The Venous Chiasma Between the Basilic Vein and the Brachial Vein: A Case Report
Naveen Kumar1, Ashwini P. Aithal2, Mohandas K.G. Rao3, Satheesha B. Nayak4
1 Lecturer, Melaka Manipal Medical College, Manipal, India.
2 Lecturer, Melaka Manipal Medical College, Manipal, India.
3 Associate Professor, Melaka Manipal Medical College, Manipal, India.
4 Professor and Head of Department of Anatomy, Melaka, Manipal Medical College, Manipal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ms. Ashwini P. Aithal, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal. Karnataka State. INDIA. 576104.
Phone: +919738928345
E-mail: ashwini.anat@gmail.com
Variations in the venous pattern of the arm are common. In this case report, we are presenting the variations of the brachial vein and the basilic vein.
During the routine dissections which were done by medical undergraduate students, we observed some variations in the veins of the upper limb. In the current case, there was only one brachial vein which accompanied the brachial artery. The basilic vein originated from the medial side of the dorsal venous network, ascended along the medial side of the forearm and joined the brachial vein to form the axillary vein at the distal border of the teres major muscle. The basilic vein and the brachial vein joined with one another in the middle of the arm to form a unique venous chiasma.
A large number of invasive procedures are carried out by using the veins of the upper limb, particularly in and distal to the axillary region. This type of a venous chiasma may lead to complications in these procedures.
Venous chiasma, Basilic vein, Brachial vein
Introduction
The basilic vein is one of the superficial veins of the upper limb. It begins from the medial side of the dorsal venous network and ascends in the subcutaneous tissue, along the medial side of the forearm. In its further upward course, the vein accompanies the medial border of the biceps and pierces the deep fascia in the middle of the arm, to pass from superficial to deep.
The brachial veins are usually 2 in number and they are located on either side of the brachial artery. They are usually formed by the union of the radial and the ulnar venae comitantes, near the level of the elbow [1].
Eventually, the brachial vein joins with the basilic vein to form the axillary vein at the distal border of the teres major muscle. We observed variations in the basilic vein and in the brachial vein.
Case Report
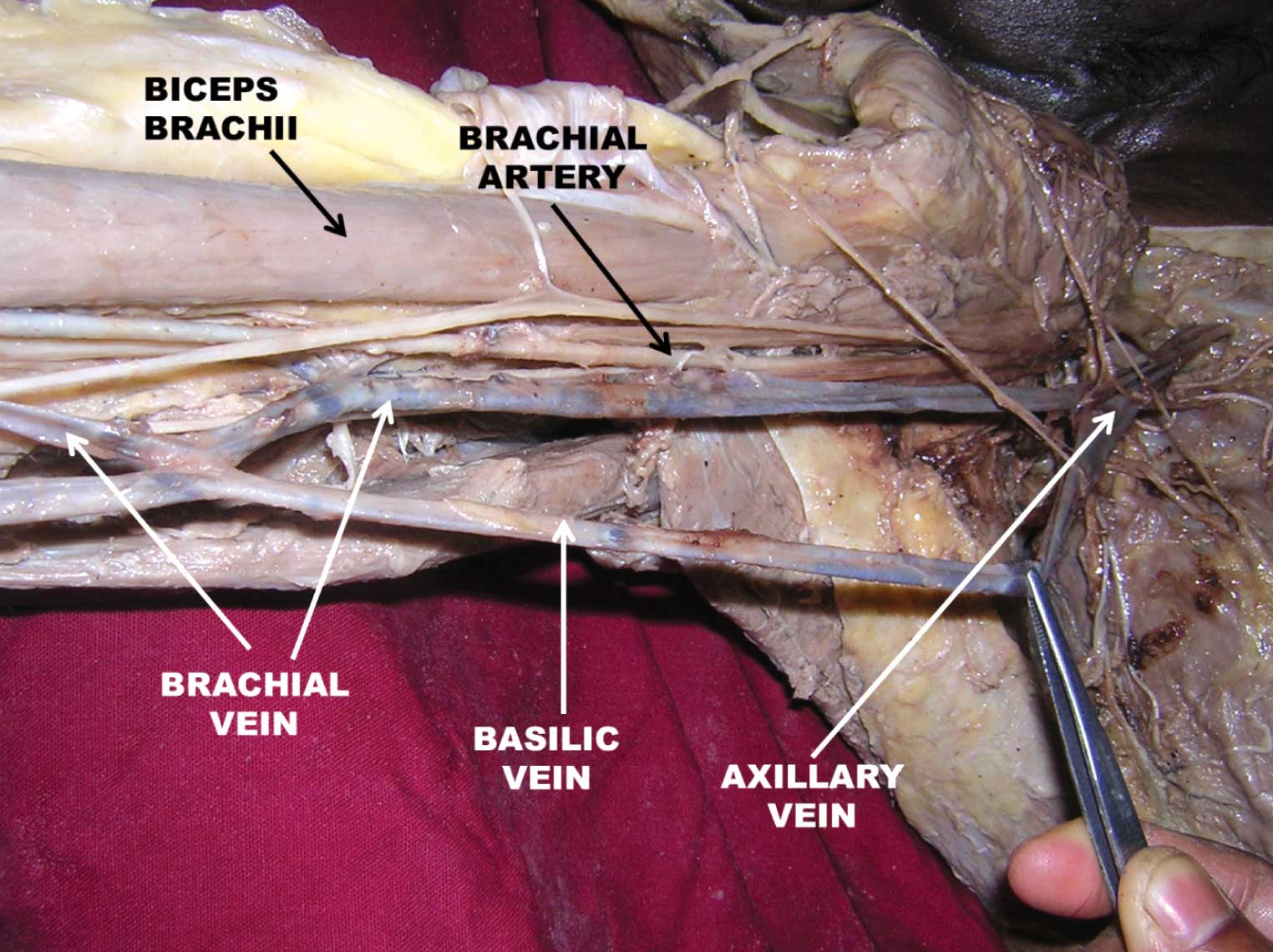
During the routine dissections which were done by medical undergraduate students, we observed the following variations in the right upper limb of a 60 year old male cadaver. There was a single brachial vein which accompanied the brachial artery, instead of the usual venae comitantes. This single brachial vein was formed by the union of a single radial vein and the ulnar vein near the elbow. The brachial vein, at first joined with the basilic vein in the middle of the arm, medial to the biceps brachii muscle, then got divided from it and after a short distance (approx. 13cm), again rejoined with the basilic vein to form a unique chiasmatic pattern before forming the axillary vein in the axilla, at the lower border of the teres major muscle [Table/Fig-1]. These variations were unilateral. There was no variation in the course of the cephalic vein which began from the lateral side of the dorsal venous network, ascended in front of the elbow, then ran lateral to the biceps and thereafter, in the groove between the pectoralis major and the deltoid, pierced the clavipectoral fascia and drained into the axillary vein.
Discussion
The superficial veins of the forearm are subject to great variations, both in the disposition and the size of their trunks and their arrangement. There are very few variations of the basilic vein and the brachial vein which have been reported. A case wherein the brachial-basilic junction was located in an unusual position near the antecubital fossa, leading to an inadvertent distal brachial vein ligation, was reported by Kaiser et al. [2]. In a study which was done by Shima et al. [3], the basilic vein was absent in 0.5% of the cases and in a similar study which was done by Singh et al. [4] it was absent in 1% of the cases. Jose Carlos et al. [5], reported that the basilic vein joined with the medial brachial vein in 53.8% of the cases and that it joined with both the brachial veins in 23.1% of the cases, after which it continued onwards as the axillary vein.
Photograph shows the closer view of the variation. Chiasmatic pattern between basilic vein and brachial vein and also presence of a single brachial vein can be seen.
The brachial vein represents an important route of the collateral circulation of the upper limb, which connects the arm to the axilla and this can be useful in surgeries which are done for the management of a chronic venous insufficiency [6].
In the present case, we observed a single brachial vein instead of the usual venae comitantes. The brachial vein formed a venous chiasma with the basilic vein before forming the axillary vein. When the brachial vein is used as an autogenous vein, its normal course and variations like this must be held in mind [7].
In a case which was reported by Ahmet Songur et al. [8], they mentioned a fenestrated brachial vein which was perforated by the lateral root of the median nerve. Venkat et al. [9], reported a case wherein the brachial vein passed between the two roots of the median nerve and opened into the axillary vein. They presume that such a course might lead to the dilation of the deep veins of the forearm. Anaya Ayala et al., [10] have reported the prevalence of the variant brachial-basilic vein anatomy and their implications for a vascular access planning. Purvis et al., [11] reported in their study, that a segment of brachial vein which contained a competent valve, could be transplanted into a lower extremity vein during a vein valve transplantation operation.
During the early stages of development of the limb, the blood in the terminal capillary plexus returns to the body via a marginal vein. As the limb enlarges, the marginal vein gets subdivided and forms the superficial veins. Deep veins develop in situ, alongside the arteries, by the fusion or the disappearance of few smaller veins [12]. This might result in the formation of a single brachial vein and its chiasmatic pattern of fusion with the basilic vein.
A large number of invasive procedures are carried out by using the veins of the upper limb, particularly in and distal to the axillary region. Cannulation through the basilic vein for cardiac catheterization is preferable because of its continuity with the axillary vein without angulation [13]. We think that this type of a venous chiasma may mislead the cannulation and lead to complications in such procedures.
[1]. Williams PL, Dyson M, Gray’Anatomy38thELBS and Churchill Livingstone:1582 [Google Scholar]
[2]. Kaiser CL, Anaya-Ayala JE, Ismail N, An unrecognized basilica vein variation which led to complications during the basilic vein transposition and the arteriovenous fistula creation: a case report and the implications for an access planningEuropean Journal of Vasc and Endovasc Surg. 2010 39(5):627-29. [Google Scholar]
[3]. Shima H, Ohno K, Shimizu T, An anatomical study on the valves of the superficial veins of the forearmJ. Craniomaxillofac. Surg. 1992 20:305-09. [Google Scholar]
[4]. Singh SP, Ekandem GJ, Bose S, A study on the superficial veins of the cubital fossa in Nigerian subjectsActa Anat. 1982 114:317-20. [Google Scholar]
[5]. Baptista-Silva JCC, Dias AL, Cricenti SV, The anatomy of the basilic vein in the arm and its importance in surgeriesBraz. J. Morphol. Sci. 2003 20(3):171-75. [Google Scholar]
[6]. Gusmao LC, Prates JC, An anatomical study on the accessory axillary veinSurg. Radiol. Anat. 1992 14:131-36. [Google Scholar]
[7]. Bazan HA, Schanzer H, Transposition of the brachial vein: a new source for autologous arteriovenous fistulasJ. Vasc. Surg. 2004 40:184-86. [Google Scholar]
[8]. Songur A, Uygur R, Akçer S, A fenestrated brachial vein being perforated by the lateral root of the median nerve: a case reportAnatomy (International Journal of Experimental and Clinical Anatomy) 2009 3:65-68. [Google Scholar]
[9]. Vollala VR, Potu BK, Gorantla VR, The variant median nerve and the lateral antebrachial cutaneous nerve being associated with the anomalous brachial vein: a case reportNeuroanatomy 2008 7:28-32. [Google Scholar]
[10]. Anaya-Ayala JE, Younes HK, Kaiser CL, Prevalence of the variant brachial-basilic vein anatomy and its implications for a vascular access planningJ Vasc Surg. 2011 53(3):720-24. [Google Scholar]
[11]. Purvis ES II, Hyde GL, Peck D, Anatomy of the arm veins: its significance in vein valve transplantationClin. Anat. 1992 5:45-49. [Google Scholar]
[12]. Sadler TW, Langman's Medical Embryology10th editionLippincott Williams and Wilkins:132 [Google Scholar]
[13]. Snell RS, Clinical Anatomy by Systems8th editionLippincott Williams and Wilkins.:106 [Google Scholar]