Isolated Diffuse Hyperplastic Gastric Polyposis: A Rare Case
Meenakshisundaram1
1 Associate Professor, Department of Pathology, Saveetha Medical CollegeThandalam, Chennai- 602105, Tamilnadu, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Meenakshisundaram, Associate Professor, Department of Pathology, Saveetha Medical College, Thandalam, Chennai- 602105, India.
Phone: 09444161999,
E-mail: drkms75@gmail.com
The gastric polyps are rare as compared to the colonic polyps. Multiple gastric polyps are seen in association with other polyposis syndromes like juvenile polyposis, Gardner's syndrome, the Peutz-Jeghers syndrome and the Cronkhite-Canada syndrome. Diffuse gastric polyposis is a rare entity and only few cases have been reported. The mode of treatment is surgery, either total or near total gastrectomy and a careful followup of the patient is needed due to the risk of colorectal malignancy.
Diffuse Hyperplastic Gastric Polyposis
Case Report
A 20-year old female presented with abdominal pain of eighteen months duration. The pain was intermittent, colicky and non-radiating, it was located in the epigastric region and it was relieved by the use of medications. The investigations showed a haemoglobin value of 7.6gm. The peripheral blood smears showed a microcytic hypochromic blood picture. Serum iron and ferritin were reduced, with an increase in the total iron binding capacity. Upper GI endoscopy showed multiple polyps in the stomach. The oesophagus was normal. Colonoscopy showed no polyps. Pre-operatively, the duodenum and the small intestines were found to be normal. Total gastrectomy was done.
Pathological findings
The total gastrectomy specimen measured 9cm along the lesser curvature and 15cm along the greater curvature. The lumen showed multiple polyps – pedunculated and sessile, of varying sizes, which ranged from 0.3cm to 2.5cm in diameter. The surface of few polyps showed ulceration and congestion [Table/Fig-1].
Gastrectomy specimen with multiple sessile and pedunculated polyps.

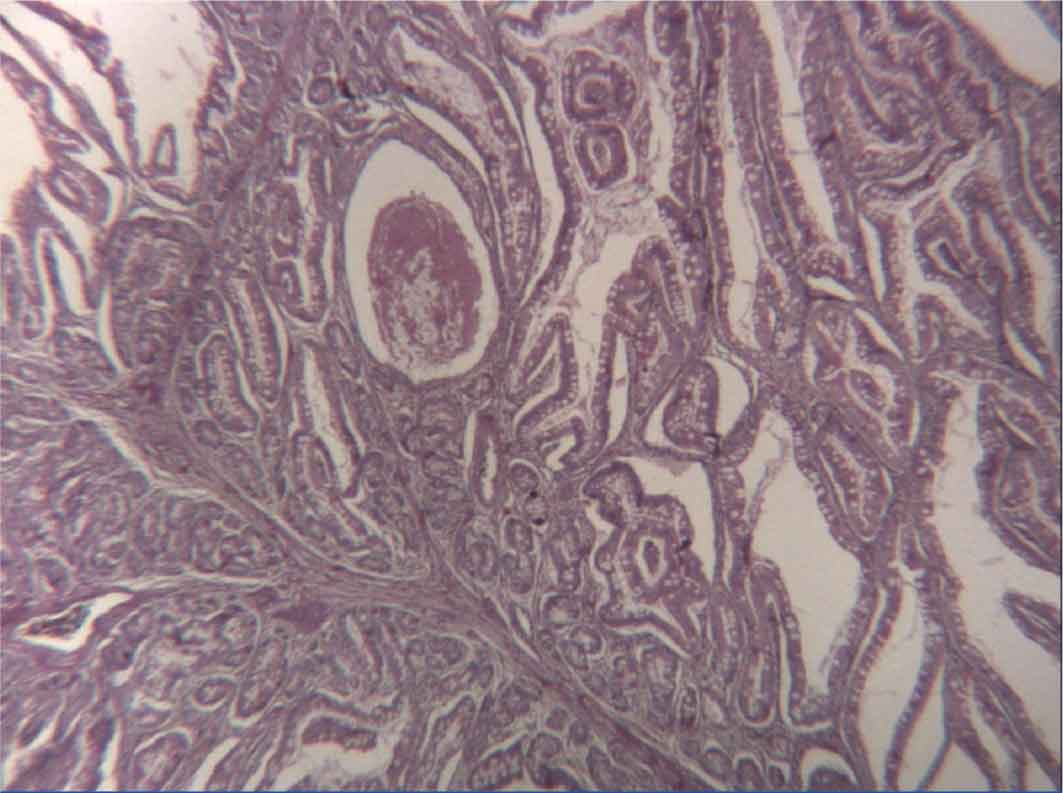
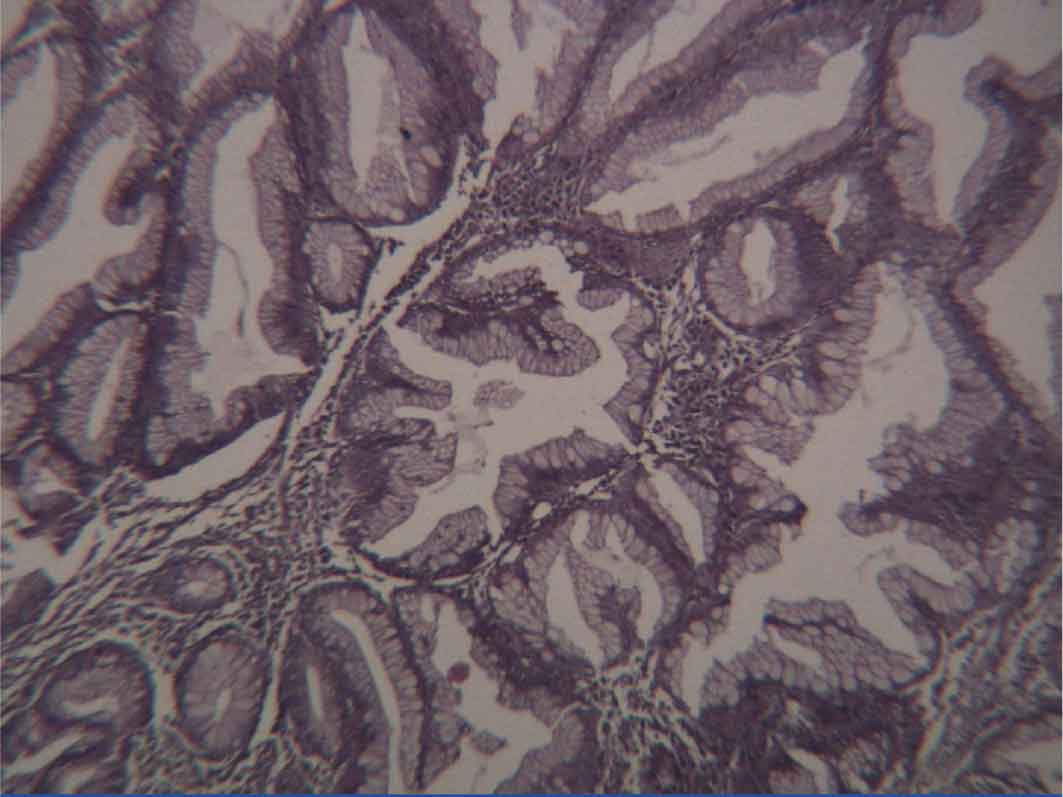
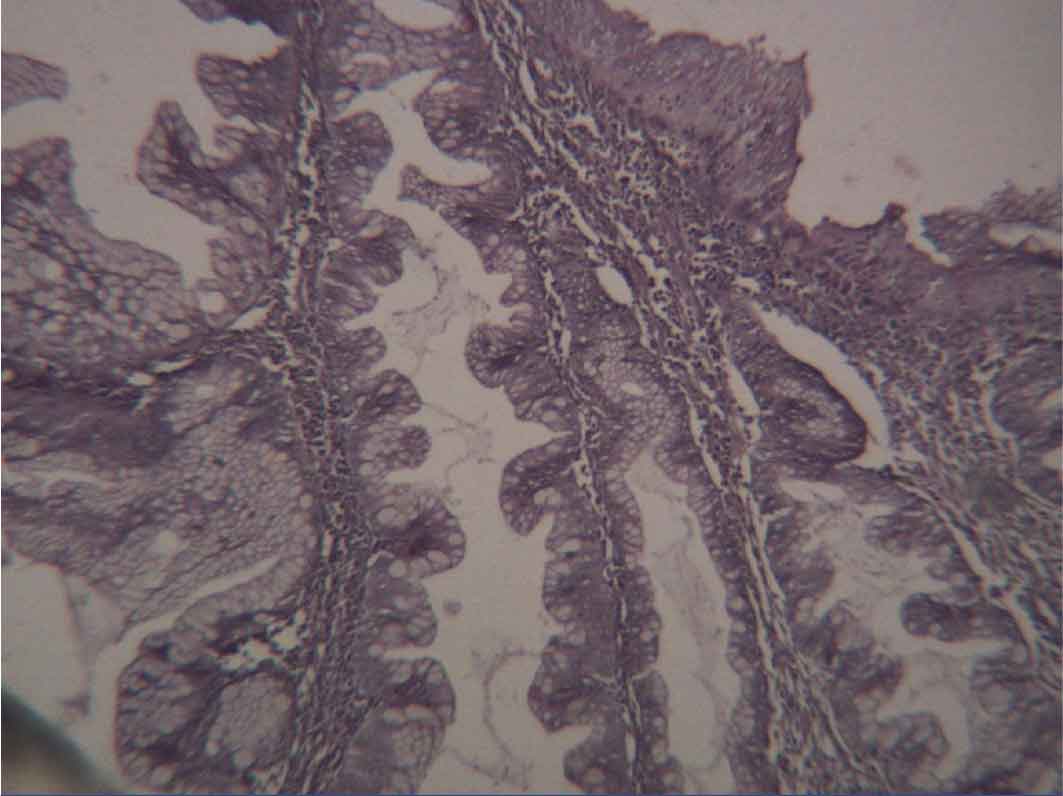
The microscopic examination showed numerous dilated glands which were lined by columnar cells with abundant mucinous cytoplasm and basally placed nuclei. A corkscrew appearance was seen in many glands as a result of the infolding of the epithelium. No dysplasia was seen. No evidence of malignancy was seen
[Table/Fig-2], [Table/Fig-3] and [Table/Fig-4]. The special stains which were done for Helicobacter pylori were negative.
Microscopy revealed varying sized glands with few of them dilated. [H&E stain 10X]
Microscopic picture showed corkscrew appearance. [H&E stain 10X]
Microscopic picture showed glands are lined by columnar cells with abundant mucin with infoldings giving a corkscrew appearance. No atypia seen. [H&E stain 40X]
Discussion
Polyps are defined as nodules or masses that project above the mucosal surface into the gastric or the colonic lumen [1]. The gastric polyps are rare as compared to the colonic polyps [2].
The polyps in the stomach may develop as a result of epithelial or stromal hyperplasia, inflammation, ectopia or neoplasia [3]. Gastric polyps are classified into non-neoplastic polyps, neoplastic polyps and miscellaneous lesions with polypoidal growth patterns. The non-neoplastic polyps include hyperplastic polyps, inflammatory polyps and hamartomatous polyps. The neoplastic polyps include adenomas, carcinomas and carcinoids. The other lesions that protrude into the lumen are lymphoid hyperplasias/lymphomas, mesenchymal stromal tumours and vascular tumours [4]. The hyperplastic polyps are the most common type of gastric polyps [5].
Most of the hyperplastic polyps develop in chronic gastritis patients as a result of the exaggerated mucosal healing response through the stages of hyperplasia and polypoidal hyperplasia, which result in hyperplastic polyps. An important predisposing factor is Helicobacter pylori gastritis. The non-Helicobacter causes are chemical or reactive gastritis [5]. The hyperplastic polyps have a wide age range distribution and they are common in females, as it was in our case. These are randomly distributed in the stomach- antrum, the fundus and the cardia [5]. Our case did not show any evidence of the Helicobacter infection.
A majority of the polyps are single and most of them are less than 0.5cm in size. Rarely can more than 50 polyps be seen and the diagnosis of hyperplastic polyposis can be given. Our case also showed more than 70 polyps of varying sizes [5]. Gastric polyposis can present with iron deficiency anaemia, hypoproteinaemia, high gastrin levels and gastric outlet obstruction [6]. Our patient had iron deficiency anaemia but with normal gastrin levels.
The long term use of proton pump inhibitors is associated with the development of gastric polyposis in children [7]. Our case did not have a history of the prolonged intake of proton pump inhibitors. Hyperplastic polyps do not have the risk of malignancy in the stomach. But the risk increases when they are associated with pernicious anaemia [8]. Hyperplastic polyposis is associated with colorectal malignancy [9]. In our case, proctosigmoidoscopy and colonoscopy showed normal results. Since the risk is there, she is still under constant surveillance.
Summary
Isolated hyperplastic gastric polyposis is a rare entity and only few cases have been reported in the literature. This case was of particular interest because the patient presented with abdominal pain alone and the investigations showed multiple polyps in the stomach with a normal picture of the remaining gastrointestinal tract. The patients with this disease are at a risk of development of gastric malignancy or colorectal malignancy and hence they need constant surveillance.
[1]. Stricker TP, Kumar V, NeoplasiaThe pathologic basis of disease 2010 8th edition:261 [Google Scholar]
[2]. Scott – Conner CEH: Benign Gastric Tumours. eMedicine 2006 [Google Scholar]
[3]. Turner JR, The Gastrointestinal tractThe pathologic basis of disease 2010 8th edition:783 [Google Scholar]
[4]. Park DY, Gregory, Lauwers, Gastric polyps – classification and managementArch Pathol Lab Med. 2008 132:633-40. [Google Scholar]
[5]. Turner JR, Odze RD, Polyps of the stomachSurgical Pathology of the GIT, liver, biliary tract and the pancreas 2009 2nd edition:416 [Google Scholar]
[6]. Kepczyk T, Kadakia SC, A prospective evaluation of gastrointestinal tract patients with iron deficiency anemiaDig Dis Sci 1995 40(6):1283-89. [Google Scholar]
[7]. Pashankar DS, Israel DM, Gastric polyps and nodules in children who received long term omeprazole therapyJ Pediatr Gastroenterol Nutr 2002 35(5):658-62. [Google Scholar]
[8]. Rickes S, Gerl H, Lochs H, Gastric polyps in pernicious anemia : indications for polypectomyDtsch Med Wochenschr 2000 125(36):1035-38. [Google Scholar]
[9]. Niv Y, Delpre G, Sperber AD, Hyperplastic gastric polyposis, hypergastrinemia and colorectal neoplasia : a description of four casesEur J Gasteroenterol Hepatol 2003 15(12):1361-66. [Google Scholar]