Introduction
Neurovascular variations in the upper limb are common and they are well documented. An accurate knowledge of the normal and the variant anatomy of the median nerve and the median artery are important for clinical procedures and for vascular surgeries. The persistant median artery is one such anomaly which was seen in 6.6% (4) of the 60 upper limbs which were dissected in the present study, it being bilateral in one cadaver.
Material and Methods
The present study was conducted on 60 upper limbs of 30 cadavers at the Government Medical College, Amritsar, India. The whole course of the median nerve and the persistant median artery was exposed.
Results
In all the 4 variant limbs, the persistent median artery originated from the anterior interrosseous artery and terminated in the incomplete mediano- ulnar type of the superficial palmar arch. In three upper limbs, the persistant median artery simply accompanied the median nerve upto the palm. But in the left upper limb of the cadaver with the bilateral variation, the artery penetrated and divided the nerve into two halves which joined to form a neural loop around the artery. Thereafter, the nerve and the artery followed the same course upto the palm. Such a penetration of the median nerve by the persistent median artery is extremely rare. Further, its ontogeny and clinical implications have been discussed in detail.
Persistant median artery, Median nerve penetration, Neurovascular variations
Introduction
The median artery is a transitory vessel that represents the arterial axis of the forearm during the early embryonic life. It normally regresses after the second embryonic month to become a small slender artery, the commitansnervi median [1–3]. However, it may persist in 1.1-27.1% of the individuals, as has reported in different studies [4–9]. In most of the cases, it simply accompanies the median nerve which is in the hand, but it may even perforate the median nerve [8,10,11]. The later entity is however rarely seen. While Keen [12] reasoned a persistant median artery to be due to the persistence of an embryonic vessel, Jaschtchinski [13] had called this as an atavistic condition because it is normally found in the palmar arch of certain lower animals. The importance of the persistant median artery lies in the fact that the one with a large calibre may lead to an early compression of the median nerve in the carpal tunnel in patients who are prone to it eg. in myxo-oedema , rheumatoid arthritis, etc. It has also been related to the compressive pathology of the median nerve, which is secondary to arterial calcification [14], thrombosis [15] and atherosclerosis [16]. Turso et al., [17] reported an incomplete, mediano-ulnar type of the superficial palmar arch. In a case report, Ramanathan et al., [18], observed the superficial arterial system which was associated with a palmar type of the median artery in the left limb of a 52 year old cadaver.
The prevalence of the persistent median artery, as has been mentioned above and as was reported by different studies, shows a wide range. This gave us an impetus to design this study, to find out the frequency with which the persistent median artery is found in north Indians and the pattern of its termination wherever it is seen.
Materials and Methods
The present study was conducted on 60 upper limbs which belonged to 30 formalized and preserved cadavers (M:F::28:2) which were obtained from the Department of Anatomy, Government Medical College, Amritsar, Punjab, India. The limbs were dissected as per the dissection guidelines which were given by the Cunningham’s manual of Practical Anatomy [19], to expose the median nerve and its whole course from its formation till its termination. Similiarly, the persistent median artery was traced till its termination.
Results
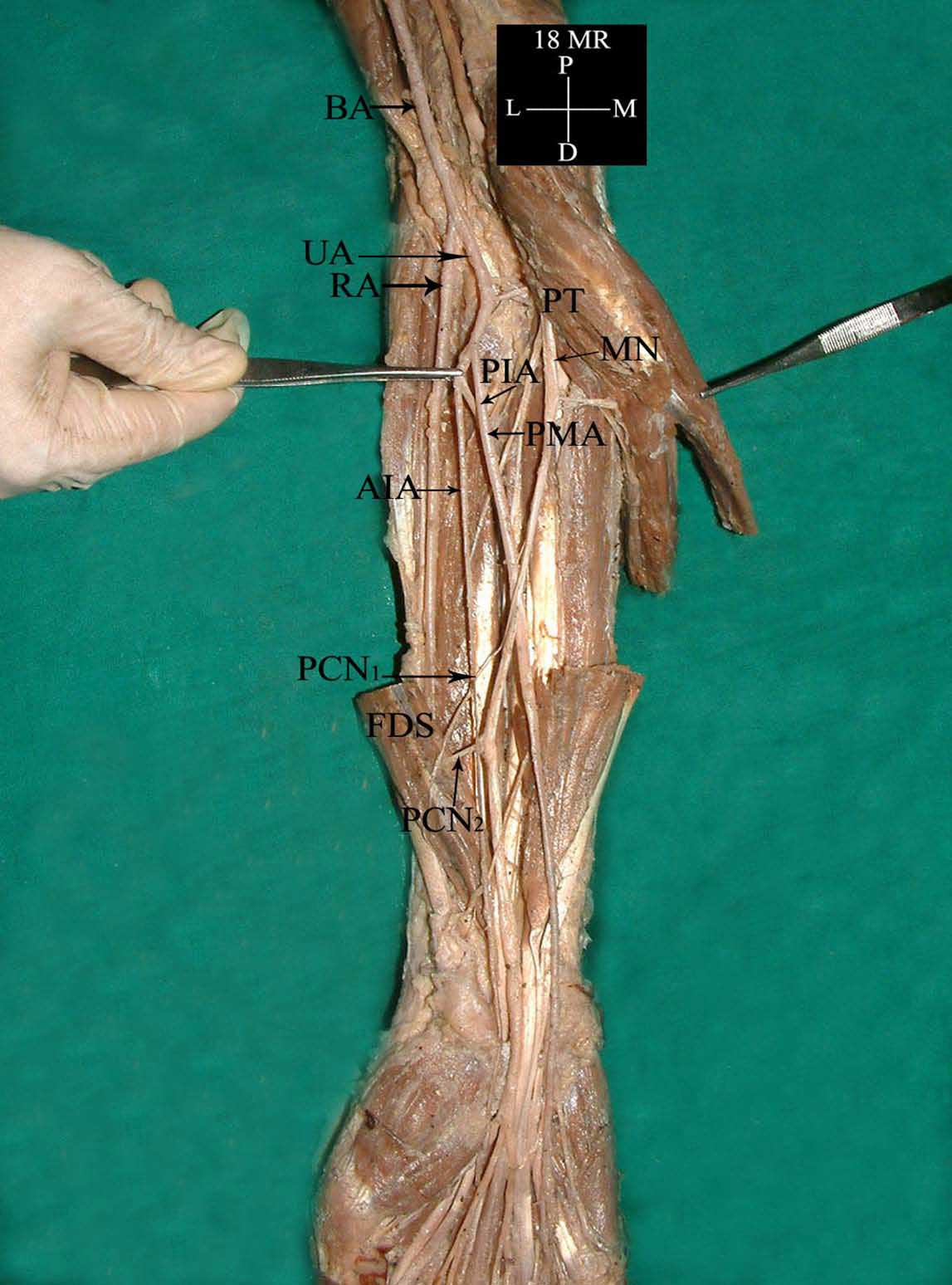
Among the 60 limbs, a persistant median artery was observed in 4 (6.6%) limbs. All the 4 limbs with the persistant median artery belonged to the male sex. In one cadaver, it was found to be bilateral, while among the other 2 limbs, one was found to be on the right side and one was on the left side. In all the limbs, the persistant median artery originated from the anterior interroseousartery, accompanied the median nerve in the forearm and it finally terminated in the hand by forming an incomplete mediano ulnar type of superficial palmar arch [Table/Fig-1]. Apart from this, in the left upper limb of the male cadaver with the bilateral variation [Table/Fig-2], the persistent median artery, after its origin from the anterior interosseous artery, penetrated the median nerve, just distal to its emergence between two heads of the pronator teres muscle and it divided the nerve approximately into two halves. The separated nerve fibres reunited immediately below the site of the penetration, thus forming a neural loop which circumscribed the artery [Table/Fig-2]. Thereafter, the penetrating median artery accompanied the median nerve and it contributed to the formation of the mediano–ulnar type of the superficial palmar arch. A bilateral high and duplicate origin of the palmarcutaneous branch of the median nerve was also observed in the same cadaver [Table/Fig-3].
Photograph of right upper limb showing persistant median artery.(AIA-Anterior interosseousartery,BA-Brachial artery, FDS-Flexor digitorum superficialis, MN-Median nerve, PIA-Posterior interosseousartery, PMA-Persistant median artery, PCN1-Palmar cutaneous nerve, PCN2-Palmar cutaneous nerve, PT-Pronator teres, RA-Radial artery, UA-Ulnar artery)
Photograph of left upper limb showing median nerve penetration by a persistant median artery. (AIA-Anterior interosseousartery, BA-Brachial artery,CFO-Common flexor origin, MN-Median nerve, PT-Pronator teres, PIA-Posterior interosseousartery, PMA-Persistant median artery, UA-Ulnar artery, RA-Radial artery)
Photograph of left upper limb showing persistant median artery penetrating median nerve.(AIA-Anterior interosseous artery, BA-Bachial artery, MN-Median nerve, PIA-Posterior interosseousartery, PTS-Pronator teres superficial head, PTD-Pronator teresdeephead, PCN-Palmar cutaneous nerve, PCN2- Palmar cutaneous nerve, PMA-Persistant median artery, RA-Radial artery, UA-Ulnar artery)
Discussion
The median artery is a transitory artery which develops as an axis artery during the ontogeny of the arteries of upper limb in the early embryonic life, but it usually regresses after the second embryonic month to become a small slender artery [1–3]. However, it may fail to retrogress and then it may accompany the median nerve as a persistant median artery. It usually arises from the anterior interrosseous or the common interroseous and it terminates either in the superficial palmar arch or the palmar carpal arch. Different studies have given different prevalence values of this entity [Table/Fig-4], which have ranged from 1.1–16.1%.
Prevalence of Persistent Median Artery
| Sl. No. | Author | Year | Percentage |
|---|
| 1 | Tandler [20] | 1897 | 16.1 |
| 2 | Jaschtschinski [13] | 1897 | 7.5 |
| 3 | Adachi [5] | 1928 | 8.0 |
| 4 | Gray [21] | 1945 | 1.1 |
| 5 | Misra [22] | 1955 | 8.4 |
| 6 | Coleman and Anson [23] | 1961 | 9.9 |
| 7 | Keen [12] | 1961 | 9.5 |
| 8 | Anson [24] | 1966 | 8.0 |
| 9 | Karlsson and Niechajev [25] | 1982 | 4.0 |
| 10 | Eid et al. [26] | 2011 | 4.0 |
The disparity in the percentage frequency of the prevalence of this artery (1.1–16.1%) can be explained in part by the observation that the median artery frequently joins the superficial palmar arch as a fibrotic thread or as a very tiny vessel, which is barely dissectable. In these cases, the median artery does not contribute any part of the blood supply to the hand.
Ontogeny
The median artery is an important vessel in the embryogenic circulation of the forearm. The continuation of the axial artery in the forearm is at first an anterior interosseous artery. When the latter recedes, it is replaced by its more superficially placed branch, the median artery [27]. Later, it is replaced by the radial and the ulnar arteries. A persistent median artery represents the persistence of an embryonic vessel. This is in consonance with Arey [28], according to whom one of the causes of the anomalous blood vessels is the persistence of the vessels which are normally obliterated.
In humans, the arteries of the upper limb remain separated from the nerves. The blood vessels in the upper limb bud proliferate in the limb bud mesoderm due to the growth of the pre-existing vessels, with a characteristic branching of the vascular cells to form a vascular plexus [29]. A component of this plexus, the axial artery, forms the brachial artery in the arm and it continues as the median artery in the forearm. During this proliferative process, there is a distinct temporal and a spatial succession of the emergence and the regression of paths, so that the individual variations of the forelimb arterial tree are common [30]. So, the present variation may thus be a remnant of the capillary plexus around the median nerve that anastomosed with the anterior interosseous artery [31].
Phylogeny
The growth of a blood vessel at a particular site is necessary for providing nutrition and oxygen to that part of the embryo. An artery which penetrates a nerve is usually considered to be a phylogenetic or a developmental remnant, because this structural feature is common in the lower primates, which correlates with the extreme muscular development and the requisite, extensive blood supply [30].
Clinical Applications
The importance of the persistent median artery lies in the fact that it necessitates the ligation of the radial and the ulnar arteries above its origin or even the ligation of the brachial artery, in cases of wounds of the palm [30,32,33]. A persistent median artery of a large calibre may lead to an early compression of the median nerve in the carpal tunnel in patients who are prone to it e.g. in myxo-oedema, rheumatoid arthritis and pregnancy which leads to the carpal tunnel syndrome [34].
An anomalous artery which penetrates the median nerve in the arm can compress it and produce symptoms of proximal median neuropathy which is similar to the Struthers ligament or a tight bicipitalaponeurosis. The compressive force of the pulsating penetrating artery may produce ischaemia which is distributed unequally in the nerve, damaging those fibres which are destined to become one branch of the median nerve. These nerves are usually weak at the site of the arterial penetration and they are more susceptible to pathological conditions such as diabetes mellitus [31]. This finding may be relevant to the pathologies that require a surgical intervention.
Summary and Conclusion
To summarize, the persistant median artery was seen in 6.6% upper limbs, which has got an ontogenic and a phylogenic implication. Apart from this, clinically, it may be responsible for the carpal tunnel syndrome in patients who are prone to myxoedema, rheumatoid arthritis, etc. A surgeon should be familiar with this variant, as a catastrophe may occur if he encounters such an artery but is unfamiliar with the same.
[1]. DeVriese B, Recherchessur 1’evolution des vaisseauxsanguins des membres chez l’hommeArchives de Biologie 1902 18:665-730. [Google Scholar]
[2]. Singer E, The embryological pattern which persists in the arteries of the armAnatomical Record 1933 55:403-09. [Google Scholar]
[3]. Mrazkova O, Lereseauvasculaire du member superieur etsesrelation savec les muscles pendant l’ontogenesehumaineAngeiologie 1989 41:41-52. [Google Scholar]
[4]. Quain R, The anatomy of the arteries of the human Body 1844 LondonTaylor and Walton [Google Scholar]
[5]. Adachi B, Hasebe K, Adachi B., Das Arteriensystem der JapanerAnatomiederJapaner, vol. 1KyotoVerlag der Kaiserlich-JapanischenUniversitatzu Kyoto:364-372.Cited by Nakatani T, Tanaka S. Absence of the musculocutaneous nerve with innervation of the corocobrachialis, the biceps brachii, the brachialis and the lateral border of the forearm by the branches from the lateral cord of the brachial plexus. J Anat 1997; 49: 459-60. [Google Scholar]
[6]. Mccormack LJ, Cauldwell EW, Anson BJ, Brachialandantebrachial arterial patterns: a study on 750 extremitiesSurg, Gynecol Obst 1953 96:43-54. [Google Scholar]
[7]. Lippert H, Pabst R, Arterial variations in man 1985 New YorkSpringer:68-73. [Google Scholar]
[8]. Srivastava SK, Pande BS, The anomalous pattern of the median artery in the forearm of IndiansActa Anatomica 1990 138:193-94. [Google Scholar]
[9]. Henneberg M, George BJ, A high incidence of the median artery of the forearm in a sample of recent south African cadaversJ. Anat 1992 180:185-88. [Google Scholar]
[10]. Miller RA, Observations on the arrangement of the axillary artery and the brachial plexusAm J Anat 1939 64:143-63. [Google Scholar]
[11]. Spinner M, Cryptogenic infraclavicular brachial plexus neuritis: a preliminary reportBull Hosp Joint Dis 1976 37:98-104. [Google Scholar]
[12]. Keen JA, A study on the arterial variations in the limbs, with a special reference to the symmetry of the vascular patternsAm J Anat 1961 108:245-61. [Google Scholar]
[13]. Jaschtschinski SN, Morphologic and topographic des arcusvolar-issublimis and profundaAnatHefte 1897 7:163-188.Cited by Coleman S Anson J. The arterial pattern in the hand, based upon a study on 650 specimens. Surg Gynaecol Obstet 1961; 113(4): 409-24. [Google Scholar]
[14]. Dickinson JC, Kleinbert JM, Acute carpal-tunnel syndrome which was caused by a calcified median artery. A case reportBone Joint Surg 1991 73:610-11. [Google Scholar]
[15]. Levy M, Pauker M, Carpal tunnel syndrome which was caused by a thrombosed persisting median artery. A case reportThe Hand 1978 10:65-68. [Google Scholar]
[16]. Luyendijk W, The carpal tunnel syndrome: the role of a persistent median arteryActa Neurochirurgica 1986 79:52-57. [Google Scholar]
[17]. Tsuruo Y, Ueyama T, Ito T, Nanjo S, Gyoubu H, Satoh K, Aneurysms of the median artery which cause the recurrent carpal tunnel synrsistant median artery in the hand: A report with a brief review of the literatureAnat Sci Internat 2006 81:242-52. [Google Scholar]
[18]. Ramanathan L, Nayak SR, Vinay KV, Krishnamurthy A, Prabhu LV, Co-existence of the superficial brachio-ulno-radial pattern and the persistant median arteryIndian J Plast Surg 2009 Jan-June42(1):112-14. [Google Scholar]
[19]. Romanes GJ, The pectoral region and the axilla, the arm and the forearm and the handCunninghams Manual of Practical Anatomy 1986 115th EditionEdinburgh, LondonThe English Language Book Society and Oxford University Press:28-89. [Google Scholar]
[20]. Zur Anat Tandler J., omie der arterien derHand Anat Hefter 1897 7:263-83.Cited by Coleman S, Anson J. The arterial pattern in the hand, based upon a study on 650 specimens. Surg Gynaecol Obstet 1961; 113(4): 409-24. [Google Scholar]
[21]. Gray DJ, Some variations which appear in the dissection room. Stanford MBull 1945 3:120-27. [Google Scholar]
[22]. Misra BD, The arteriamedianaJ Anat Soc Ind 1955 4:48 [Google Scholar]
[23]. Coleman S, Anson J, The arterial pattern in the hand, based upon a study on 650 specimensSurg Gynaecol Obstet 1961 113(4):409-24. [Google Scholar]
[24]. Anson BJ, The Cardiovascular and The Nervous SystemMorris Human Anatomy 1966 12th EditionNew YorkThe Blakiston Division McGraw-Hill Book Company:708-24.1060-66 [Google Scholar]
[25]. Karlsson S, Niechajev IA, The arterial anatomy of the upper extremityActa Radiol Diag 1982 23:115-21. [Google Scholar]
[26]. Eid N, Ito Y, Shibata MA, Otsuki Y, The persistant median artery: A cadaveric study and review of the literatureJ Clin Anat 2011 24(5):627-33. [Google Scholar]
[27]. Starch D, Embryologie George Thieme 1955 Stuttgart:529Cited by Keen JA. A study on the arterial variations in the limbs with a special reference to the symmetry of the vascular patterns. Am J Anat 1961; 108: 245-61. [Google Scholar]
[28]. Arey LB, The development of an artery. The peripheral nervous systemA Textbook and Laboratory Manual of Embryology 1957 6th EditionLondonW.B. Saunders Company:375-77.504 [Google Scholar]
[29]. Risau W, Flamme I, VasculogenesisAnn Rev Cell Dev Biol 1995 11:73-91. [Google Scholar]
[30]. Berry MM, Standring S, Bannister LH, Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, The nervous systemGrays’s Anatomy 1995 38th EditionEdinburgh, LondonChurchill Livingstone:1266-74. [Google Scholar]
[31]. Roy TS, Median nerve penetration by a muscular branch of the brachial arteryClin Anat 2003 16:335-39. [Google Scholar]
[32]. Treves FB, Rogers L, The upper extremitySurgical and applied anatomy 1947 11th EditionLondon Toronto, Melbourne and SydneyCassell and Co. Ltd:230-66. [Google Scholar]
[33]. Huber GC, The vascular systemPiersol’s Human Anatomy 1930 9th EditionPhiladelphia, Montreal, LondonJ.B. Lippincott Co.:767-91. [Google Scholar]
[34]. Lister G, Nerve compressionThe hand: Diagnosis and Indications 1977 Edinburgh, LondonChurchill Livingstone:96 [Google Scholar]