A Rare Presentation of the Klinefelter’s Syndrome
Sharabeh Hezarkhani1, Mohammad Moujerloo2, Sima Sedighi3, Negar Sadat Taheri4
1Department of Internal Medicine, Golestan University of Medical Sciences, Gorgan, Iran.
2Department of Internal Medicine, Golestan University of Medical Sciences, Gorgan, Iran.
3Department of Internal Medicine, Golestan University of Medical Sciences, Gorgan, Iran.
4Golestan Research center of Gastroenterology and Hepatology, Golestan University of Medical Sciences, Gorgan, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Negar Sadat Taheri, Shahid Nabavi Polyclinics, 4th Azar Alley, 5 Azar Blvd, Gorgan, Iran. Postal Code: 4917765181 Tel: +981712340835; Fax: +981712369210
E-mail: negar_taheri1@yahoo.com
A 16 years old boy with Chronic Renal Failure (CRF) was not suspected of having Klinefelter’s syndrome until he complained of painful gynecomastia. He was under haemodialysis for 2 years. At first, he was in an approximately full pubertal development (P5, G5), but he had a small and a firm testis (length 2.2cm) and some degree of facial male pattern hair. He also had a decreased upper to lower body segment ratio and despite having chronic renal failure, he was taller than his parents and siblings. His laboratory tests showed high levels of FSH and normal levels of LH and testosterone. With regards to all these findings, we suspected that there might be an occult Klinefelter’s syndrome. So, we made his karyotype that showed a 47XXY pattern. Because there are only a few number of cases that have occult Klinefelter’s syndrome in the basis of chronic renal failure, we decided to report this case.
CRF, Occult klinefelter, Haemodialysis
Introduction
Gynecomastia is a complication of chronic renal failure which occurs due to an imbalance between oestradiol and testosterone in these patients. Chronic renal failure may also lead to hypogonadotropic hypogonadism that is due to the chronic disease, but the kidney can’t catabolize and secret the FSH and LH. So the serum level of these hormones are elevated in chronic renal failure [1].
Klinefelter’s syndrome is the most common chromosomal abnormality that is associated with primary testicular insufficiency and infertility. The prevalence of Klinefelter’s Syndrome is between 1: 500 to 1:1000 live born boys. The most prevalent karyotype in Klinefelter’s syndrome is 47XXY [2-4]. Most of the patients with this syndrome go through life without a diagnosis and they may then die due to the comorbid conditions of the disease, which include acute leukaemia, lymphoma and germ cell tumours, aortic valvular disease, the rupture of the berry aneurysms and breast carcinoma (20 times the rate in normal men and one fifth of that in women), systemic lupus erythematosus and osteoporosis in about 25% of the affected adults. There is an increased risk of diabetes mellitus, thyroid disease, fatigue, varicose veins and essential tremors [2,5,6].
Gynecomastia is a manifestation of Klinefelter’s syndrome and it is also seen in chronic renal failure [1,2].
As has been noted earlier, chronic renal failure is associated with an increase in the FSH and the LH levels due to the impairment of the renal function in catabolizing these hormones. Consequently, if a patient has these two conditions at the same time (CRF and Klinefelter’s syndrome), the presence of gynecomastia and also an increase in the FSH and the LH levels, that are seen in chronic renal failure, can overlap with the Klinefelter’s syndrome manifestations and they can mask and leave the Klinefelter’s syndrome undiagnosed. Consequently, these patients can be affected by the comorbid conditions which are associated with Klinefelter’s syndrome.
Here, we are reporting a case of chronic renal failure who complained of painful gynecomastia, with elevated FSH and normal LH levels. Moreover, this patient was diagnosed with Klinefelter’s syndrome by virtue of the 47XXY karyotype in his peripheral blood smear.
Case Report
A 16-years old boy with chronic renal failure was referred to the endocrinology clinic of 5-Azar Hospital in Gorgan – Iran, for the management of painful gynecomastia. He was suffering from painful gynecomastia since 5 months. He also had urinary reflux since he was 6 years old and he was under haemodialysis three times per week for 2 years [Table/Fig-1].
Gynecomastia and facial male pattern
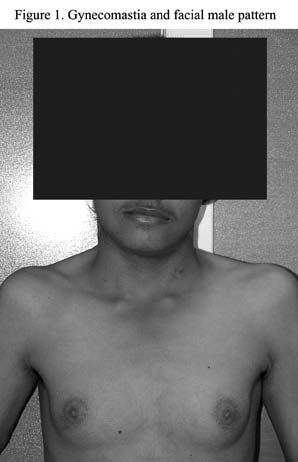
On his first visit, the patient was found to be 164.5cm tall and he weighed 40kg. His upper to lower body segment proportion was 0.89 and his arm span was 160.5. His blood pressure was 130.85mm Hg and his pulse rate was 75 per minute. His physical examination showed bilateral 4.5cm gynecomastia and his genital examination was G5, P5 based on the tanner staging, but his testicular length was 2.2cm bilaterally. There wasn’t any heart murmur on the heart examination.
From the laboratory findings, we could detect a high FSH level (49.8 mIU/ml)(normal: 1.4-15.4 mIU/ml), a normal LH level (4.5 mIU/ml) (normal: 1.24-7.8 mIU/ml), a total testosterone level of 316.8 ng/dl (normal: 250-1100 ng/dl), an oestradiol level of 18 (pg/ml) ( normal: 10-50 pg/ml) and normal levels of serum BHCG. The liver function tests were within the normal range. In the sonographic imaging, small testes with no mass or other defects were detected.
With regards to all of these findings, we examined his blood sample for his karyotype. Twenty metaphase spreads were studied on the basis of the GTG technique at a 450-500 band resolution, which revealed the 47XXY pattern. The findings indicated that the patient had Klinefelter’s syndrome with chronic renal failure [Table/Fig-2].
Kariotype of the patients indicate klinefelter syndrome

A written informed consent was obtained from the patient for the publication of this case report and the accompanying images. A copy of the written consent is available for review with the Editorin-Chief of this journal.
Discussion
Chronic renal failure may cause gynecomastia due to an imbalance between oestrogen and testosterone and it may also be associated with an elevation of FSH and LH because of the impaired catabolism and the excretion of these two hormones. The patients with chronic renal failure who had the disease from childhood, always have a short stature and a delayed puberty. All these findings can mask the manifestations of Klinefelter’s syndrome in a patient with chronic renal failure [1].
Klinefelter’s syndrome is a congenital disorder which is seen in men and the predominant karyotype is 47XXY.The disease is characterized by hypogonadism, asospermia, a rise in the FSH and the LH levels and also gynecomastia [1,2,4].
An association between the Klinefelter’s syndrome, diabetes, urogenital infections and congenital malformations of the urogenital system has been reported in a number of studies during the past years [12-14]. A previous study showed an increased risk of death due to urogenital diseases [12].
Although all these associations can lead to an increased risk of renal failure in the patients with Klinefelter’s syndrome, there are no adequate explanations at hand as yet, for their incidences and these possible relationships of chronic renal failure in this syndrome. There are only a few reports on the accompaniment of the Klinefelter’s syndrome and renal abnormalities. There are also a few reports on the occult Klinefelter’s syndrome in the basis of chronic renal failure [7-11].
These observations and the fact that chronic renal failure could mask the clinical and the laboratory findings of Klinefelter’s syndrome on one side, and on the other hand, the importance of the Klinefelter’s syndrome and its comorbid complications such as breast cancer, leukaemia, lymphoma, germ cell tumours and vascular abnormalities, made us think whether there were any associations between the sex chromosomal disorders and renal failure or other renal structural disorders that led to renal failure. Also, there was a question whether it was necessary for the patients with Klinefelter’s syndrome to have regular hospital visits for assessing their renal function or whether it was necessary to search for sexchromosomal abnormalities in patients with chronic renal failure. The future studies will hopefully address these important issues.
[1]. Griffin JE, Wilson JD, Disorders of the testes and the male reproductive tract. In: Larsen PR, Kronenberg HM, Melmed S, Polonsky KS, editorsWilliams textbook of endocrinology 2003 10thPhiladelphia WBSaunders:709-53. [Google Scholar]
[2]. Styne DM, Grumbach MM, Puberty: ontogeny, neuroendocrinology, physiology, and disorders. In: Kronenberg HM, Shlomo M, Polonsky KS, Larsen PR, editorsWilliams Textbook of Endocrinology 2008 11th edPhiladelphia PaSaunders:969-1166. [Google Scholar]
[3]. Visootsak J, Graham JR, The Klinefelter’s syndrome and other sex chromosomal aneuploidiesOrphanet J Rare Dis. 2006 1:1-5. [Google Scholar]
[4]. Verri A, Cremante A, Clerici F, Destefani V, Radicioni A, The Klinefelter’s syndrome and the psychoneurologic functionsMolecular Human Reproduction 2010 16:425-33. [Google Scholar]
[5]. Rovens KÝ, J. Rheumatic diseases and the Klinefelter’s syndromeReview. Scripta Medica. 2006 79:237-46. [Google Scholar]
[6]. Klinefelter HF, Reifenstein EC, Albright F, A syndrome which was characterized by gynecomastia, aspermatogenesis without a-Leydigism and increased excretion of the follicle stimulating hormonesJ Clin Endocr Metab 1942 2:615-24. [Google Scholar]
[7]. Nwosu BU, Hopkins TB, Newborns with the Klinefelter’s syndrome and posterior urethral valvesUrology 2008 72:1033-35. [Google Scholar]
[8]. Chang JT, Chiu PC, Chen YY, Chao MC, Hsieh KS, The 49, XXXXY syndrome with a severe vesico-ureteral reflux and hydronephrosis: the report of one caseActa Paediatrica Taiwanica 2005 46:35-38. [Google Scholar]
[9]. Ozata M, Yesilova Z, Saglam M, Tunca Y, A case of Klinefelter’s syndrome which was associated with unilateral renal aplasiaMed Sci Monit. 2000 6:1000-02. [Google Scholar]
[10]. Barroeta JE, Stopyra GA, The 47,XXY karyotype with associated bilateral renal agenesisArch Pathol Lab Med. 2004 128:44-45. [Google Scholar]
[11]. Matsuoka K, Orikasa H, Eyden B, Yamazaki K, The postmortem diagnosis of occult Klinefelter’s syndrome in a patient with chronic renal disease and liver cirrhosisArch Pathol Lab Med. 2002 126:359-61. [Google Scholar]
[12]. Bojesen A, Juul S, Birkebaek N, Gravholt C, The increased mortality in the Klinefelter’s syndromeJ Clin Endocrinol Metab. 2004 89:3830-34. [Google Scholar]
[13]. Nielsen J, Johansen K, Yde H, The frequency of diabetes mellitus in patients with Klinefelter’s syndrome of different chromosome constitutions and the XYY syndrome. The plasma insulin and the growth hormone levels after a glucose loadJ Clin Endocrinol Metab. 1969 29:1062-73. [Google Scholar]
[14]. Bojesen A, Juul S, Birkebaek N, Gravholt C, Morbidity in the Klinefelter’s syndrome: A Danish register study which was based on the hospital discharge diagnosesJ Clin Endocrinol Metab. 2006 91:1254-60. [Google Scholar]