Neonatal Salmonella Typhi Meningitis: A Rare Entity
Vikram Singhal1, Saleem EK2, Rajesh SM3, Anita Coutinho4
1 Senior Resident, Kasturba Medical College, Mangalore, Manipal university, India
2 Post Graduate, Kasturba Medical College, Mangalore, Manipal university, India
3 Associate Professor, Kasturba Medical College, Mangalore, Manipal university, India
4 Assistant Professor, Kasturba Medical College, Mangalore, Manipal university, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vikram Singhal, Department of Pediatrics, KMC Hospital, Attavar, Mangalore-575001 Karnataka, India.
Phone: 09972003528,
E-mail: mailkanu@rediffmail.com
Salmonella meningitis is rarely seen in neonates and if it is present, it is associated with complications like subdural collections and abscesses. We are presenting a case of Salmonella meningitis in a 28 days old neonate who developed complications like extensive subdural collections and ventriculitis. The child responded well to prolonged systemic antibiotics and other supportive measures.
Neonate, Meningitis, Complications
Introduction
The invasion of the blood stream, leading to systemic complications, is rarely seen in Salmonella infections. Central nervous system infections which are caused by Salmonella, which lead to complications, is very uncommon in children, that too in infancy [1]. The intracranial infections may vary in presentation from meningitis and subdural effusions on one hand to subdural empyema, epidural empyema and brain abscess on the other [2]. Inspite of the administration of the appropriate antibiotic therapy, the mortality which is associated with Salmonella infections is very high during early infancy and the chance of relapse in the survivors is very high. We are reporting an infant with Salmonella typhi meningitis, with subdural collections, ventriculitis and periventricular ischaemic changes.
Case Report
A 28 day old male neonate presented with fever of three days duration and poor activity, excessive crying and clonic convulsion of one day’s duration. The baby was born at term by caesarean section with a birth weight of 3.8 kg and a head circumference of 35 cm and an uneventful antenatal and postnatal period. Baby was drowsy at the time of admission. The pulse rate was 190 beats per minute, the respiratory rate was 48 per minute, the temperature was 99° F and the weight was 3400 grams. The anterior fontanel was bulging and non-pulsatile, and the head circumference was 38 cm. On neurologic examination, a generalized increased tone, an incomplete moro and a poor suck reflex were observed. The deep tendon reflexes were 3 + bilaterally.
The initial laboratory studies showed: Haemoglobin- 15.8 gm/dL and leukocyte count- 6200/cumm with neutrophilia and a normal platelet count. The serum electrolytes including calcium, the liver function test and the renal function test were normal. The C-reactive protein was positive (80mg/L) and the blood glucose was 124 mg/dL. The Cerebrospinal Fluid (CSF) analysis was suggestive of meningitis, with protein of 927 mg/dL, glucose of 1 mg/dL and 2050 leukocytes per cumm (N-40%, L-52%, E-2%, M-6%). The blood and the CSF culture grew Salmonella typhi. The CT scan at admission showed demyelination of the genu of the corpus callosum, diffuse cerebral oedema with meningeal enhancement and a subdural collection in the bifrontotemporal region which extended into the interhemispheric fissure and the falx.
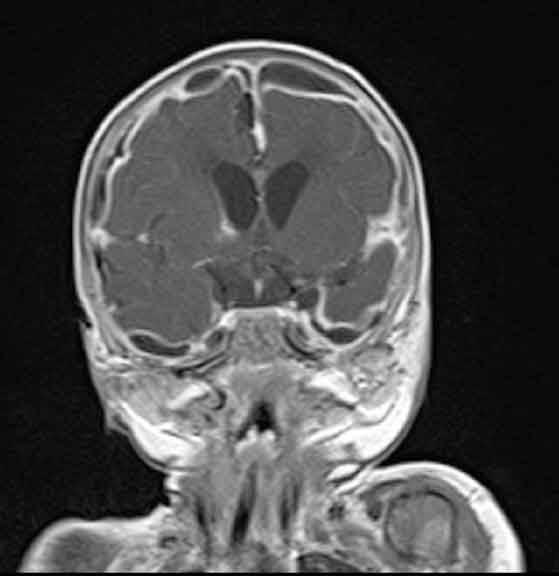
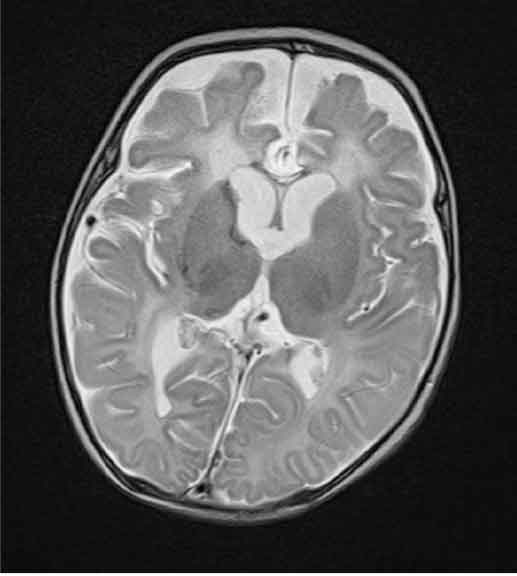
The baby was initially treated with the IV antibiotics, ceftriaxone and amikacin and antiepileptics, iv fluids and symptomatic treatment and he was mechanically ventilated in view of the apnoeic episodes. Inj chloramphenicol was added as per the culture and the sensitivity report. The baby improved after 10 days of treatement and was extubated on day 10 of the ventilation. The mother’s blood culture also grew Salmonella typhi. The baby developed fever and convulsions during the 3rd week of the treatment. The repeat investigations were suggestive of sepsis with an increased total leucocyte count and thrombocytopaenia. But the repeat blood and CSF cultures and the sensitivity were found to be sterile. An MRI of the brain which was done in view of the persistent seizures, showed features which were suggestive of meningitis with a subdural collection in the bifrontal, parietal and interhemispheric fissure and in the middle cranial fossa. Features which were suggestive of ischaemic changes in the bilateral periventricular areas and features of ventriculitis were also present.
[Table/Fig-1] The antibiotics were changed to Meropenem and Netilmycin and they were given for 14 days. A neurosurgery opinion was taken and no active intervention was advised. The anticonvulsant doses were adjusted and the child became afebrile and seizure free and started gaining weight. Now, on follow up, the child’s growth and development was found to have become normal for age. An audiological evaluation which was done at review was found to be normal. The consent of the parents was taken before the reporting of this case was done.
Coronal postcontrast T1 weighted image reveals meningitis with subdural empyaema and ventriculitis
Discussion
With Salmonella infections, focal intracranial infections are unusual. But if intracranial infections occur, they are more common in the paediatric age group. In 1907, Ghon reported the first case of Salmonella meningitis [1]. Upto the year 2002, only around 80 cases of Salmonella meningitis had been reported in the literature [2], with 83 percent of the patients being less than 2 years of age and 50 percent being less than 2 months old [3]. The prognosis and the course of Salmonella meningitis is different from that of other causes of meningitis and it varies from patient to patient. West et al. reviewed the acute neurological complications of Salmonella meningitis and found ventriculitis, subdural empyema, hydrocephalus and chronic neurological abnormalities in as many as 43% cases and a 64% relapse rate [4]. In our case, both the blood and the CSF cultures had grown Salmonella typhi and moreover, the mother’s blood culture also had grown the same organism. Later, an MRI of the brain had shown a subdural collection in the bifrontal, parietal and the interhemispheric fissure and in the middle cranial fossa. Salmonella, being a facultative intracellular micro-organism, the drug penetration is inadequate, which may result in the progression of the infection [5] and also, there is an evidence of an increasing resistance against the commonly used antibiotics, Chloramphenicol, Ampicillin, Cephalosporins and Cotrimoxazole [2,6]. The third generation cephalosporins are the drugs of choice and the duration of the therapy with the parenteral antibiotics should be at least 4 weeks [2,7]. In our case, the chances for relapse and recrudescence were common when the duration of the treatment was inadequate or when ampicillin with either chloramphenicol or cotrimoxazole were used as the initial therapy. Adjunctive dexamethasone may be recommended to attenuate the effects of the acute innate inflammatory response to the bacterial invasion within the CNS, although the benefits of steroids in meningitis seem to be controversial [8]. An early surgical management of the intracranial lesions gives a better prognosis. Although the meningitis in infants is rarely caused by Salmonella, the children who develop Salmonella meningitis may have severe neurological complications and affected neurodevelopment, as Salmonella is an extremely virulent and a pathogenic organism. Hence, a proper antibiotic therapy and a prompt surgical drainage is necessary for a favourable outcome. So, all the patients with pyrexia of unknown origin or prolonged fever should be adequately investigated for the aetiology of Salmonella.
Summary
The major issues which concern the Salmonella intracranial infection are its high mortality, the high treatment failure rates and the significant morbidities in the survivors. A prompt diagnosis of the Salmonella subdural collections, together with an adequate surgical evacuation, and the appropriate choice of the antibiotic at the initial presentation, followed by their prolonged therapy, can improve the outcome significantly.
[1]. Rodriguez RE, Valero V, Watanakunakorn C, Salmonella focal intracranial infections: A review of the world literature (1884-1984) and the report of an unusual caseRev Infect Dis 1986 8:31-41. [Google Scholar]
[2]. Mahapatra AK, Pawar SJ, Sharma RR, Intracranial Salmonella infections: meningitis, subdural collections and brain abscesses. A series of six surgically managed cases with follow-up resultsPediatr Neurosurg 2002 36:8-13. [Google Scholar]
[3]. Henderson LL, Salmonella meningitis- A report of three cases and a review of one hundred and forty four cases from the literatureAm J Dis Child 1948 75(3):351-375. [Google Scholar]
[4]. West SE, Goodkin R, Kaplan A, Neonatal Salmonella meningitis which was complicated by cerebral abscessesWest J Med 1977 127:142-145. [Google Scholar]
[5]. Torrey S, Fleisher G, Jaffe D, The incidence of Salmonella bacteremia in infants with Salmonella gastroenteritisJ Pediatr 1986 108:718-721. [Google Scholar]
[6]. Levin CS, The treatment of multi-resistant Salmonella infectionsLancet 1991 47:337 [Google Scholar]
[7]. American Academy of PediatricsCommittee on infectious diseases. Salmonella infectionsRed Book 2000: Report of the Committee on Infectious Diseases 2000 25th ed.Elk Grove, ILAmerican Academy of Pediatrics:501-6. [Google Scholar]
[8]. Quagliarello V, Scheld WM, Infectious diseases: do steroids benefit patients with bacterial meningitis?Nat Rev Neurol 2010 6(10):529-30. [Google Scholar]