Low Back Pain (LBP) represents a prevalent musculoskeletal issue on a global scale, constituting the primary cause of functional impairment and work absenteeism [1]. As of 2020, approximately 10% of the global population suffered from this condition, with projections indicating a further rise in incidence [2]. It is estimated that up to 80% of adults experience LBP at least once in their lifetime [3].
Among the potential aetiologies of LBP, herniated intervertebral discs emerge prominently, particularly among individuals aged 30-50 years. This pathology exhibits a predilection for males and correlates with factors such as heightened physical exertion, weightlifting, smoking, obesity and sedentary employment [4,5]. Disc herniation often arises from age-related degenerative processes characterised by diminished proteoglycan synthesis, leading to disc desiccation and collapse. Additionally, extrusion of disc material can result from excessive axial loading and biomechanical stress, precipitating acute symptomatic episodes, notably following strenuous physical activity. Such manifestations profoundly impede the individual’s engagement in routine activities [4,6].
Early assessment and the selection of an appropriate treatment strategy significantly influence the duration of a patient’s recovery [6]. Initial management typically entails rest, analgesia, physical therapy and potentially epidural steroid injections. Urgent surgical consideration arises in cases of progressive neurological deficits, bowel or bladder dysfunction, and/or saddle block anaesthesia. While approximately 90% of patients experience symptom resolution with conservative measures, persistent symptoms following exhaustive conservative therapy prompt consideration of lumbar discectomy [7-10].
Quantitative assessment of herniation size through Magnetic Resonance Imaging (MRI) plays a crucial role in deciding between conservative and surgical interventions [9]. Clinical data suggest that patients with disc herniations exceeding 6 mm in size achieve superior postoperative outcomes, establishing this metric as indicative of surgical necessity [9]. The hypothesis associating preoperative herniation size with surgical efficacy is supported by research from En’Wezoh DC et al., which simultaneously disproved the existence of a precise threshold determining the suitability of a patient for conventional or operative treatment [10]. Regardless of the existence of a precise threshold, MRI measurements are widely considered the most objective means of assessing the severity of LDH, enabling the prediction of treatment success in symptomatic patients [9,10]. However, due to the expense and technical complexity associated with MRI scans, this diagnostic tool is typically reserved for patients who do not respond to conventional treatments or exhibit symptoms suggestive of the need for surgery. Consequently, many studies examining the effectiveness of non invasive therapeutic approaches do not include MRI assessments, relying instead on subjective symptom evaluation [11-15].
An increasingly popular non surgical alternative to surgery is spinal decompression therapy. This treatment operates on the principle of delivering targeted decompression force to the affected spinal segment using a sophisticated positioning and motion system integrated into the treatment couch. The mechanism is controlled through a computerised algorithm that applies the accurate decompression load to the specified segment. Non invasive spinal decompression therapy can be administered alone or in conjunction with other physical therapy modalities, providing complementary effects such as tension release, improved circulation and pain reduction [12,16].
The existing clinical evidence focusing on the relatively recently developed NSSD approach promises satisfactory results for herniations at various spine levels in patients of different age groups [13-15]. However, when assessing improvements in herniation, only two studies utilised quantitative MRI measurements, specifically focusing on parameters such as the Herniation Index (HI), disc height and herniation thickness [17,18]. These studies primarily included patients with mild to moderate herniation and did not evaluate indicators such as disc area, canal area, or canal length. The threshold of 6 mm for disc herniation was selected based on existing clinical evidence, as herniations of this size are often considered indicators for successful outcomes through invasive procedures. However, from a non invasive treatment standpoint, such cases pose a significant therapeutic challenge, and studies documenting the efficacy of NSSD in herniations of this magnitude remain limited.
The present study was aimed to quantitatively assess the improvement of lumbar herniation using MRI in patients with herniation exceeding 6 mm after completing an intensive treatment regimen consisting of a combination of non invasive therapeutic methods, including NSSD, HIL, and RPMS.
Materials and Methods
A retrospective quasi-experimental study was conducted in Biosalus Private Clinic, Surdo di Rende, Italy, from November 2022 to September 2024. The study adhered to ethical guidelines outlined in the 1975 Declaration of Helsinki, as adopted by the Convention on Human Rights and Biomedicine of the Council of Europe (1997) and endorsed by the General Assembly of the World Medical Association (1997-2000) [19]. The research was approved by the local ethics committee, Comitato Etico Regione Calabria (11125 DEL 01/08/2023), under registration number 251/2024. Eight patients were provided with detailed information about the treatment program’s potential risks, and any queries were addressed. Patients confirmed their willingness to participate and agreed to the publication of the results by signing a written consent form.
Inclusion criteria: Individuals experiencing painful and debilitating symptoms attributed to LDH, as confirmed by functional assessments such as the Femoral Nerve Tension Test (FNTT) [20], Straight Leg Raising Test (SLRT) [21], evaluation of the ability to walk on tiptoes and heels, the Muscle Research Council (MRC) scale for muscle strength [22], and pain measurement using the Visual Analog Scale (VAS) [23]. Based on existing evidence, the majority of patients with LDH symptoms experience spontaneous recovery within the first 6-12 weeks of initiating conservative treatment [24]. To reduce the potential influence of spontaneous recovery on study outcomes, a criterion was added to the inclusion requirements: only patients who had not responded to prior conservative treatment were eligible for participation in the study, and the program began at least one month after the completion and three months after the initiation of their previous conventional treatment. Another condition was confirmed disc herniation at the L4-L5 level by MRI scan with an AP length greater than 6 mm and consent to participate in the intensive non invasive program and associated evaluations.
Exclusion criteria: Those with contraindications for NSSD, such as malignant bone tumours, fractures, joint inflammation, spastic paralysis, osteoporosis, meningeal signs, hernia, pregnancy, cardiac and pulmonary insufficiency, haemorrhagic conditions, infectious diseases, claustrophobia, and any condition for which movement is contraindicated were excluded from the study. Similarly, patients who had contraindications for HIL or RPMS were excluded.
Study Procedure
All participants underwent a 3-month treatment protocol involving a combination of NSSD, HIL and RPMS therapy. MRI scans were performed at baseline and immediately following the completion of treatment. Key parameters obtained by analysis of MRI images included the herniation AP length, herniation area, canal AP length, canal area and the HI [8,17]. Patients were further monitored using functional tests to detect symptom recurrence for three months post-treatment. During the first month, treatment sessions were administered five times per week; during the second and third months, the frequency was reduced to three and two times per week, respectively. In total, patients completed an intensive treatment program comprising 40 combined sessions.
NSSD therapy (BTL Spinal Decompression, Model Premium, BTL Industries Ltd.) was performed with the patient in a supine position on a therapeutic couch equipped with movable parts for optimal positioning [Table/Fig-1]. The computerised control unit ensured precise delivery of decompression force, never exceeding 50% of the patient’s body weight, specifically targeted to the affected spinal segment. The therapy session lasted 30 minutes, followed by a stabilisation period during which the patient remained still and relaxed [13,14].
Patient position during therapy with NSSD in order to reduce the extent of disc herniation at the lumbar level.

Following NSSD therapy, HIL (BTL Industries Ltd.) and RPMS (BTL Industries Ltd.) were administered. The treatment plan for each patient was individualised, taking into consideration their specific condition and symptoms. During the final month of therapy, additional therapeutic exercises were introduced to reinforce the progress made. These included proprioceptive exercises to enhance balance and body awareness, ambulatory step activities to improve gait, Re-education Global Postural (RPG) for correcting posture, diaphragmatic rehabilitation for improving breathing mechanics, and core stability exercises to strengthen the deep muscles of the torso, all aimed at sustaining the treatment outcomes.
To ensure an accurate comparison of the MRI results with existing clinical evidence, multiple measurement methods were employed (MicroDicom DICOM Viewer 2023.3 x86). Transverse T2-weighted MRI images of the L4-L5 region were analysed. The herniation AP length, determined by the maximum AP length of the disc herniation, was selected as the primary indicator of herniation size. Additionally, the herniation area was measured, along with indicators of changes in the area and length of the spinal canal. Canal AP length, in this context, refers to the distance from the lowest point of the disc to the lowest point of the canal. Several other measurements were taken to calculate the HI using the formula [17]:
Where:
HL=Herniation AP length as described above,
HW=Herniation width determined as the width of the disc at the level of half of the HL distance,
TCL=Total canal length determined as the maximal AP canal length,
TCW=Total canal width determined as the width of the canal at the level of half of the HL distance.
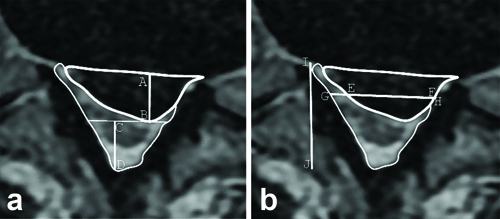
All the quantitative changes in the MRI images and the measurements utilised for calculating the HI are depicted in [Table/Fig-2a,b], respectively. The transverse MRI images were additionally categorised using the Michigan State University (MSU) classification system, which considers both the size and location of the disc herniation [25].
a) Visualisation of quantitative indicators of disc herniation from an MRI image. Herniation AP length (AB), herniation area (the upper area bounded by a thick line), canal AP length (CD) and canal area (the bottom area); b) Display of measurements determining HI calculation. Herniation width (EF), total canal width (GH) and total canal length (IJ).
All MRI images included in the study underwent evaluation by an impartial neuroradiologist, who assessed the images as part of routine clinical practice and was unaware of the study’s specifics. Patients were monitored for up to three months following the completion of the treatment program through a series of functional tests.
Statistical Analysis
Statistical analysis was conducted using the Matlab environment (MatLab R2010b, Mathworks, Inc., Natick, MA, USA) with a custom script. Given the normal distribution of the data, as determined by the Shapiro-Wilk test, the statistical significance of the observed changes in the measured values derived from the MRI image analysis was assessed using a paired t-test. A p-value of <0.05 was considered statistically significant.
Results
Eight patients with LDH exceeding 6 mm, as confirmed by MRI examination, were enrolled in the study. A summary of the demographic and other characteristics of the study participants has been provided in [Table/Fig-3]. All patients completed the treatment program without reporting any adverse events or discomfort during treatment. Quantitative measures of disc herniation were obtained by analysing MRI images taken before the initiation and after the completion of the treatment program [Table/Fig-4]. According to the MSU classification, all herniations observed before the study fell within the range of grades 2 to 3, with locations predominantly categorised as B or AB. Throughout the treatment program, all patients exhibited improvement, as evidenced by the final MRI classification according to the MSU, which ranged from grades 1 to 2, mostly in locations A or B. This improvement was further substantiated quantitatively by various indicators, with notable significance observed in terms of the HI and herniation AP length. Importantly, changes in all monitored parameters achieved statistical significance during the treatment program, with p-values <0.05. Besides quantitative analysis, MRI images underwent evaluation by an impartial neuroradiologist. The summarised text of the evaluation report is provided in [Table/Fig-5].
Patients’ characteristics, regarding demographics, onset and manifestations of symptoms.
| Patient No. | Gender | Age | Occupation | Symptoms | Duration of symptoms |
|---|
| 1 | Male | 49 | Engineer | Functional impairment in the left leg challenges in maintaining an upright posture | 7 months |
| 2 | Female | 50 | Employee | Functional deficit in the right leg, which is accompanied by difficulty walking and a sensation of paresthesia in the L5 root area | 4 months |
| 3 | Male | 49 | Sales agent | An inability to walk and drive due to a loss of sensation in the left foot | 5 months |
| 4 | Female | 54 | Bank clerk | Functional deficit in the right leg, which is accompanied by difficulty walking and a sensation of paresthesia in the l4-l5 root area | 5 months |
| 5 | Male | 50 | Driver | Pain and lumbar functional limitations | 15 months |
| 6 | Female | 46 | Housewife | Pain and lumbar functional limitations | 12 months |
| 7 | Male | 57 | Bank clerk | Pain and lumbar functional limitations | 4 months |
| 8 | Female | 33 | Housewife | Pain and lumbar functional limitations | 4 months |
Indicators derived from quantitative analysis of MRI images obtained before and after the treatment program were assessed. A statistical comparison of the changes in these measures was conducted using a paired t-test, with p-values <0.05 deemed statistically significant.
| Patient No. | MRI images | MSU* | Herniation AP length (mm) | Herniation area (mm2) | Canal AP length (mm) | Canal area
(mm2) | HI |
|---|
| 1 | Before | 3AB | 9.35 | 149.7 | 8.8 | 121.97 | 373.50 |
| After | 1A | 2.58 | 48.58 | 14.87 | 224.51 | 98.23 |
| 2 | Before | 3AB | 8.39 | 85.4 | 9.42 | 109.74 | 339.22 |
| After | 2A | 3.26 | 33.61 | 14.99 | 162.25 | 82.93 |
| 3 | Before | 3AB | 8.52 | 114.27 | 9.07 | 154.49 | 370.99 |
| After | 2A | 3.45 | 56.81 | 12.01 | 219.41 | 83.32 |
| 4 | Before | 2B | 6.03 | 57.60 | 12.25 | 116.46 | 228.11 |
| After | 1B | 1.99 | 31.21 | 16.22 | 142.78 | 62.32 |
| 5 | Before | 2B | 7.20 | 92.33 | 10.44 | 208.08 | 182.30 |
| After | 1A | 1.49 | 25.83 | 16.35 | 275.37 | 59.23 |
| 6 | Before | 3AB | 7.38 | 68.84 | 10.95 | 135.02 | 298.86 |
| After | 1B | 1.97 | 27.94 | 17.29 | 184.67 | 66.92 |
| 7 | Before | 3AB | 8.66 | 98.00 | 9.27 | 145.74 | 223.31 |
| After | 2AB | 4.23 | 53.81 | 13.98 | 188.67 | 76.65 |
| 8 | Before | 3A | 11.13 | 186.74 | 4.87 | 66.16 | 455.96 |
| After | 2A | 3.97 | 95.58 | 12.32 | 158.32 | 140.99 |
| Comparison | Before | Mean±SD | 8.33±1.54 | 106.61±42.92 | 9.38±2.16 | 132.21±40.82 | 309.03±93.01 |
| After | Mean±SD | 2.87±1.01 | 46.67±23.13 | 14.75±1.90 | 194.50±43.45 | 83.82±26.41 |
| Improvement* | Mean±SD (%) | 66.02±8.96 | 56.20±10.21 | 63.90±38.22 | 54.30±39.12 | 72.42±4.56 |
| p-value (<0.05) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
MSU: Michigan state university classification system; AP: Anterioposterior; HI: Herniation index; *The average percentage improvements were calculated by taking the percentage improvement for each individual patient and averaging these values across all participants
Assessment of MRI images obtained prior to the initiation of an intensive non invasive treatment program (pretreatment) and following its completion (post-treatment).
| Patient No. | MRI evaluation by a neuroradiologist |
|---|
| Before | After |
|---|
| 1 | At the L4-L5 level, there is a prominent disc herniation protruding into the left median-paramedian region, leading to compression and impingement on the emerging nerve roots. | The herniation seems to have notably reduced in size compared to a previous diagnostic assessment. |
| 2 | At the L4-L5 level, there is a disc herniation protruding into the right median-paramedian area, exerting pressure on the ventral surface of the dural sac and resulting in compression and impingement on the emerging nerve roots. | The identified herniation appears smaller compared to the previously noted examination. |
| 3 | At the L4-L5 level, there is a posteriorly protruding disc herniation located in the left median/paramedian region. This herniation causes a reduction in the width of the vertebral canal and blocks the ipsilateral intervertebral foramen. | There is a median disc herniation at the L4/L5 level, and the spinal canal has a regular width. |
| 4 | At the L4-L5 level, there is a herniated posteriorlateral disc on the right-side, with a fragment protruding and situated superiorly behind the body of L4 at the right anterolateral epidural location. This lesion creates an indentation on the contour of the dural sac. | The previously expelled fragment, positioned superiorly behind the body of L4 at the right anterolateral epidural site, is no longer observable at the L4-L5 level. However, there remains a residual modest elevation of herniation on the postero-lateral right-side, at the level of the disc plane. |
| 5 | There is a left median-paramedian herniation with the disc extending into the intervertebral foramen at the L4-L5 level. In the left lateral recess of L5, there is isointense tissue to the disc present in close proximity to the cauda equina nerve roots, at the extramedullary intradural site. | There is a notable decrease in the size of the left-sided median and paramedian herniation at the L4-L5 level. The signal intensity of the cauda equina appears normal. |
| 6 | At the L4-L5 level, there is a prominent herniated disc protruding into the left lateral region, causing obliteration of the corresponding foraminal recess and resulting in compression of the L5 nerve root on this side. | At the L4-L5 level, there is disc bulging with involvement of both foraminal regions, particularly notable on the right-side. Additionally, there is a left paramedian-preforaminal herniated disc posteriorly. |
| 7 | At the L4-L5 level, there is a conspicuous right lateral-foraminal disc herniation, which is pressing on the dural sac. | At the L4-L5:level, there is a median and right paramedian disc herniation. Spinal canal maintains a regular amplitude, indicating no significant narrowing or compression. |
| 8 | At the L4-L5 level, a significant amount of disc tissue appears to be extruded and displaced towards the lower right-side. This displacement reduces the amplitude of the lateral recess and extends into the foraminal space, leading to compression of the corresponding nerve root. | At the L4-L5 level, there is a modest right paramedian and posteromedian disc herniation that indents the ventral surface of the dural sac. |
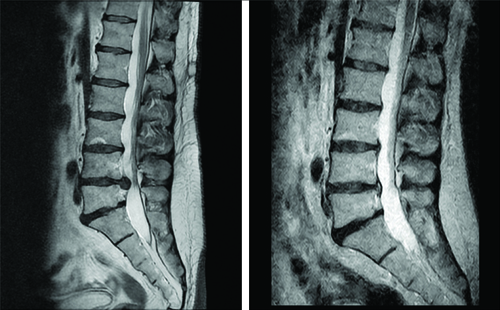
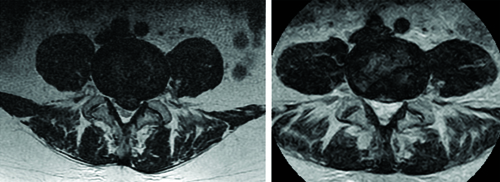
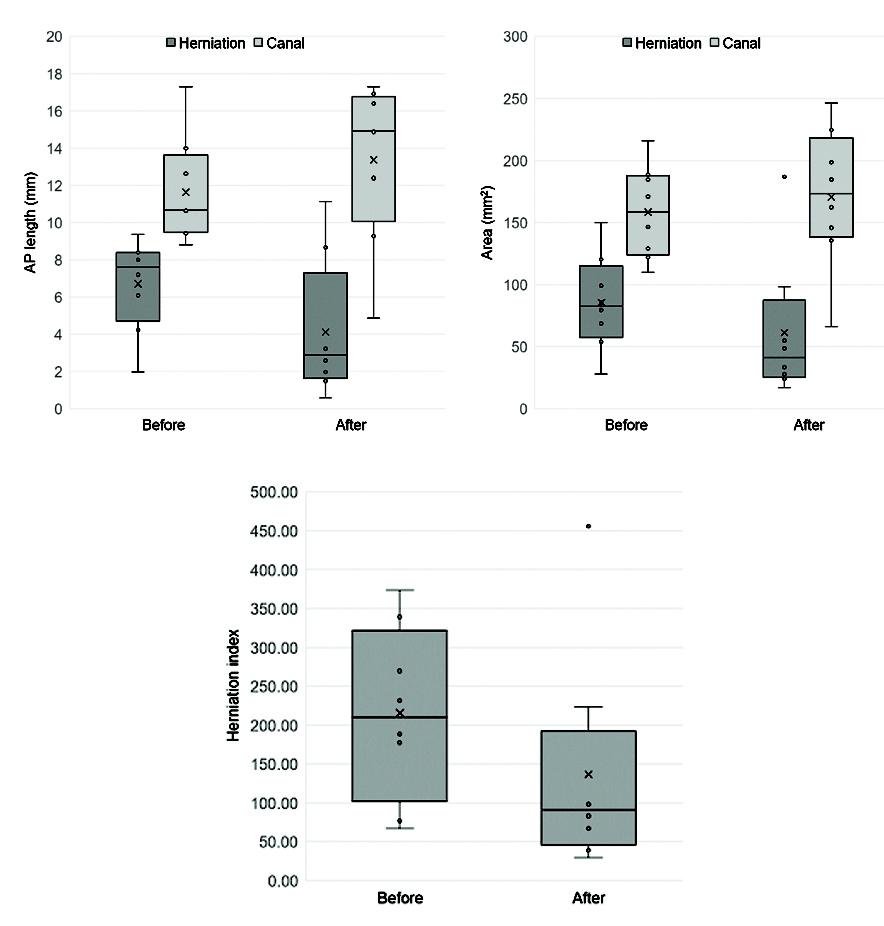
To provide a comprehensive understanding of the changes attained during the treatment program, MRI images of patient one are depicted in both [Table/Fig-6,7]. The improvement achieved is evident from both sagittal and transverse plane images. However, for the sake of quantitative evaluation, only the transverse images were processed. The obtained quantitative data are illustrated through box plot graphs in [Table/Fig-8]. These graphs depict the changes resulting from the treatment, showing a decrease in the AP length and area of the herniation, alongside an increase in the canal indicators. Of particular significance is the observed change in the HI parameter, which provides a comprehensive assessment of the achieved improvements.
Example illustrating the comparison of a sagittal T2-weighted MRI image obtained during the initial visit (left) with that acquired after the completion of the treatment program (right).
An illustration demonstrating the comparison between a transverse T2-weighted MRI image obtained during the initial visit (on the left) and one acquired after the completion of the treatment program (on the right).
Box plot graphs depicting changes based on quantitative indicators from MRI images captured before the initiation of the treatment program (before) and upon its conclusion (after) are presented. Data set’s distribution is visualised by showing the minimum, first quartile, median, third quartile, and maximum values. The graphs illustrate a comparison of herniation and canal AP length (upper left), herniation and canal area (upper right), and HI (bottom left).
All patients underwent continuous monitoring using functional assessment methods for up to three months following the completion of the treatment program. In seven patients, herniation symptoms, evaluated through the FNTT, SLRT, and the ability to walk on tiptoes and heels had completely resolved. These patients also reported a final VAS pain score of 0 and achieved an MRC strength grade of 5. One patient (no. 8) exhibited minor residual signs of herniation but experienced significant improvement in symptoms and functional capacity. Despite these remaining signs, his condition showed marked progress compared to the initial presentation.
Discussion
The current study underscores the potential efficacy of an intensive non invasive treatment protocol comprising NSSD therapy supplemented with HIL and RPMS for the management of LDH exceeding 6 mm in patients with chronic manifestations. This investigation diverges from the prevailing trend in existing clinical evidence, not only by employing quantitative MRI evaluation methods but also by focusing on patients who are typically candidates for surgery within standard medical practice. In cases where sciatica symptoms persist despite undergoing conventional therapy, and these symptoms are attributed to a large-scale disc herniation as diagnosed by MRI, surgery is generally recommended as a final treatment option [8,9].
Demirel A et al., in their study comparing the efficacy of conventional physiotherapy methods alone versus in combination with NSSD, did not observe a statistically significant difference in improvement between the two groups [18]. Notably, the improvement in terms of herniation thickness averaged 1.7 mm, significantly less than the 5.46 mm reduction achieved in the present study. This variance may be attributed to several factors. Firstly, Demirel A et al.’s study predominantly included patients with small to moderate disc herniation, typically not exceeding 6 mm in length. Consequently, comparable improvements may not be anticipated in comparison to patients with large-scale herniation reaching nearly 8 mm in AP length [18].
Therapeutically, the main disparity between the results of the two studies lies in the divergent intensity of their treatment protocols. While the current study employed an intensive 3-month treatment regimen comprising 40 combined NSSD, RPMS, and HIL sessions, Demirel A et al., opted for a shorter program consisting of 15 sessions of conventional physiotherapy, 10 NSSD sessions, and five sessions of stabilisation exercises [18]. Furthermore, it is noteworthy that in the present study, final MRI images were acquired immediately after the completion of the treatment program, whereas Demirel A et al., evaluated images taken after a 3-month follow-up period [18].
Similarly, when comparing the present study with the research conducted by Choi E et al., which examined changes in the HI following ten sessions of NSSD over an eight-week period, notable differences arise [17]. Specifically, the average reduction of 27% observed by Choi E et al., is substantially lower than the improvement demonstrated in the current study, which reached 72%. This variance can be attributed to several factors, primarily the disparity in treatment protocol intensity and the evaluation of progress solely after a 3-month follow-up period, which may elucidate this difference [17].
The findings of the present study hold promise for individuals grappling with symptoms stemming from large-scale LDH, particularly those who have experienced unsuccessful outcomes with conventional treatment methods and are hesitant to undergo invasive surgical procedures for various reasons. Through an intensive treatment program incorporating NSSD, HIL and RPMS therapy, patients achieved significant improvement to the extent that surgical intervention was no longer deemed necessary. It is important to note that due to the rigorous and time-intensive nature of the protocol, this non invasive approach may not be suitable for all individuals. However, it holds potential as an alternative for those unwilling or unable to pursue invasive interventions in the future.
An intriguing aspect of the present research is that most participants (7 out of 8) exhibited herniation in segments AB or B according to the MSU classification, regions typically associated with poor responsiveness to medical therapy [25]. Nonetheless, the application of an intensive treatment protocol proved effective for all patients in the present study.
In the current study, anatomical changes were evaluated immediately upon the completion of the treatment program, while functional tests tracking the manifestation of LDH symptoms were conducted three months after the program concluded. However, functional outcomes do not necessarily reflect underlying structural changes. Although symptom relief and functional improvements are crucial from the patient’s perspective, particularly in terms of disability, the research emphasis suggests the need for further imaging. Future studies should aim to include follow-up MRI scans, ideally six months post-treatment, to provide a more comprehensive understanding of structural recovery.
In the future, it would also be advantageous to explore the impact of various demographic and clinical factors, including age, BMI, duration of symptoms, level of herniation, etc., on the efficacy of this intensive non invasive protocol. Concurrently, assessing its time and financial requirements, as well as recovery duration, and juxtaposing them with those of invasive procedures could provide valuable insights. Such investigations could yield a decision-making framework for patients who are uncertain about which treatment strategy to pursue.
Limitation(s)
The primary limitations of the present study include the relatively small sample size, the lack of a control group and the absence of adequate follow-up with repeat MRI imaging for further evaluation. Additionally, it is important to acknowledge that the research was conducted at a single centre, which limits the generalisability of the findings to broader populations. Due to the financial constraints associated with MRI examinations and the demanding nature of the intensive treatment protocol, only the minimum requisite number of patients was included in the present study to detect statistical significance with reasonable power. The impact of spontaneous recovery, which typically manifests in the initial weeks following symptom onset and the initiation of conventional treatment, was partially addressed by the inclusion criteria specifying only patients with chronic symptoms persisting for at least three months after commencing and one month after concluding conventional treatment. However, it is advisable to incorporate a control group of patients into the research and substantially enlarge the patient cohort. In addition to enhancing the credibility and statistical robustness of the study, a larger sample size would likely facilitate the inclusion of patients from other age groups. The current study predominantly focuses on a narrow age range of 46-57 years. To corroborate the efficacy of the protocol employed, further research on a larger scale with the inclusion of a control group is essential. Ideally, studies of this nature should incorporate long-term follow-up assessments to monitor the progression of the condition beyond the immediate post-treatment phase.
Conclusion(s)
The current study outlined the potential of an intensive non invasive protocol comprising NSSD, HIL and RPMS in alleviating symptoms of large-scale LDH in patients with chronic manifestations unresponsive to conventional treatments. The substantial improvement observed, as assessed through quantitative analysis of MRI images, enabled patients to forego the necessity of surgery, which had been recommended for half of them. These findings offer a potential solution not only for patients who, for various reasons, are hesitant or unable to pursue surgical intervention and seek non invasive alternatives but also for physiotherapists who advocate non invasive approaches in managing LDH symptoms.
MSU: Michigan state university classification system; AP: Anterioposterior; HI: Herniation index; *The average percentage improvements were calculated by taking the percentage improvement for each individual patient and averaging these values across all participants