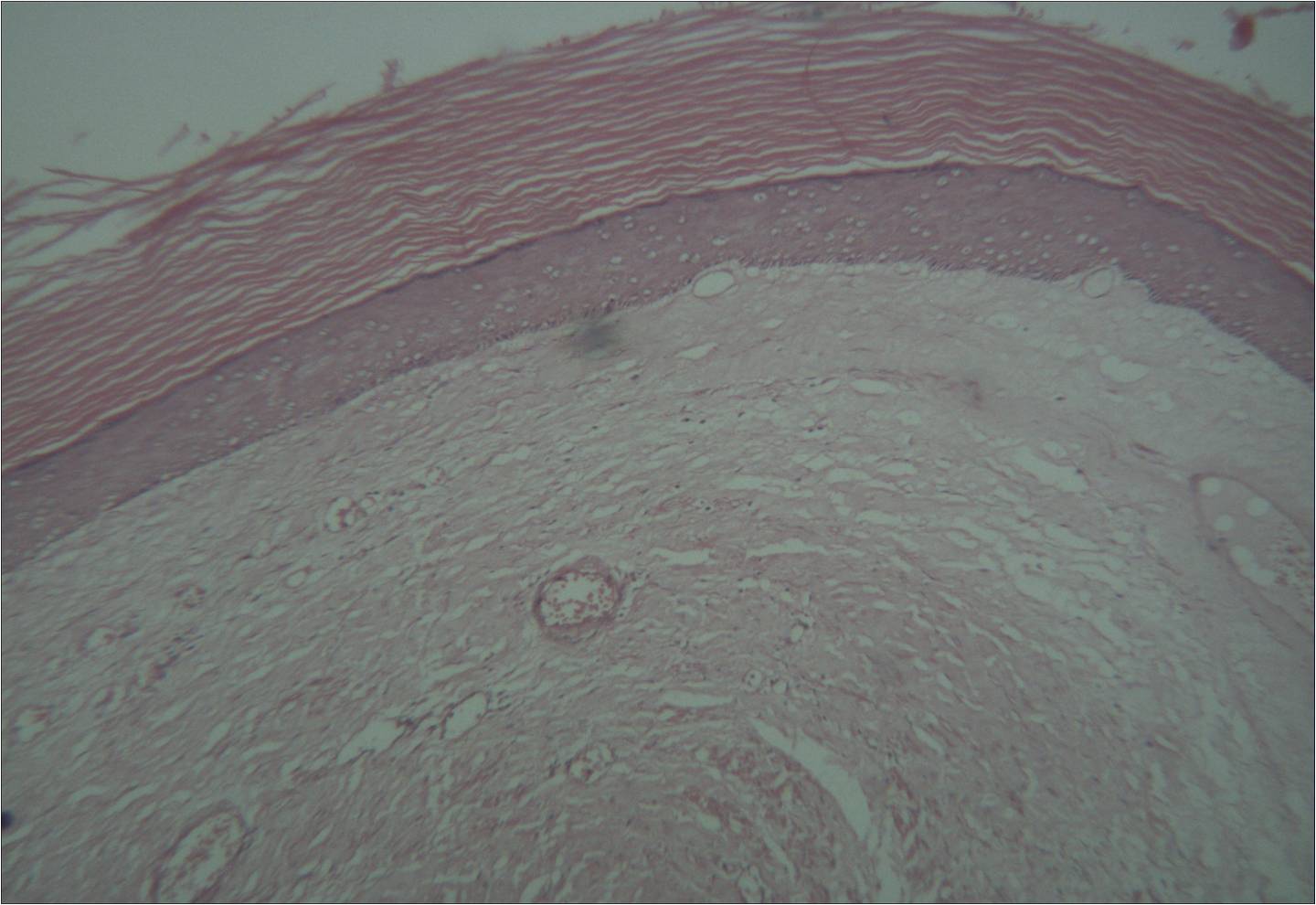
Microscopically, the fibrous wall of the cyst was lined with stratified, squamous epithelium with flakes of keratin. No hair follicles or sebaceous glands were seen after an extensive sampling [Table/Fig-3]. Based on these histological findings, a diagnosis of giant epidermoid cyst of the ovary was made.
Microscopic histopathology of the epidermoid cyst wall showing stratified squamous epithelium and flakes of keratin
Discussion
Epidermoid cyst of the ovary is an uncommon lesion and it is usually an incidental finding in the study of hysterectomy specimens. Young and Scully described three cases in 1980. They made a comparative study of the epidermoid cysts and the epithelial components of Brenner tumours. They suggested that epidermoid cysts originate from epithelial cell nests of the type encountered in Brenner tumors [1].
Peters et al., reported an epidermoid cyst of the ovary in combination with a well differentiated endometroid carcinoma of the ovary [3]. The carcinoma had the foci of squamous metaplasia, but there was no continuity between the wall of the epidermoid cyst and the squamous metaplasia of the carcinoma. While some authors had reported cases of epidermoid in association with epithelial tumours, Azena et al., described a case in combination with a germ cell tumour of the ovary [4]. Fan et al., in their series of eight cases ,suggested that ovarian epidermoid cysts represented monodermal teratomas and should be classified as such [5]. They also believed that epidermoid cyst is not as rare as the literature suggests and some are probably misdiagnosed as dermoid cysts.
Khedmati F et al., conducted the largest clinicopathological study on 18 cases of epidermoid cysts in comparison to 120 mature cystic teratomas in 2009 [6]. The authors had concluded that an epidermoid cyst of the ovary as defined by histology, was a heterogeneous group .A pure epidermoid cyst probably represents less than 1% of the ovarian epithelial tumours.
The mean tumour size was 1.75 cm. Here, we are presenting the largest reported case of an epidermoid cyst of the ovary, which measured 17x10cm. The pre-operative assessment of the patient was not suggestive of an ovarian pathology.
However, to our surprise, laparotomy did not reveal any obvious uterine pathology. We noted a giant, left ovarian cyst which was adhered to the posterior wall of the uterus, which was confirmed by histopathological studies. If the diagnosis of the ovarian cyst was possible preoperatively, we would have screened the patient for a potential ovarian malignancy and planned for a staging laparotomy. The clue to the preoperative diagnosis of the ovarian pathology was in our patient’s history, which was inadvertently overlooked ! She had no past menstrual complaints which were suggestive of a uterine fibroid.
Epithelial ovarian tumours are derived from tissues that come from the coelomic epithelium or the mesothelium [7]. The cells are a product of the primitive mesoderm, which can undergo metaplasia. Each tumour type represents a histological pattern that resembles the mucosal features of a section of the lower genital tract [8].
The epidermoid tumour can be a variant of an epithelial ovarian tumour, where the primitive mesoderm has undergone a metaplastic transformation to the stratified squamous epithelium. This is histologically identical to the vaginal mucosa.
Conclusion
Giant epidermoid cyst of the ovary is an extremely rare tumour. The diagnosis of an epidermoid ovarian cyst is often a surprise histopathological finding. One should be aware of the possibility of misinterpreting a cystic ovarian lesion as a degenerated uterine fibroid.
The clue to the diagnosis of the ovarian pathology often lies in the menstrual history of the patient, which can sometimes be inadvertently overlooked on the basis of ultrasonography and computed tomography imaging.
The diagnosis of an epidermoid cyst should only be made only after an extensive sampling has been done. The presence of hair follicles and sebaceous glands should be ruled out, to differentiate it from a dermoid cyst.
[1]. Young RH, Prat J, Scully RE, Epidermoid cyst of ovary: A report of three cases with comments on histogenesisAm J Clin Pathol 1980 73:273-76. [Google Scholar]
[2]. Juan Rosai, Rosai and Ackerman’s surgical pathology9th edition. Ovary; Epidermoid cyst:1689-90. [Google Scholar]
[3]. Peters K, Gassel AM, Muller T, Dietl J, Ovarian epidermoid cyst and endometrial carcinoma: do they share their origin?Zentralbi Gynaecol 2002 124:443-45. [Google Scholar]
[4]. Azena A, Zannol M, Bertezzol Ovarian epidermoid cyst of eight cases with comparison to mature cystic teratomasInt J Gynaecol pathol 1996 15:69-71. [Google Scholar]
[5]. Fan LD, Zang HY, Zhang XS, Ovarian epidermoid cyst of eight casesInt.J Gynaecol Pathol 1996 15:69-71. [Google Scholar]
[6]. Khedmati F, Chirolas C, Seidman JD, Ovarian and para ovarian squamous lined cysts(epidermoid cysts):a clinicopathological study of 18 cases with comparison to mature cystic teratomasInt J of Gynecol Pathol 2009 Mar 28(2):193-96. [Google Scholar]
[7]. Scully RE, Young RH, Clement PB, Tumors of ovary, maldeveloped gonads, fallopian tubes and broad ligamentIn Atlas of tumor pathology. Washington: Armed force institute of pathology 1998 Fascicle 23(3rd series) [Google Scholar]
[8]. Berek JS, Hacker NF, Practical Gynaecol oncology 2000 3rd edPhiladelphiaLippincott Williams and Wilkins:3-38. [Google Scholar]