Primary Cerebral Nocardiosis in a Renal Transplant Recipient: A Case Report
Ragini Tilak1, Arvind Achra2, Vijai Tilak3
1 Associate Professor, Department of Microbiology, IMS, BHU, Varanasi, India
2 Junior Resident, Department of Microbiology, IMS, BHU, Varanasi, India
3 Associate Professor, Department of Pathology, IMS, BHU, Varanasi, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ragini Tilak, Associate Professor, Department of Microbiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005 India.
Phone: +91 - 9415812317,
E-mail: raginijain29@rediffmail.com
Nocardial brain abscess is a rare central nervous system infection. A 50 year old renal transplant recipient developed a nocardial cerebral abscess. It manifested clinically with pyrexia of unknown origin, recurrent episodes of convulsions and a right sided hemiparesis. The purulent material was drained and sent to the Microbiology Laboratory for culture and sensitivity studies. Direct microscopy and culture confirmed the diagnosis of nocardial infection.
Nocardiosis, Cerebral abscess, Nocardia asteroides
Introduction
Nocardia is an uncommon cause of intracranial abscesses, which comprise 1% to 2% of all the cerebral abscesses [1]. The Nocardia species are weakly gram positive, partially acid fast and filamentous branching filaments which are found worldwide in soils [2]. Nocardiosis is a relatively uncommon bacterial infection but is strongly associated with immunosuppression [3]. A majority of such infections occur in patients with a weakened cell mediated immunity, in those who have received bone marrow or solid organ transplantation and in those who are on immunosuppressive therapy. Here, we are reporting a case of a Nocardial brain abscess in a renal transplant recipient.
Case Report
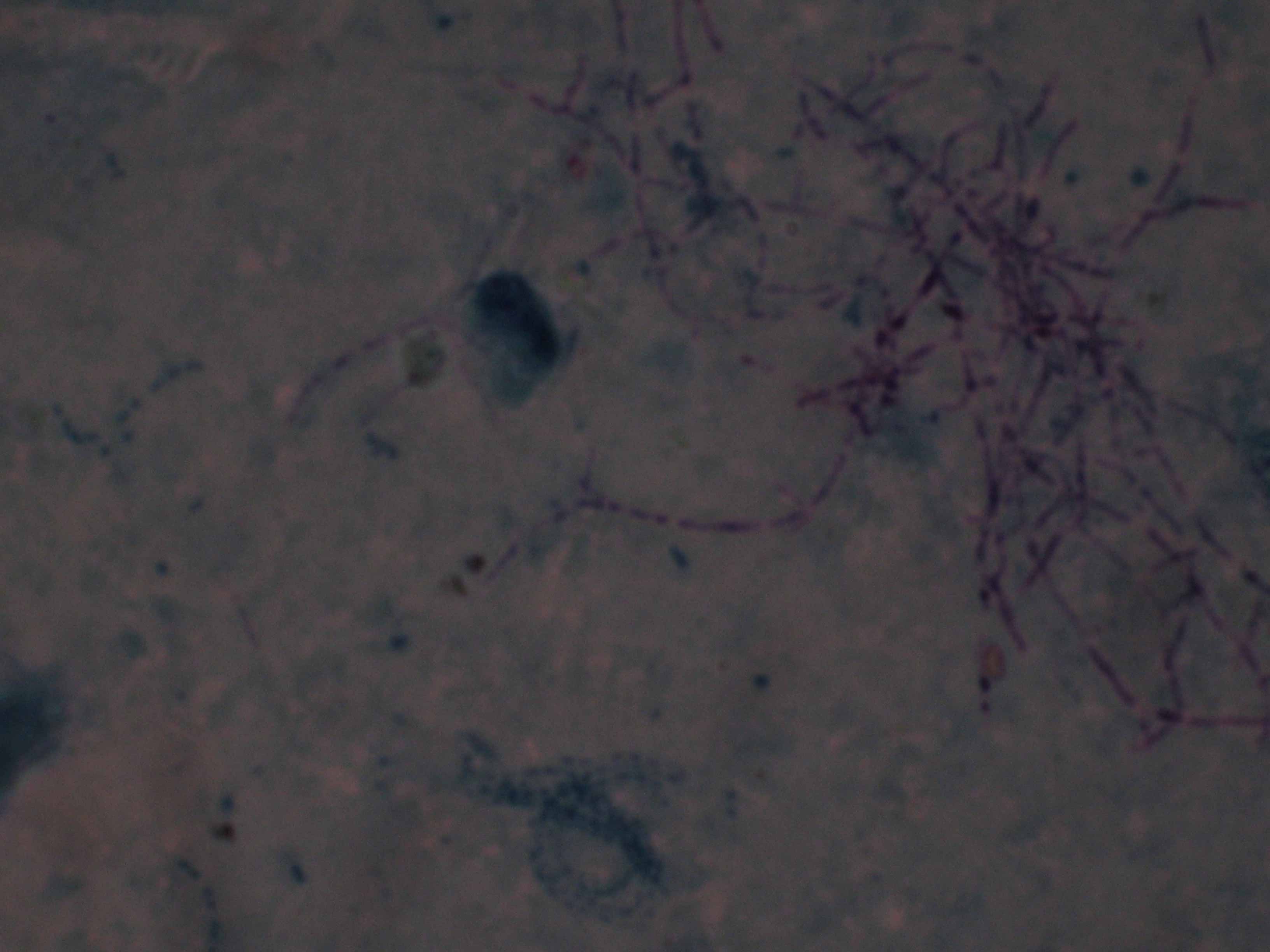
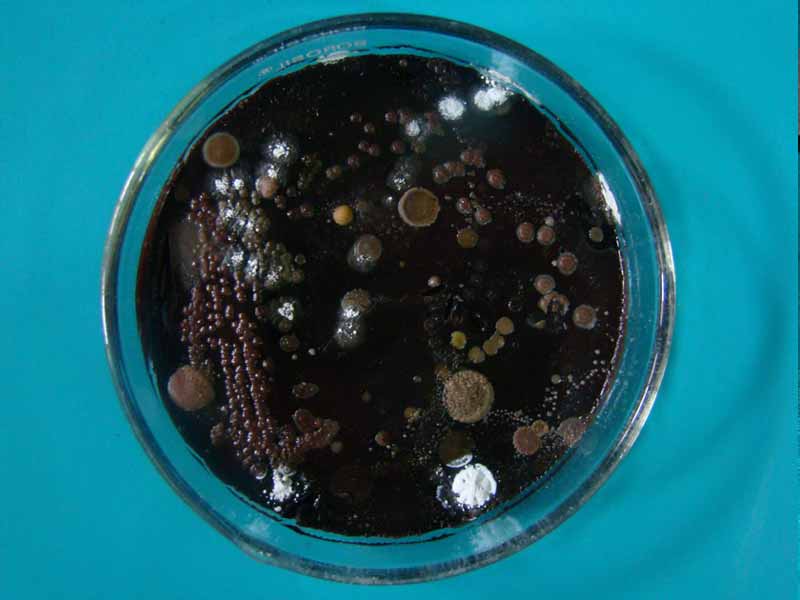
A 50-year old renal transplant recipient was admitted to our hospital, seven years post transplantation, with complaints of a throbbing generalized headache, a tonic – clonic convulsion and right sided weakness. He was on treatment (triple drug regimen) with cyclosporine, azathioprine and prednisolone. On admission, he was found to be afebrile. His laboratory investigations showed haemoglobin- 8.5gm%, TLC- 11800cells/cmm, blood urea -84mg%, creatinine -3.6mg%, SGPT- 22 IU/L, SGOT -51 IU/L, Triglycerides -148 mg/dl, HDL- 36 mg/dl, LDL- 66.4 mg/dl and VLDL- 29.6 mg/dl. His chest X-ray was normal. The computerized tomography scan of his brain showed a hypodense area in the left parietal lobe. He had no history of diabetes and hypertension. The microbiological investigation of the pus which was aspirated from the lesion showed plenty of pus cells and thin gram positive filamentous organisms. The smears of the pus which were stained with modified acid fast staining showed partially acid fast filamentous organisms [Table/Fig-1]. These findings suggested the presence of the Nocardia species. The culture of the pus showed dry, wrinkled, yellow colonies on Lowenstein Jensen’s medium, Sabouraud’s dextrose agar and blood agar [Table/Fig-2], which further confirmed the organism as N.asteroides after the biochemical tests were done for it. He was screened by collecting sputum repeatedly, for the presence of Nocardia in the respiratory tract also, but the findings were negative. The blood culture was negative. The patient was put on trimethoprim-sulphamethoxazole initially along with conventional immunosuppressives. Subsequently, he requested discharge and he was then went to SGPGI, Lucknow where his renal transplant was done.
Delicate filamentous Beading organisms with right angle branching c clearly seen on acid fast stain (oil immersion, original magnification 1000)
Blood agar showed growth of N.asteroides
Discussion
The Nocardia infection is a rare disorder which is caused by the bacteria which is called Nocardia, which tends to affect the lungs, brain, or the skin. It occurs primarily in individuals with a weakened immune system [4]. The other name of the disease is Nocardiosis. The Nocardia infection is a chronic bacterial infection that usually originates in the lungs and tends to spread to other organs, most commonly the brain and the skin. It may also involve the kidneys, the joints, the heart, the eyes, and the bones. Nocardia is found in soil all around the world. It can be acquired from the environment through inhalation or via the contamination of a wound with soil which contains Nocardia. 90% of such infections are caused by Nocardia asteroides and the remaining 10% are caused by N. brasiliensis and N .caviae [5,6]. The patients who receive steroids and/or chemotherapy are highly susceptible. There is an increased incidence of Nocardiosis in patients who suffer from bronchial asthma, malignancies or chronic pulmonary granulomatous conditions, which lead to pulmonary diseases. The subsequent haematogenous dissemination occurs from the lungs, which leads to cerebral abscess formation as well as cutaneous skin lesions [7]. Overall, the mortality rate for Nocardial abscesses (31%) is high as compared to that for other bacterial brain abscesses (10%) [8].
Our patient had the involvement of the Central Nervous System (CNS). The Nocardia species have a special tropism for the neural tissue and the most common site for their dissemination is the brain. The dissemination occurs by a haematogenous spread. The CNS infections have an indolent course. The prognosis depends on the rapidity with which the diagnosis is established. The treatment of choice is sulphonamide. In our case, a successful treatment was achieved by triple therapy with Trimethoprim Sulfamethoxazole (TMP/SMX), Ceftriaxone and Amikacin. Minocycline has been used for treating the patients with Sulphonamide Hypersensitivity [9].
Conclusion
A high index of suspicion is required to diagnose Nocardial infections, as the clinical presentation and the radiographic features mimic those of tuberculosis. An early diagnosis and a prompt treatment will improve the prognosis.
[1]. Yorke RF, Rouah E, Nocardiosis with a brain abscess which was caused by an unusual species, Nocardia transvalensisArchives of Pathology and Laboratory Medicine 2003 127(9 (2)):224-26. [Google Scholar]
[2]. Fontana I, Gasloli G, Magoni Rossi A, Bornacina C, Dodi F, Bertocchi M., Nocardiosis in a kidney-pancreas transplantJournal of Transplantation Article 2010 ID 573234,1-2, doi: 10.1155/2010/573234 [Google Scholar]
[3]. Duran E, Lopez L, Martinez A, Comuñas F, Boiron P, Rubio MC, A primary brain abscess which was caused by Nocardia otitidiscaviarum in an intravenous drug abuserJ Med Microbiol. 2001 50:101-03. [Google Scholar]
[4]. Tilak R, Agarwal D., Lahiri T.K., Tilak V., Pulmonary Nocardiosis presenting as a fungal ball-A rare entityJIDC 2008 2(2):143-45. [Google Scholar]
[5]. Talwar P, Chakrabarti A, Ayyagari A, Nayak N, Khosla VK, Minz M, Brain abscess which was caused by NocardiaMycopathologia 1989 108:21-23.doi: 10.1007/BF00436779 [Google Scholar]
[6]. Arroyo JC, Nichols S, Carrol GF, Disseminated Nocardia caviae infectionsAm J Med 1977 62:409-12. [Google Scholar]
[7]. Mamelak AN, Obana WG, Flaherty JF, Rosenblum ML, Nocardial brain abscess: the treatment strategy and the factors which influence the outcomeNeurosurgery 1994 35:622-31. [Google Scholar]
[8]. Stevens DA, Pier AC, Beaman BL, Morozumi PA, Kovett IS, Houang ET, The laboratory evaluation of an outbreak of Nocardiosis in immunocompromised hostsAm J Med 1980 71:928-34. [Google Scholar]
[9]. Sabeel A, Alrabiah F, Alfurayh O, Hassounah M, A Nocardial brain abscess in a renal transplant recipient, who was successfully treated with triple antimicrobialsClin Nephrol. 1998 Aug50(2):128-30. [Google Scholar]