Isolated Gall Bladder Perforation Following a Blunt Injury in the Abdomen
Caren D'souza1, Bhagavan K.R.2, Rakesh K.3
1 Assistant Professor, KS Hegde Medical College, Mangalore, India
2 Professor, KS Hegde Medical College, Mangalore, India
3 Post Graduate Resident, KS Hegde Medical College, Mangalore, India
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Caren D'souza, Assistant Professor, Department of General Surgery, KS Hegde Medical College, Mangalore. E-mail I D: drcaren11@gmail.com
Gall bladder injuries which are caused after a blunt trauma in the abdomen are rare and they have significant mortality and morbidity when the treatment is delayed. They usually go undiagnosed until an exploratory laparotomy is done. We are reporting here a case of isolated gall bladder neck perforation, which is an uncommon finding following a blunt injury in the abdomen.
Gall bladder, Perforation, Blunt injury abdomen
Case Report
A 27-year old man was brought to the emergency department following a road traffic accident. The patient was intoxicated, with a high dose of alcohol and heroin. On examination, his vitals were found to be normal. He had multiple bruises and minor injuries all over his body, none of which were significant. His abdominal examination revealed a bruise in the right hypochondrium. There was tenderness on palpation of the right hypochondriac region. No guarding or rigidity were seen. His biochemical and haematological profiles were normal. Ultrasonography of his abdomen revealed significant free fluid in the pericholecystic region. A Contrast Enhanced Computerized Tomography scan of the abdomen [Table/Fig-1 & 2] showed an irregularity in the gall bladder wall, with pericholecystic collection and minimal free fluid in the pelvis. The patient underwent an emergency laprotomy. Intra-operatively, bile staining of the stomach and the liver was noted. A gall bladder perforation was found near the neck of the gall bladder. No signs of liver injury or any other organ injury were seen. A cholecystectomy was done and a drain was placed in the gall bladder fossa. The post-operative period was uneventful.
CECT scan of abdomen axial cut showed irregularity in the gall bladder (white arrow)
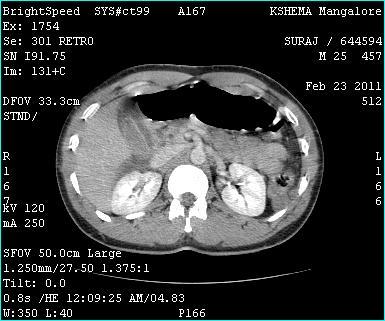
CECT scan of abdomen coronal cut showed an irregularity in the gall bladder wall with pericholecystic collection (white arrow)

Discussion
An injury to the gallbladder which results from a blunt abdominal trauma is rare; its incidence has been reported as 0.5±0.6% among all the intra-abdominal injuries [1]. The low rate of blunt trauma to the gall bladder is due to its anatomic location, which gives protection from the surrounding viscera and the ribs [2,3]. The spectrum of the injury includes contusion, perforation or rupture, laceration and avulsion [3]. Perforations are the most commonly diagnosed gall bladder injuries, accounting for 3.2% of all the injuries [2]. Gallbladder rupture following blunt trauma in the absence of other intra-abdominal injuries is extremely rare [2,4]. The mechanism of gall bladder injury in blunt trauma involves compression and shearing forces. The factors which predispose the gall bladder to perforation in blunt trauma include a thin walled normal gall bladder, gall bladder distension and alcohol ingestion, which increase the sphincter of the oddi tone and raise the biliary tract pressure [2,4].
Non-traumatic causes of gall bladder perforation can also occur due to acute cholecystitis, infections or malignancy [5,6]. The spillage of infected bile gives rise to the picture of ‘classical’ biliary peritonitis with an acute onset of toxaemia and shock, and an associated very high mortality which was variously estimated to be between 30% and 90% [4]. A delay in the presentation of the injury is not unusual. The damage to a normal, non infected gall bladder can cause the leakage of sterile bile into the abdomen. Such injures may have a delayed presentation [2,4].
The use of complementary imaging modalities such as CT, sonography and cholescentigraphy are useful for an early diagnosis of gall bladder perforation [2]. The ultrasonography findings include a complex echogenic pericholecystic collection, a thickened hypo echoic edematous gall bladder wall and disruption of the gall bladder wall with a focal loss of its reflectivity. The CT scan findings can include a pericholecystic fluid collection, gall bladder collapse, high attenuation, intra luminal density, a gall bladder wall defect, a mass effect on the duodenum and a streaky omentum or mesenteric fat [2].
The recommended treatment for gall bladder rupture and major tears is cholecystectomy. Laparoscopic cholecystectomy has been advocated to be a safe and effective procedure in the diagnosis and management of traumatic gall bladder rupture. However, in the cases in which there is an uncertainty in the diagnosis, exploratory laparotomy is the safest option [1–4].
[1]. Losanoea JE, Kjossev KT, Complete traumatic avulsion of the gallbladderInjury, Int. J. Care Injured 1999 30:365-68. [Google Scholar]
[2]. McArthur C, Unnam S, Felsenstein L, Isolated blunt traumatic gall bladder perforation which was demonstrated on MDCT and post-cholecystectomy bile leak which was revealed on Gd-EOB-DTPA (Primovist) enhanced MRCPEuropean Journal of Radiology Extra 2010 73:e65-e67. [Google Scholar]
[3]. Iwacewicz P, Wojskowicz P, Safiejko K, Barczyk J, Dadan J, Traumatic rupture of the gall ladder after a blunt abdominal traumaAdvances in Medical Sciences 2007 52:294-95. [Google Scholar]
[4]. Laffey DA, Hay DJ, Isolated perforation of the gall bladder following a blunt abdominal traumaPostgraduate Medical Journal 1979 55:212-14. [Google Scholar]
[5]. Ong CL, Wong TH, Rauff A, Acute gall bladder perforation – the dilemma in an early diagnosisGut. 1991 32(8):956-58. [Google Scholar]
[6]. Goel A, Ganguly PK, Gall bladder perforation: A case report and review of the literatureSaudi J Gastroenterol. 2004 10:155-56. [Google Scholar]