Introduction
The traditional Indian medical system known as Ayurveda includes a number of treatment approaches, including surgery. Shalya Tantra, another name for Ayurvedic surgery, has a long history and has been used for ages. But in order to guarantee the safety, effectiveness and general acceptability of Ayurvedic surgery, there has been an increasing need in recent years to create standardised approaches [1]. This article was done to examine the progress achieved in creating standardised procedures for Ayurvedic surgery, emphasising both the advantages and difficulties of this procedure.
Despite the many advantages of Ayurvedic medicine, little is known about the proper mechanisms of action, pharmacology, pharmacokinetics and pharmacovigilance of many important Ayurvedic drugs. Moreover, from a scientific perspective, a complete comprehension of Ayurveda’s core principles is unsatisfactory due to a lack of evidence [1]. Today, when the Western medical system is at the pinnacle of medical practice due to sophisticated methodologies and validated research, it is imperative to validate the basic concepts and drugs used in the Ayurvedic medical system using state-of-the-art research methods. Therefore, advancements in the existing research methodology are critical to the further development of Ayurveda. According to estimates from the World Health Organisation (WHO), between 70% and 80% of people worldwide receive their medical care from unconventional sources, mostly herbal sources [2]. The public’s interest in complementary and alternative medicine is mostly due to increased side-effects from synthetic pharmaceuticals, lack of effective treatments for many chronic illnesses, high costs associated with new drug development, microbial resistance, emerging disorders, etc., [3].
Furthermore, in this article, authors discuss the importance of audits and ethics and their utilisation in Ayurvedic practices in modern era. The rationale behind conducting a review study on ethics and audits in Ayurveda is to address the growing need for accountability, transparency and ethical standards within the field. Ayurveda, while rooted in tradition, faces increasing scrutiny in the modern healthcare landscape, where patients and regulators demand greater evidence of safety, efficacy and ethical conduct. Audits can play a pivotal role in ensuring that Ayurvedic practices adhere to ethical guidelines, safeguarding patient welfare and promoting trust. However, there is a research gap in systematically evaluating the ethical considerations of Ayurvedic treatments, particularly concerning informed consent, practitioner competence and the quality of herbal medicines. Furthermore, while audits have been widely implemented in conventional medicine, there is limited literature on how these methodologies can be adapted and implemented effectively in Ayurvedic practice. Addressing these gaps through ethical audits can help refine and regulate Ayurvedic treatments, fostering greater integration into modern healthcare systems while maintaining their traditional integrity [4].
The present study aimed to discuss the importance of audits and ethics and their utilisation in Ayurvedic practices in modern era.
Audit
“Audit” originates from the Latin word “audio,” meaning “to hear.” It refers to the procedure of the judiciary’s investigation and questioning as well as active listening. The term “audit” was first used in English to refer to “an official inspection of an organisation’s accounts, usually by an independent body.” The goal of the audit is to highlight the discrepancies between acknowledged standards and actual practice so that the necessary corrections may be made to elevate the standard of care. A unique characteristic of the clinical audit is its “professionalism,” represented by a few common elements: the object’s strong correlation with the “quality” of specialists, the participants’ clinically specific ability, and the confidentiality of the findings. From the standpoint of methodology, clinical audit consists of a “quality loop” that can restart when a topic has been chosen and discussed, quantifiable standards and criteria have been set, present clinical practice is evaluated-especially in terms of procedure or outcome-and suggestions for change are developed and put into action. The audit compares present practice to well-defined and established standards; it should not be mistaken with data-gathering operations (i.e., benchmarking) or clinical research, which really tries to determine the features of excellent practice on an unknown terrain [5].
Types of Audits
Clinical audit: A clinical audit is a structured and systematic process aimed at evaluating and improving the quality of healthcare services. It involves comparing current practices against established benchmarks or guidelines to identify gaps and areas for enhancement. The primary focus of a clinical audit is to ensure that patient care aligns with evidence-based standards, thereby promoting safety, effectiveness and consistency [6]. By collecting and analysing data on clinical outcomes and processes, audits provide actionable insights that drive improvements [7]. This iterative process typically includes selecting a specific area for review, setting clear standards, gathering and evaluating data, implementing corrective measures and reauditing to measure progress [8]. Clinical audits foster accountability, reduce variability in practices and cultivate a culture of continuous learning among healthcare professionals [9]. They are an invaluable tool for enhancing the delivery of patient-centred care across diverse medical systems, including both conventional and traditional practices like Ayurveda [10].
Surgical audit: A surgical audit is a systematic process used to evaluate and improve the quality of surgical care. It involves reviewing surgical procedures and outcomes, comparing them to established standards and identifying areas for improvement. The purpose of a surgical audit is to ensure that surgeries are performed according to best practices, to enhance patient safety and to improve overall clinical outcomes. This process typically involves collecting and analysing data on factors such as complications, recovery rates, surgical techniques and patient satisfaction. Surgical audits help identify trends, reduce errors and ensure that the healthcare team adheres to clinical guidelines. By continuously reviewing and refining surgical practices, audits contribute to better patient care and more efficient use of medical resources [11]. This technique helps to raise the standard of patient care by comparing results to established benchmarks for surgical practice. Using predetermined criteria, data is gathered, comparisons are done and suggestions for improvement are made and tracked.
A surgical audit might consist of a clinical registry with peer review, a group/hospital/specialty audit, or a personal audit (total/practice/selected). It is crucial that your audit activity covers the entirety of your scope of practice, including any seldom-performed processes, when deciding whether or not to participate in an audit [11].
Need for Audit in Ayurveda
Audits in Ayurveda are essential to maintain the quality, standardising practices, safety, patient safety and reliability of its practices and products. Regular audits are crucial to ensure Ayurvedic medicines are produced following Good Manufacturing Practices (GMP), thus preventing contamination and ensures product integrity. Audits help maintain consistency in the preparation and administration of Ayurvedic therapies, ensuring that traditional practices are preserved while meeting modern scientific standards [12]. Audits ensure adherence to both national and international guidelines, helping practitioners and manufacturers meet ethical and legal requirements. This fosters confidence among patients and users [13]. In research institutions, audits help verify that studies comply with global standards. This enables Ayurveda to gain recognition as a credible system of medicine in integrative healthcare [14]. By regularly reviewing treatment protocols, audits minimise risks and adverse effects, ensuring that Ayurvedic treatments remain safe for patients [15].
Investigation in surgical audits: An audit, in contrast to research, does not always increase the body of surgical knowledge. An audit examines surgical practice critically with the goal of raising the standard of care. The standards and limitations of research do not often apply to audits of surgical practice, as their main goal is not to further scientific inquiry; nonetheless, on occasion, they could serve as inspiration for a related research endeavour. The goal of an audit is to evaluate surgical performance in order to raise the standard of care provided by a group, hospital, or practice. Research ideas can be supported or refuted by audit databases. Thus, it makes sense to save audit data, although caution is needed [16].
The cycles of surgical audits: Depending on the kind of audit being considered, planning and preparation are necessary to guarantee its success. Speaking with important parties and thinking about doing an audit issue and the manner in which the audit will be carried out throughout a hospital, clinic, or multicentre are all crucial elements to take into account. Typically, surgical audits follow a five-step cycle [Table/Fig-1,2] [17].
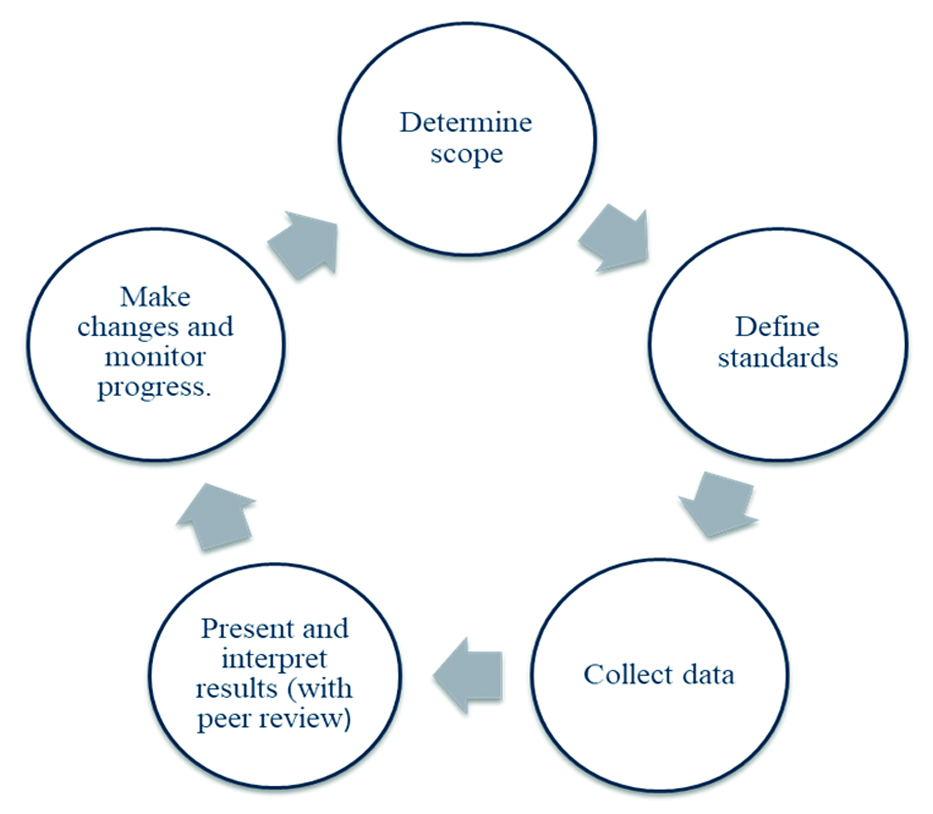
Stages of surgical audit [17].
| Stage 1 | Determine the scope [17]: | Think broadly: You may use audits to track changes, make sure that best practices are being followed, or tell your patients about the likelihood of positive and negative consequences. |
| Funding: Every audit requires resources and time. |
| Ownership: Make an effort to include everyone who could be interested in the audit’s findings. Think about include patients right now. |
| Skills: A lot of hospitals provide training programs or staff units with the knowledge and experience needed to carry out a project audit. |
| Time: Give yourself a reasonable estimate for how long the audit will take. |
| Working as a team: You can’t possibly do it all. Most initiatives require a leader. An experience of teamwork with all those concerned being actively involved is a formula that is most likely to succeed. |
| Stage 2 | Define standards [17]: | Think broadly: The auditing criteria ought to be significant. It needs to be quantifiable. The criteria have to be clear and quantifiable. |
| Verify the rules: Consult published recommendations from reliable sources if at all feasible. |
| Systematic reviews: Seek the advice of systematic reviews in fields lacking established rules. |
| Method or result: Give careful thought to the auditing criteria you have chosen. Whichever measurements you choose to use- process or outcome- will best help you achieve your goals. |
| Case mix: Regardless of the selection of criteria, a case mix modification will be necessary. While age, socio-economic status, and manner of admission are typical, co-morbidity and illness severity should be carefully considered. |
| Stage 3 | Collect data [17]: | Routine data: It’s important to confirm if your institution or any outside organisation gathers routine data in the relevant field. |
| Electronic data: Due to their simplicity of use, these data, if accessible, are worth taking into consideration. |
| Medical records: Despite their infamous incompleteness, patient registrations should nonetheless be reviewed. |
| Abstract data: Identify the information you’re looking for before visiting any data sources. Create a data abstraction tool, essentially a questionnaire, to help you identify the data that was available and the data that wasn’t. |
| Legalities: Before abstracting any data, find out what your local and national policies are regarding the project’s ethical concerns and data-related issues. |
| Stage 4 | Present and interpret results [17]: | Obstacles: Determine any potential obstacles to change before attempting to make any changes. |
| Feedback: Providing the audit participants with the results is typically not enough to bring about change on its own. |
| Talk: It is much preferable to have a conversation on ways to improve the service based on the audit results. |
| Implementation strategies: To effect change, other sectors, like the industry, employ a range of strategies. |
| Clinical governance: Using existing structures to enhance surgical care is a wise course of action. |
| Stage 5 | Make changes and monitor progress [17]: | Re-audit: Usually, it is not required to repeat the entire procedure. An occasional review along with some form of monitoring would work just well instead. |
| Ensuring that the structural change leading to better treatment is simpler for the clinician to implement than the practice it. |
| Cultural transformation: Long-term progress is hard to get unless the company actively pursues it. |
Surgical Audit in Ayurvedic Framework
A surgical audit in the Ayurveda is a systematic process of evaluating the quality and outcomes of surgical procedures performed within the Ayurvedic system of medicine. While Ayurveda is primarily known for its holistic approach to health and wellness, it also encompasses surgical interventions, known as “Shalya Tantra” [18]. Steps followed for surgical audits are described below:
Documentation: The first step involves documenting all aspects of the surgical procedure, including patient demographics, preoperative assessment, surgical technique, postoperative care, and outcomes. This documentation is crucial for later analysis.
Evaluation of surgical techniques: Ayurvedic surgical techniques, often described in ancient texts like the Sushruta Samhita, are evaluated for their efficacy, safety and adherence to traditional principles. This evaluation may involve comparing outcomes with modern surgical practices and identifying areas for improvement [18].
Assessment of outcomes: The outcomes of surgical procedures are assessed based on predefined criteria such as patient satisfaction, relief of symptoms, improvement in quality of life and complication rates. These outcomes are compared with expected benchmarks to gauge the effectiveness of the procedures.
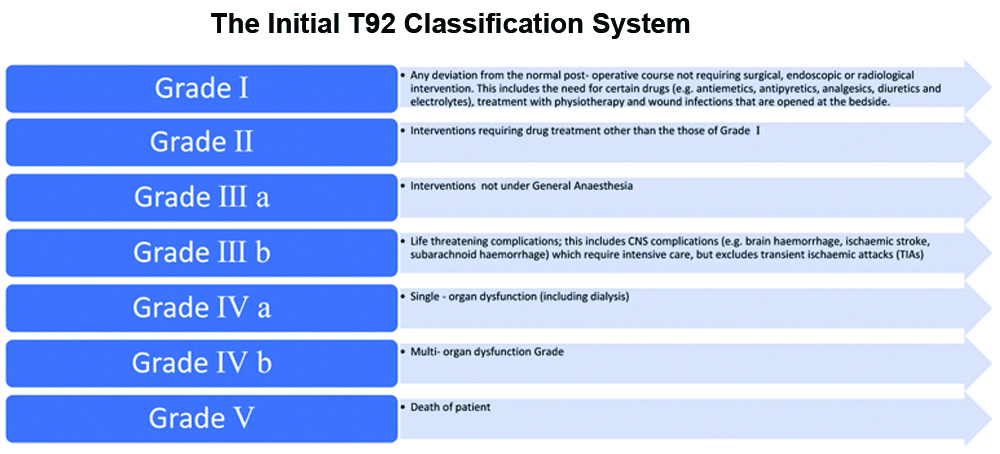
Identification of complications: Any complications arising during or after surgery are documented and analysed to determine their causes and preventability. This helps identify potential risks associated with specific surgical techniques or patient populations [Table/Fig-3] [19].
Grading of surgical complications [19].
Quality improvement: Based on the findings of the audit, quality improvement initiatives are implemented to enhance the safety and effectiveness of surgical procedures in Ayurveda. This may involve updating surgical protocols, providing additional training to practitioners, or improving infrastructure and equipment [18].
Peer review: Peer review is an essential component of surgical audit in Ayurveda, where surgical cases are reviewed by experienced practitioners to provide feedback and insights for improvement. This collaborative approach helps maintain standards and promoting continuous learning [18].
Research and innovation: Surgical audits also provide valuable data for research purposes, allowing for the development of new surgical techniques, treatment protocols and innovations in Ayurvedic surgery [18].
The Layout for the Surgical Audit
Surgical audits may take place in a variety of practice environments, such as public and private practices, which might influence the auditing practices. With the vast majority, or even all hospitals having online information systems that facilitate data collection, it should be possible for large hospitals and regional groups to conduct appropriate surgical performance audits. By doing so, they can ensure that they are meeting standards and that opportunities to improve patient outcomes will be identified. Resources to assist bigger surgical groups in doing prospective data gathering may be available in larger jurisdictions, utilising globally approved initiatives like the National Surgical Quality Improvement Programme (NSQIP) [20].
Surgical audit in remote and rural areas surgeons: Surgeons in remote areas and those who operate in small hospitals thought to define a geographic or specialised connection with more surgeons to help review. In situations where surgeons are unable to meet face-to-face or via video conference, offers a useful substitute. In regions whereby video conferences couldn’t be feasible as a result of inadequate internet access link, teleconferences need to be thought about. Additionally, it is feasible to plan an anonymous performance comparison results of surgeons in a certain area, nation, or area of expertise. But there are problems with this strategy things must be taken into account, namely variations in case mix, co-morbidity and the practice’s size and nature.
Auditing in non operational set-ups: Regardless of whether a surgeon practices surgery, being registered to practice medicine is important for participating in audits. There are audit activities that assist with quality improvement accessible for practitioners who are not operating or who are not seeing patients. These may include:
Clinical consulting practice: If surgeons are still treating patients in a clinical capacity, they ought to be participating in a clinical audit of their practice.
Report writing: Surgeons who are working as report writers may choose to have a peer review a sample of their work. Three reports must be provided annually for Continuing Professional Development (CPD) reasons, and each report must be de-identified before being submitted for evaluation. When necessary, the peer conducting the evaluation should offer specific suggestions for improvement along with helpful criticism. The Royal Australasian College of Surgeons (RACS) Medico-Legal Section may assist in facilitating a review and offers a set of criteria for evaluating a report’s quality.
Volunteer: You should carry on taking part in surgical audit and peer review in the context of your foreign volunteer activity [Table/Fig-4] [21,22].
Audit in non operative practice [22].
Role of Audit in Ayurveda [
23]
Determine strategies for enhancing and preserving the standard of patient care. Support surgeons’ ongoing education and assist in optimising resources for the delivery of surgical services. Research has demonstrated that taking part in surgical audit enhances both patient outcomes and patient care. Providing learning opportunities by promoting teamwork and changing perspectives and methods for dealing with clinical issues. Audits help in denoting knowledge and skill gaps, which prompts the creation of educational initiatives to solve problems assisting in the establishment of necessary care standards and providing direction on expectations. Surgical audits also offer chances for systemic enhancements; problems and inadequacies found in the systems ought to prompt hospital administrators to address the concerns [24].
Audit includes every surgical procedure that was carried out. Although complete practice audit is the ideal, it is acknowledged that it is not always possible. Using a complete practice audit, you may see patterns and trends in your practice by tracking changes in caseload throughput, processes completed and results. One time frame must be compared to another and must be extended sufficiently to gather a sufficient number of examples. A good general rule of thumb is to start modest and expand the audit’s scope gradually. A hospital’s quality of treatment may be measured by conducting an audit of its performance indicators, which gathers information on the process or result indicators suggested by health departments. What is the rate of wound infection, for instance, following major bowel surgery? Consider factors such as the duration of stay, antibiotic prophylaxis, emergency elective treatment and unexpected readmission rates. A large number of surgeons provide information to clinical registries, which aid in the creation of standards and variances in patient outcomes. A legitimate audit activity can be provided by a well-designed clinical registry with an outlier management procedure and a regular peer feedback loop [25].
Ethics
Ethics involve moral principles and values that guide actions, particularly in complex situations. In Ayurvedic practice, medical ethics is crucial for ensuring that treatment decisions align with core values such as respect for autonomy, beneficence, non maleficence, and justice. These principles help Ayurvedic practitioners navigate challenging cases and develop treatment plans that prioritise patient wellbeing. In situations where ethical conflicts arise, a hierarchy may be used to determine which values take precedence to guide the best course of action. Ayurvedic ethics, like in other medical fields, is especially important in decisions regarding involuntary treatments, ensuring that patient rights and health are protected while maintaining the integrity of traditional practices [26].
Ethics in Ayurveda: In Ayurveda, we refer to Bhishak, Dravya, Upasthata (attendant), and Rogi as Chatushpada. The foundation for the effectiveness of therapy is the four Gunas that each Pada has. “Upasthanam Rogi Pada Chathushtayam Bhishak Dravyani.” Bhishak occupies the highest rank among them and should possess superior theoretical knowledge, a wealth of real-world experience, dexterity, and cleanliness. Acharya Charaka is certain that anybody who wants to further their wellbeing obtains Sadvritta. In Sadvritta, Acharya teaches that it is appropriate to worship God, the Guru, the elderly, and great instructors. Acharya also suggests using flowers and fragrances, trimming hair and nails, and dressing in white. Women should not be prescribed medication without their husband or legal guardian’s consent, according to Acharya Charaka. Vaidya ought to appreciate patients who are female [27].
Ethics in Ayurvedic surgery, like in any form of medical practice, are paramount to ensure patient safety, trust, and overall wellbeing. Here are some ethical considerations specific to Ayurvedic surgery:
Qualities of surgeons:Sushruta highlights the qualities of a surgeon, including courage, rapid action, sharp surgical tools, no perspiration, no tremors, and no illusions or confusion. According to Sushruta Samhita, a quack practitioner is someone who has not individually acquired surgical skills under the tutelage of a guru (teacher) in terms of textual and practical knowledge; these persons are referred to as “Taskar-Vaidyas”. As a result, before initiating surgery, one should assess his or her own capacity to do the procedure [28].
Informed consent: Just like in modern medical practices, educated consent is crucial in Ayurvedic surgery. Patients should be provided with comprehensive information about the procedure, its risks, benefits and alternatives, enabling them to make an informed decision about their treatment [29]. To get administrative authorisation, Sushruta Samhita places equal focus on academic and practical understanding. Without actual expertise, a surgical disciple cannot conduct surgery. A surgeon cannot conduct surgery if they merely possess academic knowledge but lack practical understanding. Thus, having both theoretical and practical knowledge is necessary for an Ayurvedic Shalya Chikitsa to succeed. Once a surgeon has acquired both theoretical and practical expertise, they obtain authorisation from King’s administration. Prior to entering the medical field, a surgeon should review all related disciplines in detail. The Sushrut Samhita provides a detailed description of the rights and responsibilities of both teachers and students. The notion of student selection into the discipline of Shalya Tantra, as well as their relationship to instructor, patient, and so on, is discussed in the chapter Sisyaupaniyaadhaya of the Sushruta Samhita [30].
Preoperative/Operative/Postoperative Ethics
Three phases make up the surgical treatment of diseases comprises three phases: preoperative care (Purvakarma), surgical operation (Pradhan Karma), and postoperative care (Paschat Karma). The Sushrut Samhita highlights the significance of a clinical check-up before any surgical procedure. It is said that a surgeon should not do any procedures without first taking a complete medical history and performing a physical examination. All necessary preparations should be made before the operation, including gathering supplies like kataha (drums for hot and cold water), sitousnodaka (blunt instruments), ghrita (ghee), agni (thermal cautery), jaulaka (leeches), sutra (threads), madhu (honey), paya (milk), taila (oil), and parikarminah (attendants) who are loving, steadfast, and strong. For the treatment of Mudagarbha (obstructed labour), Udaroga (abdominal problem), Arsha (disease related to bleeding per rectum), Ashmari (urolithiasis), Bhagandar (perianal fistula), and Mukharoga (diseases of the oral cavity), Sushruta Samhita include the concept of “nil by mouth” before to surgery. Patients should be moved into a postoperative room (a special chamber) following surgery, and they should be instructed to follow the prescribed regimen (food and other activities) [31,32].
Ethics in Emergency Surgery
In emergency situations, the doctor should not adhere to protocol precisely; instead, necessary care should be administered as soon as possible, much like while rescuing a burning house. The use of lukewarm ghee heated with yastimadhuka relieves the severe agony that the knife causes the sufferers’ bodies [33].
Ethical Limitations in Practice and Referrals
Among eight branches or specialisations within Ayurveda (Ashtanga Ayurveda), it can be said that the idea of specialisation was well developed at the period, and each of these specialisations had a variety of knowledgeable practitioners. Prior to the current official legal structure, medical specialisation was recognised informally by society. The Ayurvedic literature includes a thorough description of the medical ethics that require doctors to practise within their specific areas of competence. The patient should be sent to the appropriate doctor, and one should not dabble in other specialties. It has been expressly recommended in the context of Pakva Gulma to refer the patient to the expert (surgeon) who is qualified to handle the same and in the instance of Udar-Roga Chikitsa, similarly [34].
Competence and qualifications: Ayurvedic surgeons should have the appropriate training, qualifications and experience to perform surgical procedures safely and effectively. Patients have the right to expect that their surgeon is competent and skilled in the procedures they are undergoing [35].
Respect for patient autonomy: Patients should have the right to make decisions about their own healthcare, including whether or not to undergo surgery. Ayurvedic surgeons should respect the autonomy of their patients and involve them in decision-making processes [34].
Non maleficence: This principle, commonly known as “do no harm,” is fundamental in Ayurvedic surgery. Surgeons should strive to minimise harm to patients and prioritise their wellbeing throughout the surgical process [34].
Beneficence: Ayurvedic surgeons should aim to maximise the benefits of surgery for their patients while minimising risks and harm. They should always act in the best interests of the patient’s health and wellbeing.
Confidentiality: Patient confidentiality is crucial in Ayurvedic surgery, just as it is in modern medicine. Surgeons must respect patient privacy and maintain the confidentiality of their medical information.
Integrity and honesty: Surgeons should be honest and truthful with their patients, providing accurate information about their condition, treatment options and expected outcomes. Integrity in all aspects of patient care is essential.
Cultural sensitivity: Ayurvedic surgery often involves traditional practices that are deeply rooted in cultural beliefs and customs. Surgeons should be sensitive to cultural differences and ensure that patients’ cultural beliefs and values are respected throughout the treatment process [34].
Continuing education and research: Ayurvedic surgeons should engage in ongoing education and stay updated on advancements in surgical techniques and practices. They should also contribute to research efforts aimed at improving the safety and efficacy of Ayurvedic surgical procedures.
Professionalism: Surgeons should conduct themselves with professionalism at all times, maintaining ethical standards in their interactions with patients, colleagues and the broader healthcare community.
A clinical and surgical audit in Ayurvedic practice is a quality improvement process designed to enhance patient outcomes and care by systematically evaluating Ayurvedic treatments and surgical procedures against established standards. This audit process is followed by necessary changes implemented by Ayurvedic practitioners, teams, or organisations, with a follow-up re-audit to confirm improvements in healthcare delivery. As a clinician-led initiative, it involves structured peer review where Ayurvedic practitioners assess their practices, treatments and outcomes against recognised standards, making adjustments to ensure optimal results. Ayurvedic audits ensure that best practices are applied, highlight areas where research is lacking, and guide further studies to enhance patient care. This process fosters the communication of evidence-based Ayurvedic practices, ultimately aiming to improve the quality and outcomes of care in the field [35].
Sushruta introduced the idea of highly ethical surgical practice, which is still relevant in the age of contemporary surgery. The Sushrut Samhita’s teaching and training system, which is still used in modern surgical procedures, produces highly trained individuals. The primary focus of surgery during Sushruta’s time was patient safety, a notion that is widely acknowledged in Ethical context of contemporary surgery. The exposure of surgeons to experimental surgery in models, as described in Sushruta, in order to improve the skill that is already widely accepted in surgical schools worldwide. Ayurveda places a strong focus on ethical behaviour in order to fortify the therapeutic alliance between the patient and the medical professional. The ethical principles of Ayurveda serve as benchmarks for contemporary surgeons. It is essential to recognise the ethical and professional significance of surgery and to apply the same standards of care across the board in the medical field [34].
Conclusion(s)
Standardising procedures in Ayurvedic surgery is crucial for ensuring safety, effectiveness and wider acceptance. It enhances patient care, promotes research and enables the integration of Ayurvedic surgery with modern medicine. By combining evidence-based practices, collaboration among practitioners and regulatory oversight, standardised procedures can improve outcomes. Continued research, training and strong regulatory frameworks will support the growth of Ayurvedic surgery, benefiting both patients and practitioners. Ancient Indian surgeons, guided by high ethical standards, achieved remarkable surgical skills and this legacy continues to inspire modern practices. Supporting Ayurvedic practitioners helps preserve this rich cultural heritage while advancing its role in contemporary healthcare.
[1]. Ravishankar B, Shukla VJ, Indian systems of medicine: A brief profileAfr J Tradit Complement Altern Med 2007 4(3):319-37.10.4314/ajtcam.v4i3.3122620161896PMC2816487 [Google Scholar] [CrossRef] [PubMed]
[2]. Jacqui W, Herbal products are often contaminated, study findsBMJ 2013 347:f613810.1136/bmj.f613824124179 [Google Scholar] [CrossRef]
[3]. Humber JM, The role of complementary and alternative medicine: Accommodating pluralismJAMA 2002 288(13):1655-56.10.1001/jama.288.13.165520532096PMC2876922 [Google Scholar] [CrossRef] [PubMed]
[4]. Rastogi S, Building bridges between Ayurveda and modern scienceInt J Ayurveda Res 2010 1(1):41-46.10.4103/0974-7788.59942 [Google Scholar] [CrossRef]
[5]. Abdel-Qader W, An evaluation of the international auditing standards and their application to the audit of listed corporations in Jordan [doctoral thesis] 2002 SydneyUniversity of Western Sydney [Google Scholar]
[6]. Goyal M, Srivastav S, Tiwari D, Patient safety in Ayurveda: A reviewAYU 2017 38(3):181-87.10.4103/ayu.AYU_115_1830254385PMC6153911 [Google Scholar] [CrossRef] [PubMed]
[7]. Patwardhan B, Mutalik G, Tillu G, Integrative Approaches for Health 2015 LondonAcademic Press10.1016/B978-0-12-801282-6.00012-7 [Google Scholar] [CrossRef]
[8]. Shankar D, Muralidharan S, Indian systems of medicine: A brief profileJ Ayurveda Integr Med 2010 1(1):49-56.10.4103/0975-9476.5981721829291PMC3149389 [Google Scholar] [CrossRef] [PubMed]
[9]. World Health OrganizationWHO benchmarks for training in Ayurveda 2010 GenevaWHO Press [Google Scholar]
[10]. Singh RH, The challenges of globalization and Ayurveda: Importance of clinical research and quality assurance in AyurvedaJ Ayurveda Integr Med 2010 1(2):65-66.10.4103/0974-7788.6439420814517PMC2924985 [Google Scholar] [CrossRef] [PubMed]
[11]. Pedersen AG, Petersen OB, Wara P, Rønning H, Qvist N, Laurberg S, Randomized clinical trial of laparoscopic versus open appendicectomyBr J Surg 2001 88(2):200-205.10.1046/j.1365-2168.2001.01652.x11167866 [Google Scholar] [CrossRef] [PubMed]
[12]. Ayush Ministry, Guidelines for quality control of Ayurvedic medicines 2020 New DelhiGovernment of India [Google Scholar]
[13]. Anupam S, Kanchan S, Kiran S, Mita K, Sanjeev S, Unveiling Ayurveda Aahara and regulatory provisionsJ Drug Res in Ayurvedic Sciences 2024 9(Suppl 1):S42-S47.10.4103/jdras.jdras_245_24 [Google Scholar] [CrossRef]
[14]. Hut-Mossel L, Ahaus K, Welker G, Gans R, Understanding how and why audits work in improving the quality of hospital care: A systematic realist reviewPLoS One 2021 16(3):e024867710.1371/journal.pone.024867733788894PMC8011742 [Google Scholar] [CrossRef] [PubMed]
[15]. Mishra V, Shirode P, Ayurvedic surgical advancement: Standardisation initiative and potential for enhanced healthcare resultsInt Educ Res J 2023 9(6):01-03.10.33545/26646552.2023.v5.i2a.47 [Google Scholar] [CrossRef]
[16]. Jamtvedt G, Young JM, Kristoffersen DT, Thomson O’Brien MA, Oxman AD, Audit and feedback: Effects on professional practice and health care outcomesCochrane Database Syst Rev 2000 (2):CD000259Update in: Cochrane Database Syst Rev. 2003;(3):CD000259. Doi: 10.1002/14651858.CD000259. PMID: 1079652010.1002/14651858.CD000259PMC153535 [Google Scholar] [CrossRef]
[17]. Green AJ, Smith J, Van Rij A, Watters D, Dewan P, Meade S, Surgical Audit and Peer Review: A Guide By the Royal Australasian College of Surgeons 2008 3rd edMelbourne, Victoria, AustraliaRoyal Australasian College of Surgeons:01-46. [Google Scholar]
[18]. Patwardhan K, Kumar M, Surgical practice and Ayurveda: A realistic analysis of the current debateJ Ayurveda Integr Med 2021 12(1):195-97.10.1016/j.jaim.2020.12.00833518387PMC8039338 [Google Scholar] [CrossRef] [PubMed]
[19]. Manekk R, Gharde P, Gattani R, Lamture Y, Surgical complications and its grading: A literature reviewCureus 2022 14:e2496310.7759/cureus.2496335706751PMC9187255 [Google Scholar] [CrossRef] [PubMed]
[20]. Aitken R, Nixon S, Ruckley C, Lothian Surgical Audit: A 15-year experience of improvement in surgical practice through regional computerised auditLancet 1997 350(9080):800-04.10.1016/S0140-6736(97)01021-09298014 [Google Scholar] [CrossRef] [PubMed]
[21]. Limb C, Fowler A, Gundogan B, Koshy K, Agha R, How to conduct a clinical audit and quality improvement projectInt J Surg Oncol 2017 2(6):e2410.1097/IJ9.000000000000002429177218PMC5673151 [Google Scholar] [CrossRef] [PubMed]
[22]. Lui CW, Boyle FM, Wysocki AP, Baker P, D’Souza A, Faint S, How participation in surgical mortality audit impacts surgical practiceBMC Surg 2017 17(1):42Available from: https://doi.org/10.1186/s12893-017-0240-z10.1186/s12893-017-0240-z28424055PMC5395878 [Google Scholar] [CrossRef] [PubMed]
[23]. Brown B, Bermingham S, Vermeulen M, Jennings B, Adamek K, Markou M, Surgical safety checklist audits may be misleading! Improving the implementation and adherence of the surgical safety checklist: A quality improvement projectBMJ Open Qual 2021 10(4):e00159310.1136/bmjoq-2021-00159334732540PMC8572456 [Google Scholar] [CrossRef] [PubMed]
[24]. Benjamin A, Audit: How to do it in practiceBMJ 2008 336:1241-45.10.1136/bmj.39527.628322.AD18511799PMC2405828 [Google Scholar] [CrossRef] [PubMed]
[25]. Bindroo S, Saraf R, Surgical mortality audit-lessons learned in a developing nationInt Surg 2015 100(6):1026-32.10.9738/INTSURG-D-14-00212.126414825PMC4587502 [Google Scholar] [CrossRef] [PubMed]
[26]. Gupta R, Tiwari SN, Acharya P, Shukla OP, Ethics in AyurvedaJ Ayurveda Integr Med Sci 2023 8(5):192-98.10.21760/jaims.8.6.30 [Google Scholar] [CrossRef]
[27]. Valiathan MS, Bioethics and ayurvedaIndian J Med Ethics 2007 5(1):29-30.10.20529/IJME.2008.011 [Google Scholar] [CrossRef]
[28]. Riddick F, The code of medical ethics of the American Medical AssociationOchsner J 2003 5(2):06-10.22826677PMC3399321 [Google Scholar] [PubMed]
[29]. Ambikadatta Shastri, Ayurvedatatvasandeepika Hindi commentary on Sushruta Samhita, Sutra Sthana, Chapter 4, Verse 8. 2nd ed 2012 VaranasiChaukhambha Sanskrit Sansthana [Google Scholar]
[30]. Weise M, Medical ethics made easyProf Case Manag 2016 21(2):88-94.10.1097/NCM.000000000000015126844716 [Google Scholar] [CrossRef] [PubMed]
[31]. Ambikadatta Shastri, Ayurvedatatvasandeepika Hindi commentary on Sushruta Samhita, Sutra Sthana, Chapter 7, Verse 29. 2nd ed 2012 VaranasiChaukhambha Sanskrit Sansthana [Google Scholar]
[32]. Shastri K, Chaturvedi GN, Vidyotini Hindi commentary on Charak Samhita, Part 2, Chikitsa Sthana, Chapter 13, Verses 184-190. 1st ed 2009 VaranasiChaukhambha Bharati Academy [Google Scholar]
[33]. Das B, Barman PK, Kalita D, Surgical ethics: Then and nowInt J Ayu Pharm Chem 2017 7(1):2 [Google Scholar]
[34]. Sharma SK, Singh M, Sharma SS, Surgical ethics in ayurveda–A reviewJournal of Ayurveda Physicians Surg (JAPS) 2017 Available from: https://www.semanticscholar.org/paper/SURGICAL-ETHICS-IN-AYURVEDA-%E2%80%93-A-REVIEW-Sharma-Singh/ec6572d6fcd58f7f1991769b7302965a737a78e1?utm_source=direct_link [Google Scholar]
[35]. Rose N, Pang DSJ, A practical guide to implementing clinical auditCan Vet J 2021 62(2):145-52.33542553PMC7808188 [Google Scholar] [PubMed]