A Rare Case of Primary Parapharyngeal Well Differentiated Liposarcoma with Rhabdomyoblastic Differentiation
Geetha V.1, Bhavna N.2, Ruchi K.3
1 Additional Professor of Pathology, KMC, Manipal University, Manipal, India.
2 Assistant Professor of Pathology, KMC, Manipal University, Manipal, India.
3 Assistant Professor of Pathology, KMC, Manipal University, Manipal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhavna Nayal Assistant Professor, Department of Pathology, Kasturba Medical College, Manipal, Manipal University, India
E-mail: bhavnayal17@gmail.com
Rhabdomyoblastic differentiation in liposarcoma is a rare entity, with only few cases being reported in the literature. These cases were reported in either dedifferentiated liposarcomas or in recurrent tumours which occurred in the retroperitoneum. The present case was a rare case of a primary parapharyngeal well differentiated liposarcoma with a focal rhabdomyoblastic differentiation.
Rhabdomyosarcomatous differentiation, Liposarcoma, Parapharyngeal
Introduction
Liposarcoma, a soft tissue tumour of adult life, most frequently occurs in the thigh and the retroperitoneum [1]. The head and neck region is less commonly affected. Benign or malignant heterologous mesenchymal components may be present in liposarcomas [2]. There are very few cases of a divergent rhabdomyosarcomatous differentiation which have been reported in the literature and almost all have been documented in retroperitoneal dedifferentiated liposarcomas or in recurrent tumours [2,3].
We are describing a case of a primary parapharyngeal sclerosing liposarcoma with a focal rhabdomyosarcomatous differentiation in the absence of a dedifferentiated component. Immunohistochemistry was done to confirm our diagnosis.
Case Report
A 72 year old male presented with a gradually progressive dysphagia of eight months duration. On laryngoscopic examination, a smooth bulge was found to be present on the left side of the posterior pharyngeal wall, which was touching the epiglottis. The clinical impression was that of lipoma. Contrast enhanced CT revealed a retropharyngeal mass with a left parapharyngeal extension. The routine haematologic and biochemical investigations were normal. The parapharyngeal tumour was excised by a transcervical approach and it was sent for a histopathological examination. The excision specimen consisted of a well circumscribed nodular mass which weighed 148gms and measured 9.5 x 8.5 x 3.5cms. The cut section showed a solid, grey white tumour with interspersed yellow and myxoid areas [Table/Fig-1]. The histologic examination showed a tumour which was composed of sheets of adipocytes in varying stages of differentiation, some being spindle shaped and pleomorphic, with enlarged hyperchromatic nuclei and others with irregular nuclear membranes and moderate to scant vacuolated and eosinophilic cytoplasm, with some of the vacuoles causing indentation of the nuclear membrane. Few multivacuolated lipoblasts were noted to be interspersed amongst large univacuolated adipocytes [Table/Fig-2]. Further, few rhabdomyoblast-like large ovoid cells with abundant, deeply eosinophilic fibrillar cytoplasm were also noted. On immunohistochemistry, these cells showed positivity for desmin, thus confirming the light microscopic impression of rhabdomyoblasts [Table/Fig-3]. The stroma showed focal sclerosis with myxoid areas, proliferating vascular channels and a focal chronic inflammatory cell infiltrate.
A well circumscribed nodular mass. Inset: cut section shows solid grey white areas with interspersed yellow fatty and myxoid areas.

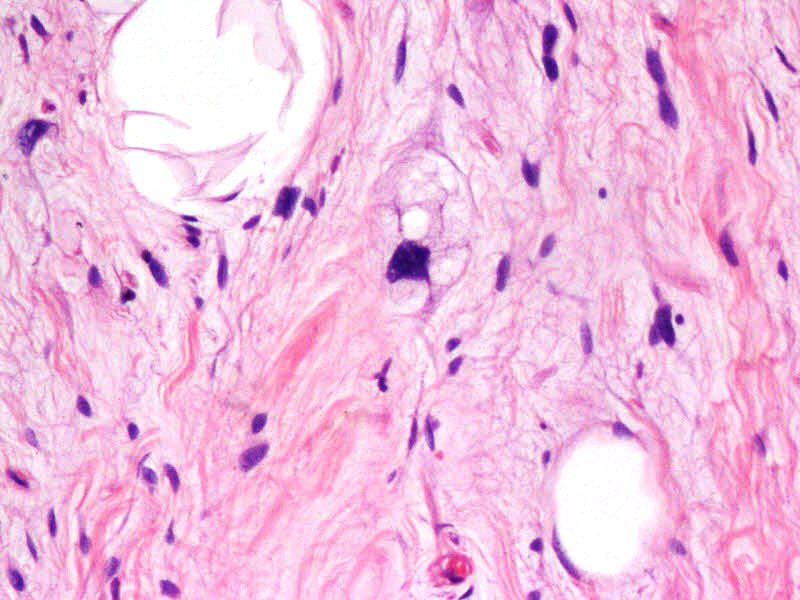
Well differentiated sclerosing liposarcoma with a multivacuolated lipoblast (H and E X400)
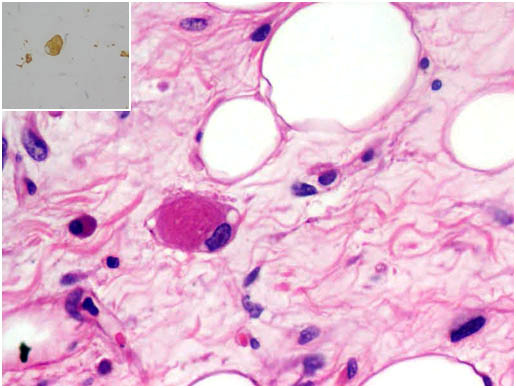
Liposarcoma showing rhabdomyoblast with deeply eosinophilic fibrillar cytoplasm. Inset shows desmin immunoreactivity. (H and E x400)
The surgical excision was complete. One month following the surgical excision, the patient presented with abdominal lymphadenopathy and was diagnosed to have diffuse large B cell lymphoma. Chemotherapy was planned for the same. However, the patient was lost to follow up.
Discussion
Liposarcomas comprise one of the most common adult soft tissue sarcomas. According to the WHO, liposarcomas are divided into 4 subtypes, namely the well differentiated, myxoid/round cell, dedifferentiated and the pleomorphic types. The well differentiated liposarcomas in turn, are categorized morphologically into lipoma like tumours which consist predominantly of mature fat, sclerosing liposarcomas which are characterized by fibrotic zones which alternate with mature adipocytes and the inflammatory type which shows a dense lymphocytic or plasmacytic infiltration which is superimposed on a lipoma like/ sclerosing form [1]. Our case was that of a well differentiated, sclerosing liposarcoma.
The dedifferentiated liposarcomas consist of a well differentiated liposarcoma and a mitotically active spindle cell dedifferentiated component. Most of these tumours result from the progression of a well differentiated liposarcoma due to the acquisition of new cytogenetic anomalies, which give them metastatic potential [1]. Various heterologous elements can been seen in the dedifferentiated component of these tumours, which include smooth muscles, striated muscles, cartilages, vessels and bones [3,4].
Heterologous rhabdomyoblastic elements have been described in very few cases of liposarcomas and they have been seen in recurrent retroperitoneal liposarcomas with dedifferentiation [2,3].
To the best of our knowledge, only 2 cases of primary liposarcoma with a rhabdomyoblastic differentiation have been described in the literature. In the first case, the rhabdomyosarcomatous component coexisted within a mixed pleomorphic and myxoid liposarcoma [3], while the second was a myxoid liposarcoma with a rhabdomyoblastic differentiation [4]. To the best of our knowledge, the present case is the first account of a primary well differentiated sclerosing liposarcoma with a divergent rhabdomyosarcomatous differentiation. In our case, sheets of adipocytes in various stages of maturation were seen, along with focal areas which contained interspersed desmin positive rhabdomyoblasts and sclerotic bands. We excluded the possibility of a dedifferentiation by careful gross and microscopic examinations.
Liposarcomas with rhabdomyosarcomatous areas have been shown to have genetic alterations and a prognosis which is similar to that of well-differentiated/dedifferentiated liposarcomas [1,5]. However, no genetic studies were done in our case. Due to the very short follow up duration of one month, the prognostic implication of the rhabdomyosarcomatous differentiation in liposarcoma cannot be commented on in the present case.
[1]. Enzinger FM, Weiss SW, Goldbum JR, Soft Tissue Tumors. 5th ed. St Louis, Mo: Mosby 2008 :477-516. [Google Scholar]
[2]. Mc Cormick D, Mentzel T, Beham A, Fletcher CD, A dedifferentiated liposarcoma. A clinicopathologic analysis of 32 cases which suggested a better prognostic subgroup among the pleomorphic sarcomasAm J Surg Pathol 1994 18(12):1213-23. [Google Scholar]
[3]. Shanks JH, Banerjee SS, Eyden BP, A focal rhabdomyosarcomatous differentiation in a primary liposarcomaJ Clin Pathol 1996 49:770-72. [Google Scholar]
[4]. Govender D, Pillay P, A primary myxoid liposarcoma with rhabdomyoblastic differentiationArch Pathol Lab Med 1998 122:740-42. [Google Scholar]
[5]. Shimada S, Ishizawa T, Ishizawa K, Kamada K, Hirose T, A dedifferentiated liposarcoma with a rhabdomyoblastic differentiationVirchows Arch 2005 Jul 13 447(5):835-41. [Google Scholar]