Pseudocarcinomatous Hyperplasia of the Fallopian Tubes which was Associated with Female Genital Tract Tuberculosis, Histologically Mimicking Tubal Adenocarcinoma: A Diagnostic Challenge
Sonam Gupta1, Prem Singh2, Jyoti Bala3, Deeba Mushtaq4, Ankita Goyal5
1 Resident, MM Institute of Medical Sciences & Research, Mullana, Ambala: Haryana, India
2 Associate Professor, MM Institute of Medical Sciences & Research, Mullana, Ambala: Haryana, India
3 Assistant Professor, MM Institute of Medical Sciences & Research, Mullana, Ambala: Haryana, India
4 Assistant Professor, MM Institute of Medical Sciences & Research, Mullana, Ambala: Haryana, India
5 Assistant Professor, MM Institute of Medical Sciences & Research, Mullana, Ambala: Haryana, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prem Singh, House No-474, Sector-7, Urban Estate, Karnal, Haryana - 132001.
Phone: 918950204113,
E-mail: premsingh011@rediffmail.com
The benign proliferative and reactive processes of the fallopian tubes which are a result of female genital tract tuberculosis can mimick malignant neoplasms, both clinically and pathologically. ‘Pseudocarcinomatous hyperplasia’ is a term which is applied to the florid form of epithelial hyperplasia with atypical features, that mimicks tubal adenocarcinoma. It may be encountered in the tuberculous and the non tuberculous forms of chronic salphingitis. We are reporting a case of a 30 years old female who presented to our institute with complaints of vaginal discharge and fever. She underwent panhysterectomy for uterine fibroids. Both her fallopian tubes revealed features of florid atypical epithelial hyperplasia, along with widespread caseating granulomatas. Ziehl Neelsen (ZN) staining of the lesion for acid fast bacilli (AFB) was positive. A diagnosis of pseudocarcinomatous hyperplasia of the fallopian tubes which was associated with female genital tract tuberculosis, which histologically mimicked tubal adenocarcinoma was made, which posed a diagnostic dilemma.
Pseudocarcinomatous hyperplasia, Tuberculosis, Adenocarcinoma, Fallopian tubes
Introduction
Many benign hyperplastic and reactive processes may occur in the fallopian tubes, which can be mistaken for a neoplasm, both clinically and pathologically. A florid form of epithelial hyperplasia which affects the fallopian tubes, that mimicks tubal adenocarcinoma, has been termed as ‘pseudocarcinomatous hyperplasia’. It may be encountered in tubercular salpingitis and non tubercular salpingitis and it is characterized by the crowding and the stratification of the epithelium and gland formation with a cribriform pattern. It may be associated with the glandular infiltration of the muscular layer with desmoplastic reactive pseudoglandular hyperplasia of the tubal serosal mesothelial cells, mimicking the transmural extension of a carcinoma. Sometimes, chronic inflammation with a granulomatous reaction may also be seen in tubal carcinoma, which may sometimes be difficult to differentiate from the reactive atypical hyperplasia which is seen in tubercular salpingitis [1].
Case Report
A 35 years old female gravida 10 and para 3 reported to this institute with a history of persistent discharge per vaginum, dysmenorrhoea and oligomenorrhoea since one year. She had been having fever for the past one month. The patient had undergone five medical termination of pregnancies along with two spontaneous abortions in the past. On physical examination, she was found to be febrile. Her systemic examination showed a normal picture and there was no evidence of tuberculosis. There was no organomegaly. Her pelvic ultrasound examination revealed two uterine fibroids and dilated fallopian tubes. Hysterosalpingography showed a diffuse dilatation of both the fallopian tubes. She underwent panhysterectomy for the fibroids as a part of the treatment.
Gross Examination
The panhysterectomy specimen revealed two, small, intramural uterine fibroids. Both the fallopian tubes were grossly dilated and thickened [Table/Fig-1]. The cut surface of the fallopian tubes revealed a friable mucosa with papillary fronds and foci of caseous necrosis [Table/Fig-1] (inset). There was no gross evidence of any tumour.
Panhysterectomy specimen showing grossly dilated and enlarged fallopian tubes. Inset showing mucosal tufting and focal areas of caseation.

Microscopic Examination
Her endometrium and ovaries showed multiple granulomatas. There was no evidence of endometrial hyperplasia or carcinoma. The fallopian tubes revealed stratification of the epithelium, tufting with cribriforming and gland formation. Nuclear atypia with occasional mitotic figures was seen. There was a glandular infiltration of the muscularis propria [Table/Fig-2 & 3]. Both the fallopian tubes showed widespread granulomatas which were composed of epithelioid cells, Langhans giant cells, lymphocytes and plasma cells with areas of caseous necrosis [Table/Fig-4]. The presence of granulomatas was also seen on the surface of the fallopian tubes and in the wall [Table/Fig-2]. ZN staining for AFB was positive. A final diagnosis of pseudocarcinomatous hyperplasia of the fallopian tubes which was associated with female genital tract tuberculosis was made.
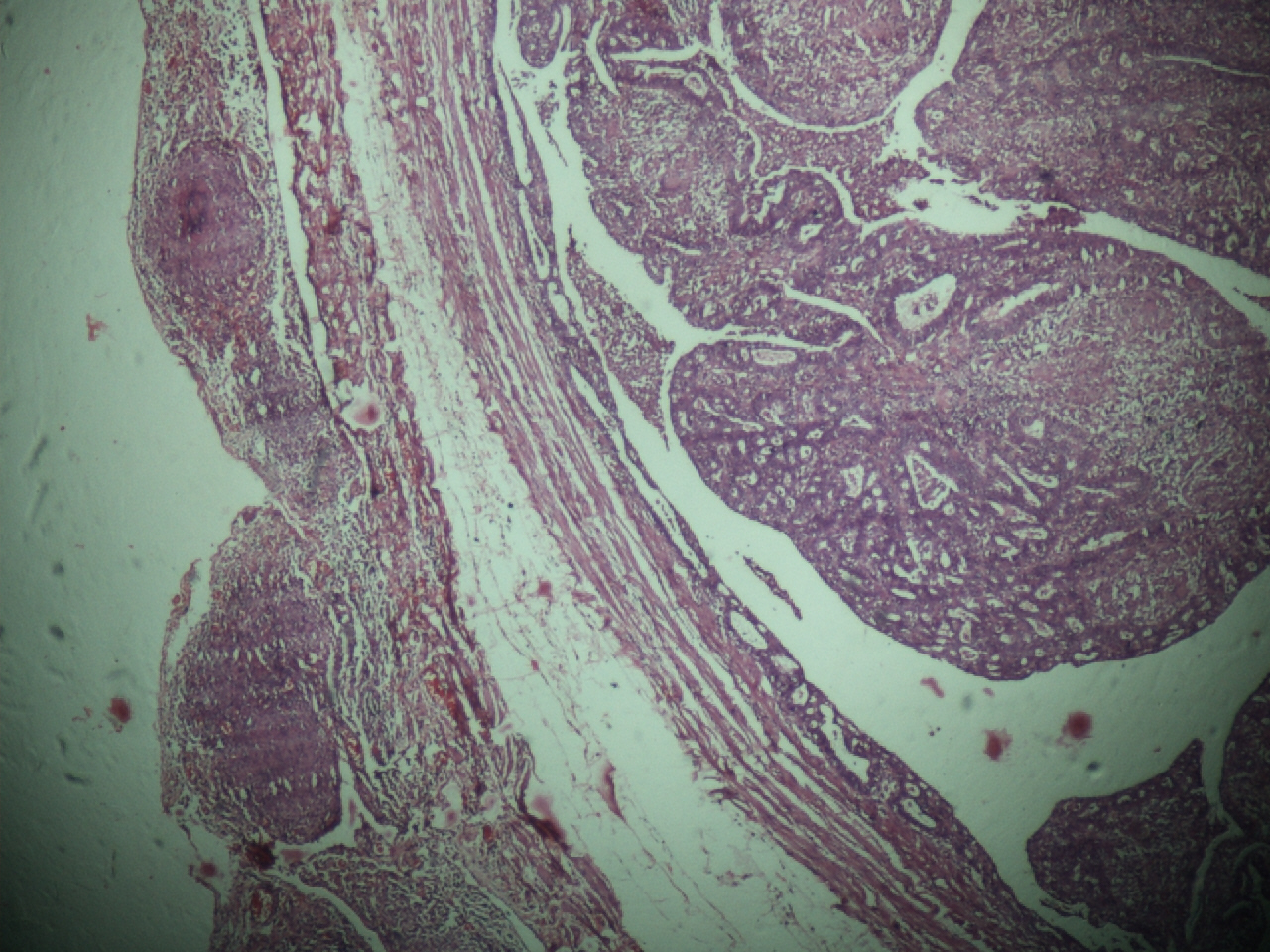
Pseudocarcinomatous hyperplasia of the fallopian tube. Marked mucosal proliferation with cribriform pattern. The serosa shows presence of granulomas. Invasion of the muscular wall with glandular epithelium is seen. (H&E, × 40)
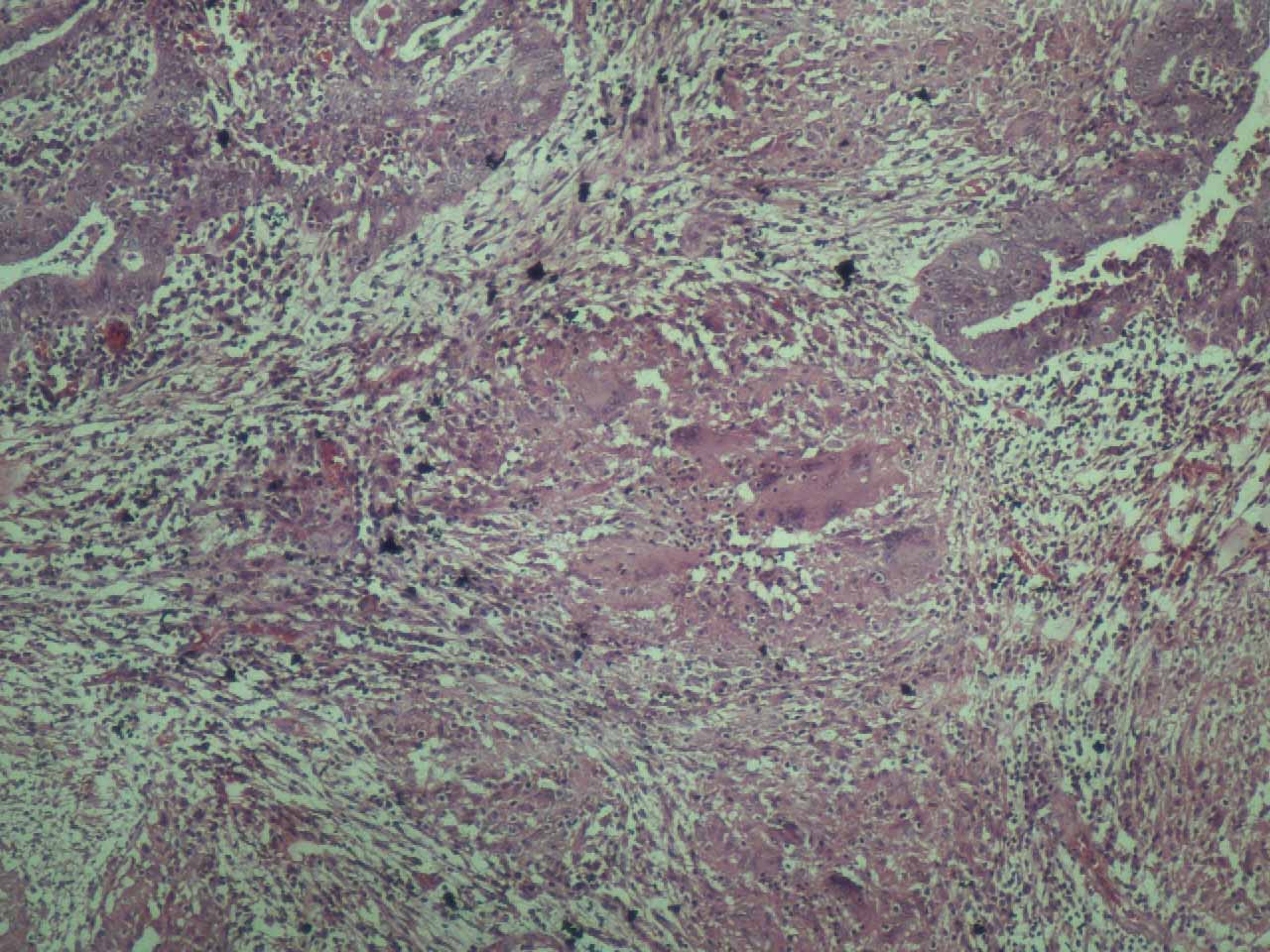
Marked mucosal proliferation and granulomatas composed of epithelioid cells and Langhan's giant cells. Focal areas of caseation are seen. (H&E, × 200).
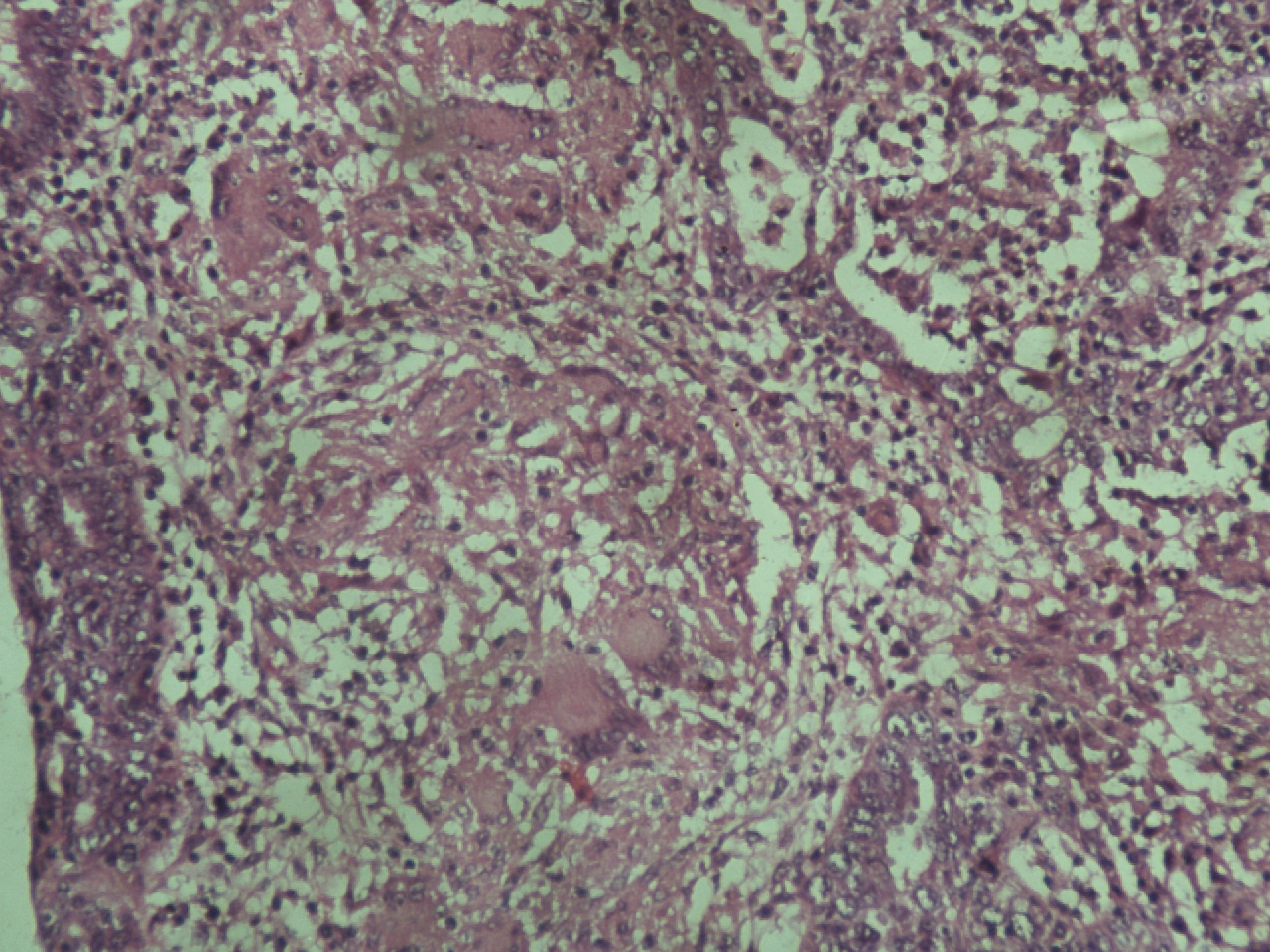
Crowding and stratification of epithelium with gland formation, nuclear atypia and a mitotic figure seen in the right lower part of the field. Center of the field shows granuloma with numerous giant cells. (H&E, × 200)
Discussion
The florid form of epithelial hyperplasia which accompanies a recurrent, non tuberculous inflammation of the fallopian tubes was first described by Dougherty and Cotten in 1964 [2]. Subsequently, Cheung and collegues emphasized the association of various forms of chronic salpingitis, which included tubercular salpingitis, with hyperplastic tubal mucosal lesions which are occasionally difficult to differentiate histologically from adenocarcinoma [3]. Moore and Enterline noted the presence of epithelial hyperplasia in 18.5% cases of surgically resected fallopian tubes which showed associated salpingitis in 50% of the cases [4]. The prevalence and the clinical significance of hyperplastic mucosal epithelial proliferations are controversial, with differing opinions about their significance [5]. Some believed it to be a frequent incidental finding with no clinical significance [4]. Some authors claim the finding to be an uncommon lesion which is associated with malignant lesions of the female genital tract [6]. Pseudocarcinomatous hyperplasia is histologically characterized by small papillary tufts, stratification of the epithelial lining with nuclear overcrowding which is associated with loss of polarity and occasional mitotic figures. The nuclear atypia comprises of elongated and enlarged nuclei with an increased nucleocytoplasmic ratio in the hyperplastic cells. The nuclear chromatin of the hyperplastic cells is finely granular and 1-2 prominent nucleoli are commonly observed [7]. These findings were consistent in our case also and they need to be differentiated from adenocarcinoma of the fallopian tubes. The patients of tubal adenocarcinoma are mostly postmenopausal with a mean age of 62 years, whereas those with hyperplasia are younger, as has been reported in this case. Additionally, a majority of the carcinomas are grossly evident, but the pseudocarcinomatous lesions are discovered usually incidentally. A solid proliferation of the epithelial cells was not observed, although the complex pseudoglandular pattern was seen in our case. Moreover, the reactive changes which involve the fallopian tubes have been referred to as ‘hyperplasias’, which have been encountered in association with a variety of conditions, including chronic inflammation and hyperoestrogenic states [8]. There was no evidence of the involvement of the ovary by any tumour which caused a hyperoestrogenic state in our case. The other features which differentiated pseudocarcinomatous hyperplasia from adenocarcinoma were bilateral diffuse involvement of the tubes and the pseudoglandular architecture of the hyperplastic lesion which was seen microscopically with the cribriform pattern. The nuclear atypia was mild, with occasional mitotic figures.
Conclusion
We have reported a case of pseudocarcinomatous epithelial hyperplasia of the fallopian tubes, which histologically mimicked adenocarcinoma in a patient with female genital tract tuberculosis. Such cases need to be differentiated morphologically from adenocarcinoma of the fallopian tubes. A meticulous morphological assessment is required in such cases, to avoid any overtreatment of the benign condition and subsequently for the proper management of the case.
[1]. Limaiem F, Chelly I, Mekni A, Bellil S, Challenging diagnosis; florid epithelial hyperplasia versus adenocarcinoma of the fallopian tubePathology 2010 Jan42(1):99-101. [Google Scholar]
[2]. Dougherty CM, Cotten MM, Proliferative epithelial lesions of the uterine tube: I. Adenomatous hyperplasiaObstet Gynecol 1964 24:849-54. [Google Scholar]
[3]. Cheung AN, Young RH, Scully RE, Pseudocarcinomatous hyperplasia of the fallopian tube which was associated with salpingitis. A report of 14 casesAm J Surg Pathol. 1994 Nov18(11):1125-30. [Google Scholar]
[4]. Moore SW, Enterline HT, Significance of proliferative epithelial lesions of the uterine tubesObstet Gynecol 1975 45:385-90. [Google Scholar]
[5]. Yanai-Inbar I, Silverberg SG, Mucosal epithelial proliferation of the fallopian tube: prevalence, clinical associations, and optimal strategy for a histopathologic assessmentInt J Gynecol Pathol 2000 19:139-44. [Google Scholar]
[6]. Dallenbach-Hellweg G, Niehoff B, The epithelium of the tubes in correlation with the histological findings in the endometrium and the ovaryVirchows Arch A Pathol Pathol Anat 1971 354:66-79. [Google Scholar]
[7]. Alvarado-Cabrero I, Cheung A, Caduff R, Tumours of the fallopian tube. Pathology and genetics of the tumours of the breast and the female genital organs 2003 LyonIARC Press:209-10. [Google Scholar]
[8]. Pauerstein CJ, Woodruff JD, The cellular patterns in proliferative and anaplastic diseases of the fallopian tubeAm J Obstet Gynecol. 1966 96:486-92. [Google Scholar]