A Rare Case of Cockayne Syndrome-MRI Features
Praveen Mundaganur1
1 Assistant Professor, Department of Radiology, BLDE Medical College and Research InstituteBijapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Praveen Mundaganur Assistant Professor, Department of Radiology, BLDE Medical College and Research Institute Bijapur- Karnataka - 586103 ,India.
Phone: 09916278706
E-mail: praveen_mdrd@yahoo.com
The Cockayne Syndrome is a rare syndrome of congenital originwhich is charcterized by growth retardation, facial dysmorphism, facial naevi,retinopathy and mental retardation, which are associated with the changes in the brain parenchyma. The findings of MRI of the brain support the clinical diagnosis of the Cockayne Syndrome. We would like to highlight the MRI findings of this rare syndrome.
Cockayne syndrome, Radiology, Brain
Case Report
A 17 year old male presented with facial dysmorphism, seizures,mental retardation, hyperpigmentation of the skin which is over the face and neck, bilateral congenital talipes equinovarus deformity of the feet and photophobia.
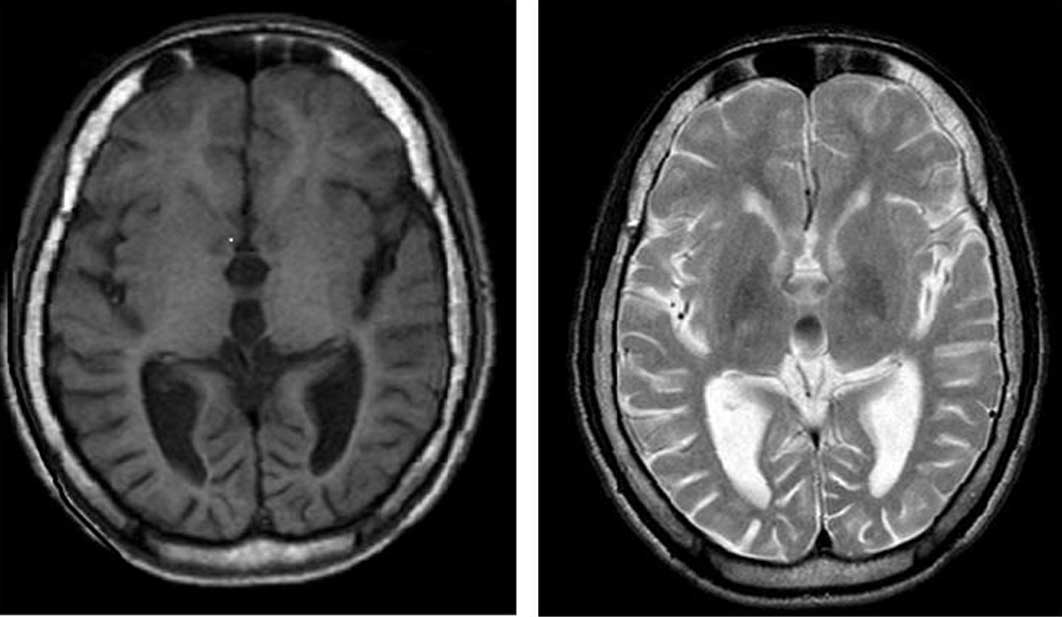
Audiometry and fundoscopic examinations revealed moderate sensory neural hearing loss and atypical retinitis pigmentosa. Then, the patient was subjected to an MRI study. The MRI of the brain, without a contrast study, showed generalized severe cerebral and cerebellar atrophies with widened sulci and an enlarged fourth ventricle, soft calcification of the bilateral basal ganglia and thinning of the brain stem, which are the classical features of Cockayne Syndrome. The MRI and the classical Ccinical features helped in arriving at the diagnosis of the Cockayne Syndrome [Table/Fig-1,2 & 3].
T1 and T2WI axial images showing diffuse cerebral atrophy with prominence of ventricular system. t2WI shows soft calcification of basal ganglia.
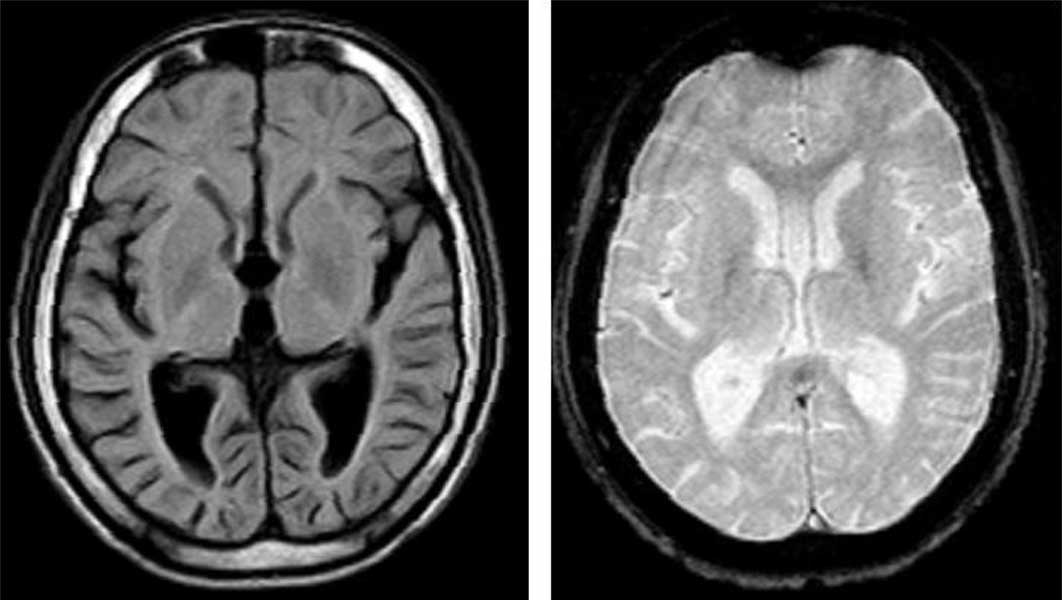
Axial FLAIR and gradient [GRE} images. FLAIR image shows diffuse atrophy with reduced white matter volume and no evidence of dysmyelination . GRE image shows small ares of hypointensity in basal gangia suggests soft calcification.
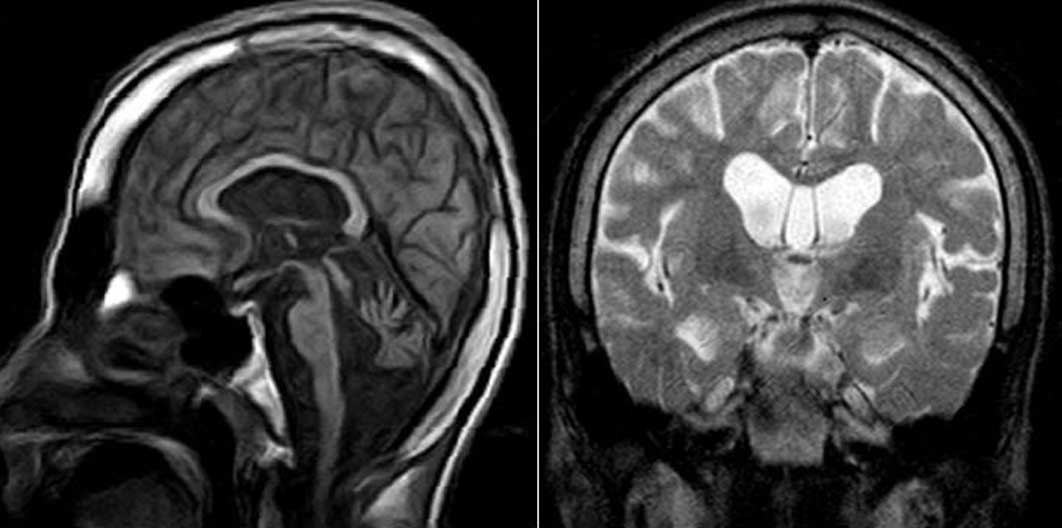
T1 weighted saggittal and T2 weighted coronal images. T1 and T2WI show diffuse cerebral and cerebellar atrophy with thinning of brain stem and soft calcification of basal ganglia on T2WI.
Discussion
The Cockayne Syndrome which is transmitted as an autosomal recessive trait, is a DNA repair – deficient disorder and it consists of abnormal ultra violet hyper sensitivity, retinitis pigmentosa, premature aging, dwarfism, microcephaly, deafness and progressive encephalopathy [1-3].
The Cockayne Syndrome is a rare condition with less than 40 cases in the world literature. This syndrome often goes undetected in infancy, during which the growth and development are normal. The progressive degeneration is manifested by the second or the third year of life. Most of the survivors live upto the fourth decade. The male to female ratio is 3:1. The neuropathologic changes include neuronal and myelin loss with deposits of calcium and iron in the vessels in the cerebellum, the basal ganglia and the cerebrum. The most common neurological manifestation is mental retardation, and the other classical features include retinitis pigmentosa and photosensitive retinitis. The previously reported radiological findings of the Cockayne Syndrome include atrophy of the brain stem, cerebellum and the cerebrum, and the high signal intensity of the cerebral white matter on T2 weighted images, which reflects demyelination [4-8]. Calcification of the dentate nucleus of the cerebellum and the basal ganglia has also been documented. [6-8]. The pathogenesis of the Cockayne Syndrome is unknown. Its diagnosis is based on the clinical diagnostic criteria and it may be supported by the demonstration of the intracranial calcification. The calcification of the basal ganglia and the subcortical white matter may be detected on CT as early as 3 years of age . The few detailed neuropathological studies which have been done, have shown calcification in the basal ganglia, with a variable degree of cerebral and cerebellar calcifications and cerebellar atrophy and white matter atrophy, with a patchy demyelination [9].
MRI is a sensitive tool which can demonstrate the white matter disease. MRI demonstrated results which were compatible with the diffuse hypomyelination of the cerebral white matter.
The MRI in our patient showed diffuse white matter atrophy with no demyelination. From our observations, it was not possible to differentiate the Cockayne Syndrome from the other white matter diseases in the absence of the intraparenchymal brain calcifications. In the appropriate clinical context, the MRI features like hypomyelination, supratentorial white matter loss, cerebellar atrophy or hypoplasia, and bilateral basal ganglia calcifications are an important adjunct for supporting the diagnosis of the Cockayne Syndrome.
Conclusion
Hypomyelination, supratentorial white matter loss, cerebellar atrophy or hypoplasia, and bilateral basal ganglia calcifications are the most typical features in the Cockayne Syndrome, which are often associated with the cortical calcifications in the early-onset types of the disease. These features can help in differentiating the Cockayne Syndrome from other leukodystrophies.
[1]. Lehman AR, The DNA repair-deficient diseases, Xeroderma pigmentosa, the Cockayne Syndrome and trichothiodystrophyBiochemie 2003 85:1101-11. [Google Scholar]
[2]. Ren Y, Saio M, Nakatsu Y, Nakai H, Yamiazumi M, The Cockayne Syndrome group AGenes Genet Syst 2003 78:93-102. [Google Scholar]
[3]. Komutsu A, Suzuki S, Inagaki T, Yamashita K, Hashizume K, A kindred with the Cockayne Syndrome which was caused by multiple splicing variants of the CSA geneAm J Med Jenet A 2004 128:67-71. [Google Scholar]
[4]. Sugita K, Takanashi J, Ishii M, Niimi H, Comparison of the MRI white matter changes with the neuro psychological impairment in the Cockayne SyndromePaediatr Neurol 1992 8:295-98. [Google Scholar]
[5]. Hamel BC, Raama A, Schuitema-Dijkstra AR, The Xeroderma pigmentosa – the Cockayne Syndrome complex: a further caseJ Med Genet 1996 33:607-10. [Google Scholar]
[6]. Demaerel P, Kendall BE, Kingsley D, Cranial CT and MRI in the diseases with DNA repair defectsNeuroradiology 1992 34:117-21. [Google Scholar]
[7]. Bolthauser E, Yalcinakya C, Wichmann W, Reuuter F, Prader A, Valavanis A, MRI in the Cockayne Syndrome Type 1Neuroradiology 1989 31:276-77. [Google Scholar]
[8]. Demaerel P, Wilms G, Verdru P, Carton H, Baert AL, MRI in the diagnoisis of the Cockayne Syndrome. One caseJ Neuroradiol 1990 17:157-60. [Google Scholar]
[9]. Softer D, Grotsky W, Rapin I, Suzuki K, The Cockayne Syndrome: the unusual neuropathological findings and the review of the literatureAnn Neurol 1979 6:340-48. [Google Scholar]