A Glomus Tumour Arising from the Flexor Aspect of the Forearm: A Case Report with Review of the Literature
Jitendra Singh Nigam1, Vatsala Misra2, Anshul Singh3, Veer Karuna4, Smita Chauhan5
1 Junior resident, Department of Pathology, M.L.N.Medical CollegeAllahabad, U.P., India.
2 Professor and Head of Department, Department of Pathology, M.L.N.Medical CollegeAllahabad, U.P., India.
3 Assistant Professor, Department of Pathology, M.L.N.Medical CollegeAllahabad, U.P., India.
4 Junior Resident, Department of Pathology, M.L.N.Medical CollegeAllahabad, U.P., India.
5 Junior Resident, Department of Pathology, M.L.N.Medical CollegeAllahabad, U.P., India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jitendra Singh Nigam Department of Pathology M.L.N.Medical College Allahabad, U.P., India.
Phone: +919412628083
E-mail: nigamjs@gmail.com, dr_jsnigam@yahoo.co.in
A 45 year old male patient presented with the complaint of a purplish nodular painful swelling on the flexor aspect of the left forearm of five years duration. A radiological examination of the lesion was not done prior to its excision. A biopsy was done and it was sent for a histopathological examination. The biopsied tissue was single, irregular, firm and globular, it measured 0.5 x 0.5cm in size and it was processed in two halves Its microscopic examination showed a well circumscribed area which comprised of sheets and nodules of monomorphic round cells with slightly vesicular, round nuclei and an acidophilic cytoplasm, amongst which were interspersed numerous blood vessels, many of which were dilated and congested, along with numerous lymphatic channels which were filled with lymph. Immunohistochemistry for SMA, CEA and CD 34 was advised, out of which only SMA turned out to be strongly positive and a final diagnosis of a Glomus tumour was made.
Vascular tumour, Extradigital tumour, Forearm
Introduction
The glomus tumour is a distinctive neoplasm that arises from the smooth muscle of the glomus body [1]. The glomus tumours typically occur in young adults but they can occur at any age. No sex predilection is seen, except in the subungual lesions which are far more common in women [2]. The commonest sites are the subungual regions, the lateral areas of the digits, and the palm [1]. Histologically, the glomus tumours and their variants are benign neoplasms that require only a simple excision. We are describing here, a case of a glomus tumour of five years duration, which arose on the flexor aspect of the left forearm.
Case Report
A 45-year old male patient presented with the complaint of a nodular, purplish swelling on the flexor aspect of the left forearm of five years duration, which was painful. He also gave a history of a nodule which was removed by surgery from the same site few years back by a local doctor, the histopathology of which was not done. The complete blood count, the random blood sugar levels, the chest X-ray and the ECG were normal. A biopsy was done and the tissue was sent for a histopathological examination.
The biopsied tissue was single, irregular, firm, globular and bluishblack in colour, which measured 0.5 x 0.5 cm in size. The cut surface was greyish white. The piece was processed in two halves.
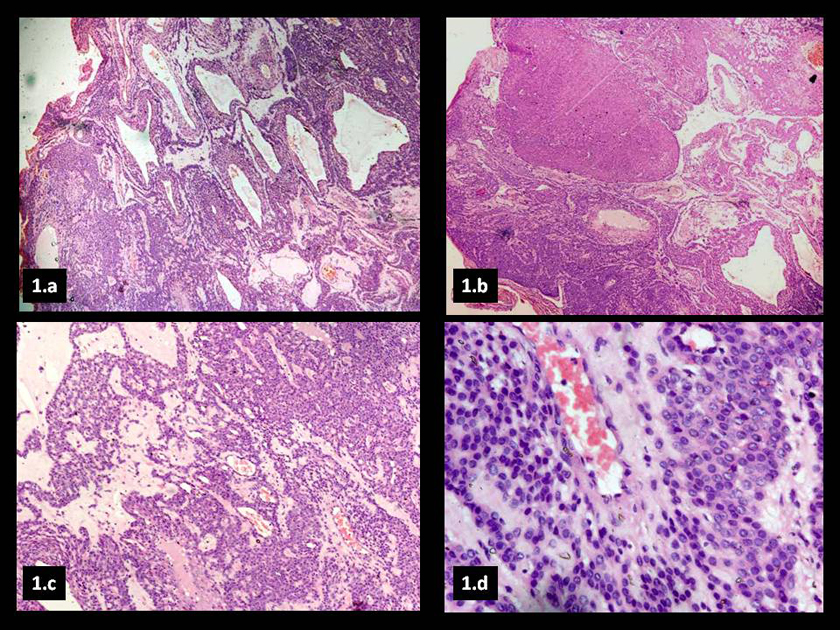
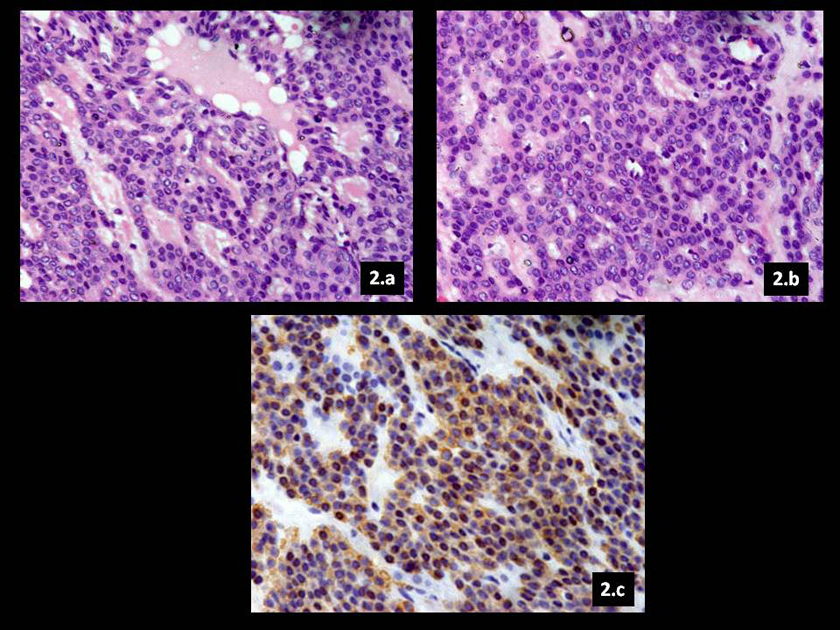
The microscopic examination showed a well circumscribed area which comprised of sheets and nodules of monomorphic round cells with slightly vesicular round nuclei and an acidophilic cytoplasm, amongst which were interspersed numerous blood vessels, many of which were dilated and congested, along with numerous lymphatic channels which were filled with lymph [Table/Fig-1(a), (b), (c), (d), and 2(a), (b)]. A differential diagnosis of haemangioma, glomus tumour and eccrine spiradenoma were made. The immunohistochemistry for SMA (for glomus tumour), CEA (for eccrine spiradenoma) and CD 34 (for haemangioma) was done. SMA was strongly positive [Table/Fig-2c], whereas CEA and CD34 were negative and a final diagnosis of a glomus tumour was made.
(a) Numerous dilated blood vessels with interspersed monomorphic glomus cells (H&E x100); (b) Solid area of glomus tumour (H&E x100); (c) Monomorphic tumour cells in a background of oedema (H&E x100); (d) Tumour cells with eccentric round vesicular nuclei and scant cytoplasm (H&E x400)
(a) Tumour cells arranged concentrically around blood vessels (H&E x400); (b) Tumour cells intermixed with numerous bloodvessels(H&Ex400); (c) Diffuse cytoplasmic positivity for SMA ( x400)
Discussion
The normal glomus body is a specialized form of arteriovenous anastomosis which regulates heat [1]. It is located in the stratum reticularis of the dermis and it is most frequently encountered in the subungual region, the lateral areas of the digits, and the palm [1]. The glomus body is made up of an afferent arteriole which is derived from the small arterioles which supply the dermis and which branch into two or four preglomic arterioles [1]. These arterioles are endowed with the usual complement of the muscle cells and an internal elastic lamina, but they blend gradually into a thick-walled segment with an irregular lumen which is known as the Sucquet- Hoyer canal [1]. This region is the arteriovenous anastomosis proper. It is lined by plump cuboidal endothelial cells, which in turn are surrounded by longitudinal and circular muscle fibres, but with no elastic tissue. Scattered throughout the muscle fibres are the rounded, epithelioid “glomus” cells [1]. These canals drain into a series of thin-walled collecting veins. The entire glomic complex is encompassed by a lamellated, collagenous tissue which contains small nerves and vessels [1]. The glomus tumour, which is also known as a solitary or a solid glomus tumour, a glomangioma and a nonchromaffin paraganglioma, is a rare benign neoplasm which arises from the glomus body or the Sucquet-Hoyer canal of this apparatus and it accounts for 1-2% of the soft tissue tumours in the hand. This neoplasm was first fully described by Masson in 1924 [3]. The presentation is generally a solitary lesion, but in some cases, multiple lesions have been described. The lesions develop as small blue-red nodules that are usually located in the deep dermis or the subcutis of the upper or the lower extremity. The single most common site is the subungual region of the finger, but the extradigital sites include the palm, wrist, forearm, foot, bone, stomach, colon, trachea, vagina, cervix, and the mesentery [1]. A pathological review of 52 atypical glomus tumours showed tumour locations that ranged from the thigh (n=11), calf and ankle (n=7), foot (n=4), buttock (n=3), trunk and the abdomen (n=7) to the arm (n=9), wrist and hand (n=7), lung (n=2), stomach (n=1) and even the L3 vertebra (n=1). Other studies suggested that the frequency of the extradigital cases varied from 11-65% and that it may be more common in men than in women [4].
The superficially located glomus tumours often present with paroxysms of pain which radiate away from the lesion; these symptoms are often exacerbated by the changes in the temperature, in particular, the exposure to cold. The deeply seated glomus tumours typically have no associated symptoms [2].
Few cases of extradigital glomus tumours which were found in the forearm have also been reported [5-9]. Most of these were either intravascular or deep seated [10,11]. In the present case, the lesion was superficial and it was not related to any major blood vessels. The first case of an intravascular glomus tumour, which was located in the right forearm of a 40 year old male, was described by Beham et al., in 1991 [8]. Acebo et al described a report of an elderly woman with a tumour which completely occluding the vein from which it grew in her right forearm [10].
In 2005, Le et al., reported a case of a glomus tumour of the softtissues of the forearm in a 23 year old woman. The diagnosis was suspected on MRI, and confirmed by doing a biopsy [6].
Hoglund et al., studied 96 cases of five common soft tumours of the hand. They concluded that ultrasound should be the first imaging investigation for soft-tissue tumours of the hand. However, MRI should also be performed when the diagnosis continues to be obscure and when a malignancy is suspected [12]. Magnetic resonance imaging may be useful in the detection of the tumours, but it may not always be sensitive [7]. The plain radiographs and the angiographs tend to be normal and of no help in determining the type of mass which is present [9]. Although blood vessel tumours are rare, they are frequently encountered in the hand and in the forearm, they being the fourth most common tumours of the hand [13]. A physician who treats the acquired, traumatic, and the congenital vascular tumours of the hand and the forearm, should also consider glomus tumour in the differential diagnosis. In the present case, the tumour was located on the flexor aspect of the left forearm for the past five years, which was painful.
Conclusion
Extradigital glomus tumours may be encountered in the hand and in the forearm, they being the fourth most common tumours of the hand. Both the pathologists and the surgeons should be aware of this and they should consider it in the differential diagnoses of such vascular lesions of the upper limb.
[1]. Weiss SW, Goldblum JR, Enzinger and Weiss's Soft Tissue Tumours 2008 5th editionPhiladelphiaMosby, Inc., an affiliate of Elsevier, Inc.:751-70. [Google Scholar]
[2]. Folpe AL, Guillou L, Tumours of the perivascular cells. In: Folpe AL, Inwards CY editorsBone and Soft Tissue Pathology (a volume in the series foundations in diagnostic pathology) 2010 1stPhiladelphiaSaunders, an imprint of Elsevier, Inc.:153-57. [Google Scholar]
[3]. Moor EV, Goldberg I, Westreich M, Multiple glomus tumour: A case report and review of the literatureAnn Plast Surg. 1999 43:436-38. [Google Scholar]
[4]. Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW, Atypical and malignant glomus tumours: An analysis of 52 cases, with a proposal for the reclassification of the glomus tumoursAm J Surg Pathol. 2001 25:1-12. [Google Scholar]
[5]. Googe PB, Griffin WC, Intravenous glomus tumours of the forearmJ Cutan Pathol. 1993 20:359-63. [Google Scholar]
[6]. Le Bellec Y, Yelles F, Kapandji T, Silbermann-Hoffman O, Glomus tumour of the forearm: A case reportChir Main. 2005 24:99-102. [Google Scholar]
[7]. Takei TR, Nalebuff EA, Extradigital glomus tumoursJ Hand Surg [Br] 1995 20:409-12. [Google Scholar]
[8]. Beham A, Fletcher CD, Intravascular glomus tumour: A previously undescribed phenomenonVirchows Arch A Pathol Anat Histopathol 1991 418:175-77. [Google Scholar]
[9]. Kogure H, Shirakura K, Arisawa N, Aramaki T, Shimegi A, 3 deepseated glomus tumours in the lower armActa Orthop Scand. 1996 67:194-95. [Google Scholar]
[10]. Acebo E, Val-Bernal JF, Arce F, Giant intravenous glomus tumoursJ Cutan Pathol. 1997 24:384-89. [Google Scholar]
[11]. van der Lei B, Damen A, van Valkenburg E, Compression of the lateral cutaneous nerve of the forearm by a glomus tumourJ Hand Surg [Br] 1997 22:71-72. [Google Scholar]
[12]. Hoglund M, Muren C, Brattstrom G, A statistical model for the ultrasound diagnosis of soft-tissue tumours in the hand and the forearmActa Radiol. 1997 38:355-58. [Google Scholar]
[13]. Palmieri TJ, Vascular tumours of the hand and the forearmHand Clin. 1987 3:225-40. [Google Scholar]