A Rare Cause of Gastric Perforation-Candida Infection: A Case Report and Review of the Literature
Nalini Gupta1
1 Dr. Nalini Gupta, Department of Histopathology, SRL Religare Reference Laboratory, Gurgoan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nalini Gupta, CC6/18 Arr Dee City IInd Floor, Sector 52, Gurgoan-122001, Haryana, India.
Phone: 9990370677
E-mail: drnalinibansal@yahoo.com
Fungal microorganisms as a cause of gastric perforation, is very rare. Most of the cases of gastric perforation are seen as the complications of peptic ulcer disease, the intake of NSAIDs (Non Steroidal Anti-Inflammatory Drugs), neoplastic diseases, etc. We are reporting a case of a 50 year old male who presented with a sudden onset of abdominal pain and shock and was diagnosed as acute peritonitis which was caused by a gastrointestinal perforation. An emergency exploratory laporotomy was performed and a gastric perforation repair with omentoplexy was done. However, the patient died in the post operative period due to a sudden cardiac arrest. A gastric perforation edge biopsy revealed the presence of fungal hyphae. The peritoneal fluid culture revealed Candida albicans colonies.
Gastric perforation, Fungal infection, Candida perforation
Introduction
Candida infections of the gastrointestinal tract are rare as its ph is low and the candida colonies are normal commensals of the gastrointestinal tract. Gastric perforation which is caused by Candida infections is very rare and it is seen mostly in immunocompromised and debilitated patients. However, the habitual use of strong antacids can also cause severe Candida infections of the stomach in healthy persons, as seen in this case [1]. We are reporting the case of a 50 year old male who presented with a gastric perforation which was diagnosed as a fungal infection on biopsy of the perforation edge.
Case Report
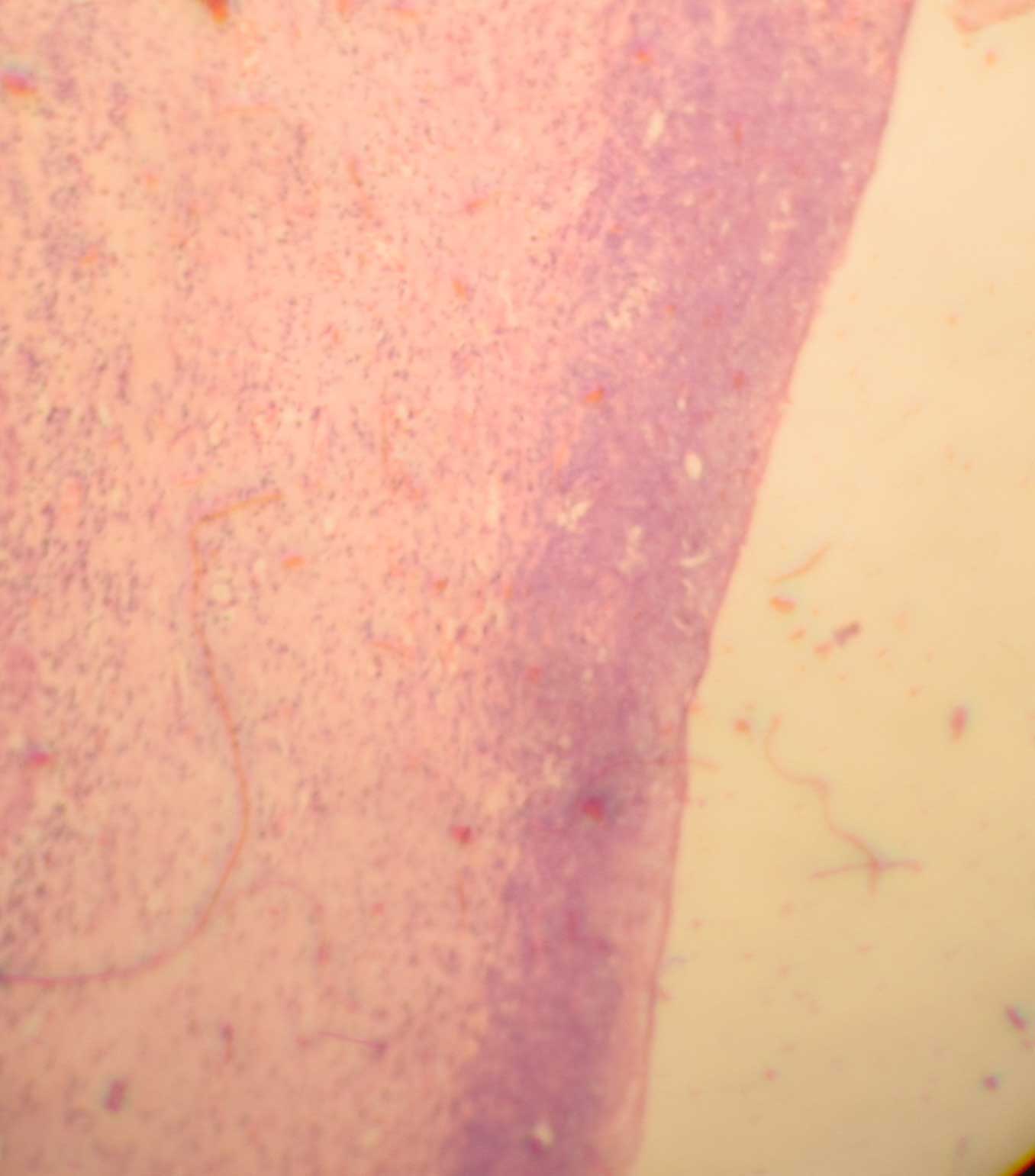
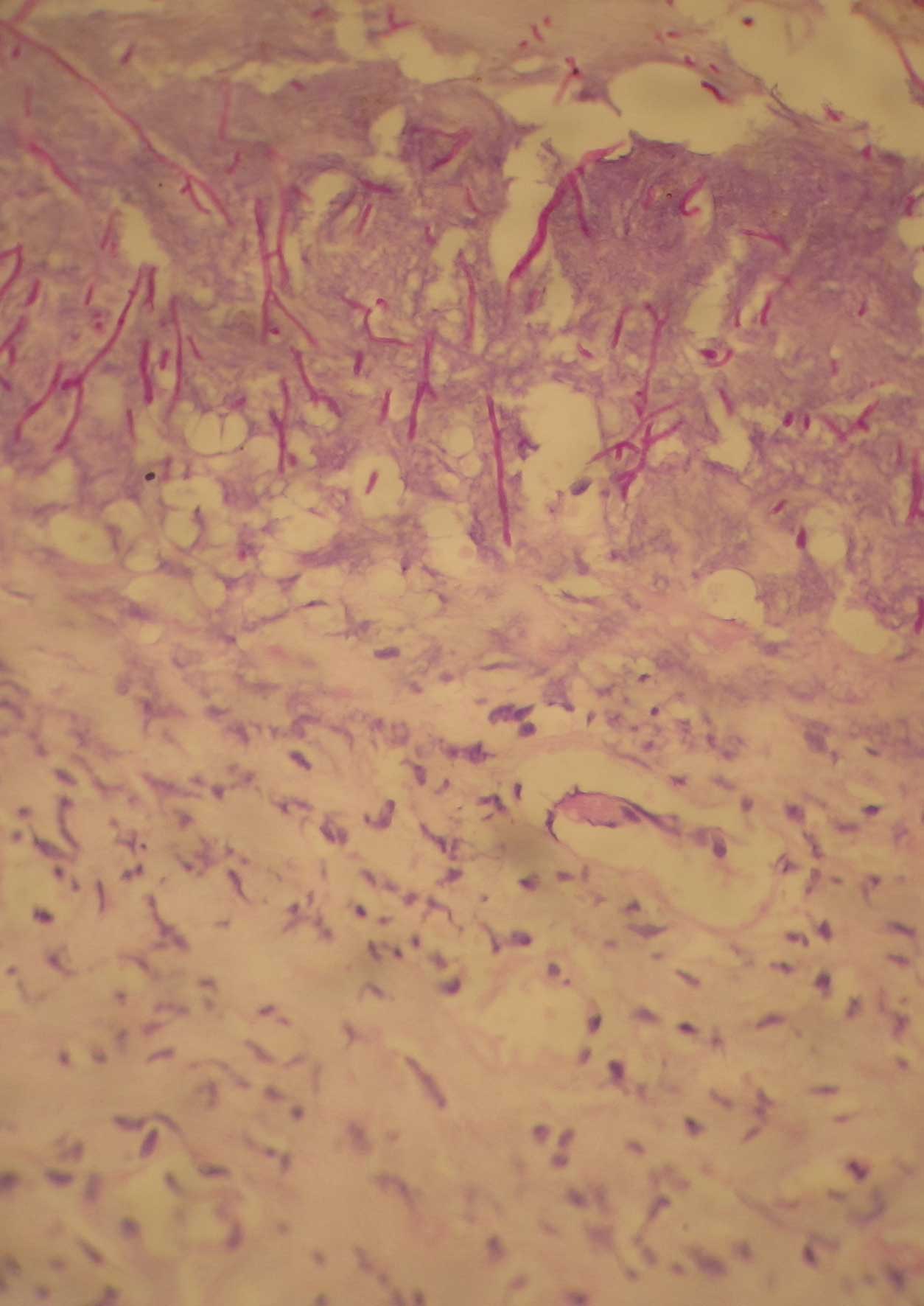
We are reporting a case of a 50 yr old male who presented with an altered sensorium. He was in shock for the past 4 hours. There was a history of abdominal pain since 1 week along with constipation and infrequent vomiting. This had progressed to a severe sudden onset of abdominal pain along with abdominal distension and constipation since 1-2 days. His past history was not significant. There was no past history of diabetes, hypertension or tuberculosis. The patient was a known bidi smoker with a history of occasional alcohol intake. A history of strong antacid intake was there. On general examination, his pulse rate was found to be feeble 130/min and his blood pressure was non recordable. His oxygen saturation was 75%. There was tenderness and guarding all over the abdomen and a liver dullness was absent. The chest X Ray showed a moderate amount of gas under the right dome of the diaphragm, with a bilateral bronchovascular prominence which was more on the right side. His white blood cell count was 13,300/mm3 with neutrophilia (83%). His prothrombin time and Activated Partial Thromboplastin Time PTT were high (35.4 sec and 44.8 sec respectively). His blood glucose level was low 20mg/dl and his creatinine and potassium levels were high. The serological tests which were done for HIV, hepatitis B and C were negative. The patient was resuscitated, Ryle's tube aspiration was done , a urinary catheter was put in and an emergency exploratory laprotomy was performed with a midline upper abdominal incision. It showed 2-2.5 litres of frank bilious fluid with pus flakes all over the abdomen. There was a 1 x 1cm prepyloric perforation which was repaired with a Lambert suture and an omental patch after a perforation edge biopsy was done.The gastric wall which was adjacent to the perforation was unremarkable to the bimanual palpation. The perforation edge biopsy was sent for histopathology and the peritoneal fluid was sent for culture. The patient gained conciousness, with an improved blood pressure and an improved pulse rate postoperatively. However, he died subsequently due to a sudden cardiac arrest. The histopathological examination of the perforation edge biopsy revealed the presence of fungal hyphae [Table/Fig-1]. Periodic Acid Schiff's PAS staining which was done, showed a positive staining in these pseudohyphae, which was suggestive of a Candida infection as a cause of the perforation [Table/Fig-2]. The peritoneal fluid culture revealed colonies of Candida albicans. A bacterial culture was not done.
Light microscopy from perforation edge biopsy revealed fungal hyphae (H& E X 10)
Light microscopy showing entangled fungal hyphae (PAS stain X 40)
Discussion
Candida is a ubiqutous fungus, even in the gut of healthy individuals. However, it is rarely pathogenic in the gut. Under normal circumstances, the level of the Candida are controlled by beneficial bacteria. However, if the bacterial-fungal balance is upset by the usage of antibiotics, for example, or if the immune system is compromised, an overgrowth of Candida can occur, resulting in an infection.
The Candida infections in the gut occur mostly in immunocompromised patients, in patients who are on steroid therapy, in those with diabetes mellitus and HIV infection, in patients who are on chemotherapy, etc and very rarely, Candida infections of the gut occurs in healthy persons[2-4]. A fungal overgrowth in the gut is encouraged by certain pH levels and by the availability of sugar (glucose)[5,6]. The patients who regularly use antacids and those with hyperglycaemia are at an increased risk.
In our case, the patient was healthy and immunocompetant, but he had a history of the regular use of antacids, which might have been the predisposing factor for the Candidal gastric perforation.
In one study which was done by Ears et al., gut mycosis was observed in 109(4.35%) of the 2517 total cases which were studied from 1960–1964 [7]. In Japan, Tsukamoto et al., reported that gut mycosis was present in 196(5.9%) of the 3,339 cases which were reported from 1971 to 1983 [8]. In these reports, the most commonly effected organ was the oesophagus, followed by the stomach, the small intestine and the large intestine [7,8]. Minali et al., reported that stomach candidiasis was seen in 0.96% of the upper intestinal endoscopies [9].
The Candida infection is a serious medical condition that requires an immediate medical attention. The invasive Candida infections are characterized by fever and shock along with low blood pressure, an elevated heart rate, respiratory distress and multiorgan failure. However, an early diagnosis can prevent these complications. Undiagnosed gastric candidiasis can be associated with a significant morbidity and mortality. In our case, the patient presented with shock and acute abdominal pain. An exploratory laporotomy was done and it revealed a gastric perforation for which a repair and ometoplexy was done. However, the patient was not given any antifungal treatment at that time. The patient died subsequently in the post operative period due to a sudden cardiac arrest. His perforation edge biopsy revealed fungal pseudohyphae of the Candida species.
This case emphasized the rare fungal aetiology as a cause of the gastric perforation. The fungal aetiology should always be thought of as an aetiology for the gastric perforation, even in healthy patients, to reduce the significant mortality which is associated with this disease, as a early detection is necessary to treat the Candida infections.
[1]. Bakhshi GD, Borisa AD, Shaikh AS, Thadeshwar NR, Kher Y, Kapadnis LA, Invasive gastric candidiasis with perforationBombay Hospital Journal 2011 53(2):264-65. [Google Scholar]
[2]. Pugh TF, Fitch SJ, Invasive gastric candidiasisPediatric Radiology 1986 16:67-68. [Google Scholar]
[3]. Gock M, Schafer M, Perren A, Demartines N, Clavien PA, A fatal oesophageal perforation which was caused by invasive CandidiasisAnn Thoracic Surg 2005 80:1120-22. [Google Scholar]
[4]. Tran HA, Vincent J, Slavin M, Griggs A, Esophageal perforation which was secondary to angioinvasive Candida glabrata following a hemopoitic stem cell transplantationClinical microbiology and infection 2003 9:1215-18. [Google Scholar]
[5]. Ginnis MR, MycetomaDermatol Clin 1996 14(1):97-104. [Google Scholar]
[6]. Buddington RK, Williams CH, Chen SC, Witherly SA, Dietary supplement of neosugar alters the fecal flora and the decreases activities of some reductive enzymes in human subjectsAm J Clin Nutr 1996 63(5):709-16. [Google Scholar]
[7]. Ears P, Goldstein M, Sherlock P, Candida infections of the gastrointestinal tractMedicine 1972 51(5):367-79. [Google Scholar]
[8]. Tsukamoto H, Clinicopathological studies on fungal infections of the digestive tractJpn J Gastroenterol 1986 83:2341-50. [Google Scholar]
[9]. Minali G, Teruzzi V, Butti G, Frigerio G, Rossini A, Gastric candidiasis: an endoscopic and a histological study in 26 patientsGastrointestinal endoscopy 1982 28:59-61. [Google Scholar]