Idiopathic Giant Cell Myocarditis: A Case Report
Kalpana Kumari M.K.1, Vijaya V. Mysorekar2, Praveen S.3
1 Associate Professor, Department of Pathology, MS Ramaiah Medical College, Karnataka, India
2 Senior Professor, Department of Pathology, MS Ramaiah Medical College, Karnataka, India
3 Associate Professor, Department of Forensic Medicine, MS Ramaiah Medical College, Karnataka, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kalpana Kumari M.K., Flat No. 710, C-Block, Sterling Residency, Dollors Colony, RMV IInd stage, Bangalore-560094, Karnataka (India).
Phone: 9886392301,
E-mail: kalpank@gmail.com
Giant-cell myocarditis is a disease of relatively young, predominantly healthy adults. The patients usually die of heart failure and ventricular arrhythmia unless a cardiac transplantation is performed. We are reporting here an autopsy case of idiopathic giant cell myocarditis with no symptoms in a 27-year old -worker who died suddenly.
The purpose of this report was to emphasize that idiopathic giant cell myocarditis was a rare disease and that it could exist in the absence of any symptomatic heart disease.
Idiopathic giant cell myocarditis, Sudden death, Giant cells
Introduction
Myocarditis is a group of pathologic entities in which infectious micro-organisms and/or inflammatory processes cause myocardial injury [1]. A rare type of this disease is idiopathic giant cell myocarditis [2]. Giant-cell myocarditis is a disease of relatively young, predominantly healthy adults. The patients usually die of heart failure and ventricular arrhythmia unless a cardiac transplantation is performed [3].
The incidence of giant cell myocarditis is low and it varies with the population which is being studied and the method of diagnosis which is used. In a Japanese autopsy registry, the incidence of giant cell myocarditis was 0.007% (25 of 377,841 cases from 1958 to 1977). The incidence of giant cell myocarditis was a similarly low (3 of 12,815 necropsies) in the period from 1950 to 1963 at the Oxford Infirmary [4].
Case Report
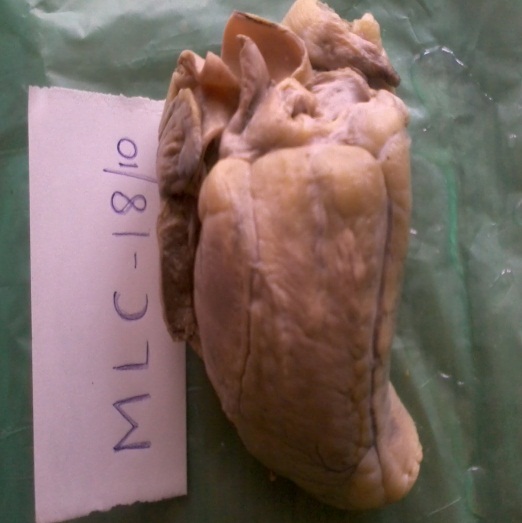
A 27-year old male with no history of any medical or surgical illness was found dead in his house and a postmortem was performed. An external examination revealed no abnormality heart weighed 250gm. The ventricular wall thickness was normal and the right coronary artery and the left circumflex coronary artery were patent. The left anterior descending artery wall was thickened and the lumen was obliterated. Gray white patches were seen on the anterior wall of the left ventricle, the largest measuring 2×2×1 cms, throughout the full thickness of the myocardium [Table/Fig-1]. The lung weighed 200gm, the external surface was unremarkable and the cut surface was congested. All the other organs were unremarkable.
Gross Appearance of Heart–Shows Multiple Greywhite Lesions on the Anterior Surface
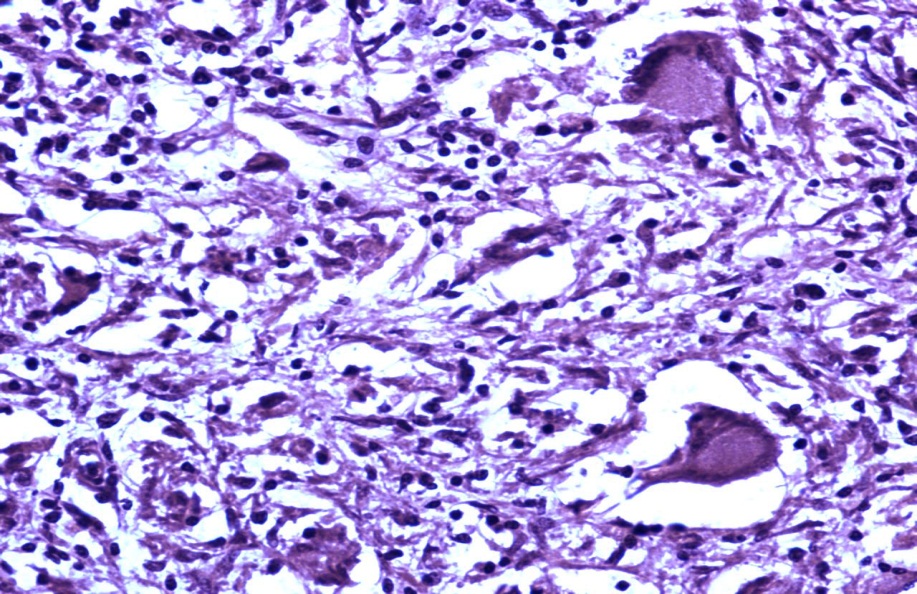
Microscopy of the myocardium revealed a diffuse inflammatory infiltrate which consisted of giant cells which were interspersed with lymphocytes, plasma cells, eosinophils and macrophages, with extensive myocyte necrosis [Table/Fig-2]. The cytoplasm of the the giant cells lacked asteroid bodies, Schaumann bodies or any fungi. The left anterior descending artery showed an atheromatous plaque which caused 30%-40% luminal occlusion. The pericardium and the endocardium were normal. No viral cytopathic effect was seen. Fite staining did not reveal any acid fast bacilli. Sections from the lung showed features of pulmonary oedema and haemorrhage. No granulomatous reaction was seen. A diagnosis of idiopathic giant cell myocarditis with pulmonary oedema and haemorrhage was made.
High Powerview 40 x H&E-Shows Giant Cells Amidst Dense Mixed Inflammtory Infitrate
Discussion
Sudden cardiac death is defined as an unexpected death which results from cardiac causes in individuals without heart disease or with an early after symptom onset, usually within 1 hour [5]. Idiopathic giant cell myocarditis is a rare clinicopathological entity which is usually known to cause death in more than half of the cases of sudden death [6].
The literature supports our finding that giant-cell myocarditis is a disease of young adults. The youngest reported patient was 6 weeks old and the average ages in two previously reported series were 37 years (5 patients) and 48 years (5 patients). The oldest reported patient was 88-years old [3]. The less number of reported cases in the elderly indicates a less frequent diagnosis or a less fulminant course of the disease.
Many disorders cause myocardial granulomas with associated giant cells, which may be mistaken for idiopathic giant cell myocarditis. The Aschoff lesions of rheumatic myocarditis evolve into characteristic, focal interstitial granulomas with giant cells. Tuberculosis and cryptococcosis also have giant cells within the granulomatous lesions. Special stains for the organisms should be performed whenever there is a suspicion of an infection. Rarely, giant cells may be seen in syphilitic myocarditis. Foreign body reaction, Wegener granulomatosis, and systemic sarcoidosis must be considered in the differential diagnosis as well. These disorders usually have distinct clinical presentations and the appropriate diagnostic studies can usually prevent their confusion with idiopathic giant cell myocarditis [4].
Numerous autoimmune disorders have been associated with giant-cell myocarditis as has been seen in the various case reports. But our case did not have any history of autoimmune disease. A majority of the cases of giant-cell myocarditis occur in otherwise healthy persons (81%) [3]. When the symptoms are present, the major symptom is rapidly progressive heart failure or concomitant ventricular arrhythmia [3]. Our case was completely asymptomatic.
Aetiology
The aetiology of giant cell myocarditis is unknown. No viral trigger has been demonstrated. Myocarditis which resembles human giant cell myocarditis can be induced in the Lewis rat by immunization with cardiac myosin, thus supporting the suspicion of an autoimmune mechanism. The principal infiltrating lymphocyte in the experimental giant cell myocarditis is the CD4+ T cell, unlike the murine viral myocarditis in which the CD8+ T cell is predominant. In human acute giant cell myocarditis, the CD8+ cells outnumber the CD4+ cells, but the CD4+:CD8+ ratio can vary with the stage of disease. Prominent eosinophilia is common in acute human giant cell myocarditis. An experimental transfer via serum or the IgG fractions is unsuccessful, thus implying the central role of the T cells in initiating a myocardial damage. The hypothesis that human giant cell myocarditis is also of an autoimmune aetiology, is supported by reports of its frequent association with autoimmune or inflammatory conditions in up to 20% of the cases, which include ulcerative colitis, Crohn’s disease, Hashimoto thyroiditis, myasthenia gravis, and different forms of inflammatory arthritis. Giant cell myocarditis has been associated with hypersensitivity reactions and cancers which include lymphoma, sarcoma, lung cancer, and thymoma [7].
Unlike in acute myocarditis, the prognosis in giant cell myocarditis is poor [8,9]. Its high morbidity and mortality are due to its refractory response to all forms of treatment, which include combined immuno-suppressive drugs. For the patients who are unresponsive to the medical therapy, cardiac transplantation remains the only viable option, despite the risk of recurrence in the transplanted heart [9].
Conclusion
In cases of sudden death in young individuals, a careful search for a histological evidence of idiopathic giant cell myocarditis is essential, after ruling out acute myocardial infarction. An endomyocardial biopsy is a must for the diagnose idiopathic giant cell myocarditis in young patients with arrthymias who do not respond to the treatment.
[1]. Magnani JW, Dec GW, Myocarditis: the current trends in its diagnosis and treatmentCirculation 2006 113:876-90. [Google Scholar]
[2]. Momin YA, Raghuvanshi SR, Lanjewar DN, Idiopathic giant cell myocarditis leading to sudden death - A case reportBombay Hosp J. 2008 50:288-89. [Google Scholar]
[3]. Cooper LT, JrBerry GJ, Shabetai R, Idiopathic giant cell myocarditis -Natural history and treatment. Multicenter Giant Cell Myocarditis Study Group InvestigatorsN Engl J Med. 1997 26:1860-66. [Google Scholar]
[4]. December GW, Cooper LT, Jr.Introduction to clinical myocarditisMyocarditis from the bench to the bedside 2003 TotowaHumana Pres.:257-81. [Google Scholar]
[5]. Schoen FJ, The heartChapter 12, Robbins and Cotran Pathologic Basis of Disease 2010 8edPennsylvaniaElsevier:555-618. [Google Scholar]
[6]. Konapur PG, Daded AV, Udaykumar M, Idiopathic giant cell myocarditis: a case report and review of the literatureIndian Journal of Pathology and Microbiology 2003 36:241-43. [Google Scholar]
[7]. Laufs H, Nigrovic PA, Schneider LC, Oettgen H, Del NP, Moskowitz IP, Giant cell myocarditis in a 12-year-old girl with a common variable immunodeficiencyMayo Clin Proc. 2002 77:92-6. [Google Scholar]
[8]. HooKim K, De Roux S, Igbokwe A, Stanek A, Koo J, Hsu J, Bluth MH IgG anti-cardiomyocyte antibodies in giant cell myocarditisAnn Clin Lab Sci. 2008 38:83-87. [Google Scholar]
[9]. Blauwet LA, Cooper LT, MyocarditisProg Cardiovasc Dis. 2010 52:274-88. [Google Scholar]