Management of Concurrent Talar Body and Bimalleolar Fractures in Sagittal Plane: A Case Report
Rohit Varma Kothapalli1, Vijayanand Balasubramanian2, RS Palanisami3
1 Postgraduate, Department of Orthopaedics, SRM Medical College Hospital and Research Institute, Chennai, Tamil Nadu, India.
2 Professor and Head, Department of Orthopaedics, SRM Medical College Hospital and Research Institute, Chennai, Tamil Nadu, India.
3 Assistant Professor, Department of Orthopaedics, SRM Medical College Hospital and Research Institute, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Rohit Varma Kothapalli, A505, SIS Marakesh, Karnaipuduchery Road, Urapakkam, Chennai-603202, Tamil Nadu, India.
E-mail: rk5026@srmist.edu.in
Talar fractures are relatively uncommon, with an incidence of 0.1% to 0.85% of all fractures and 3% to 6% of all foot fractures. Among these, talar neck fractures are more common than those of the talar body, typically occurring in the coronal plane. Restoration of joint congruency is necessary to reduce the incidence of osteonecrosis and post-traumatic osteoarthritis. Most fractures occur in the talar neck or body in the coronal plane. In the present case report, authors present a sagittal plane fracture of the talar body in combination with a bimalleolar fracture in a 45-year-old female, managed with open reduction and internal fixation using screws. In the present case, the dual approach, which is ideal, could not be performed due to the condition of the wound over the lateral aspect of the ankle. Proper planning regarding the timing of surgery, considering the swelling and soft tissue status, alongside proper anatomic reduction and rigid fixation with good surgical technique and postoperative rehabilitation, are key to achieving favourable clinical outcomes.
Osteonecrosis, Post-traumatic osteoarthritis, Talus fracture, Vertical fracture
Case Report
A 45-year-old female presented to the Emergency Department four hours following a road traffic accident, with a grossly swollen right ankle and foot, along with an inability to bear weight. Minor abrasions were noted over the lateral malleolus [Table/Fig-1]. The swelling was sudden in onset, firm in consistency and diffusely present around the medial and lateral malleoli, extending to the anterior aspect of the ankle joint and the dorsum of the midfoot. The distal neurovascular status was intact.
Clinical picture of patient’s ankle with abrasions over the lateral aspect.

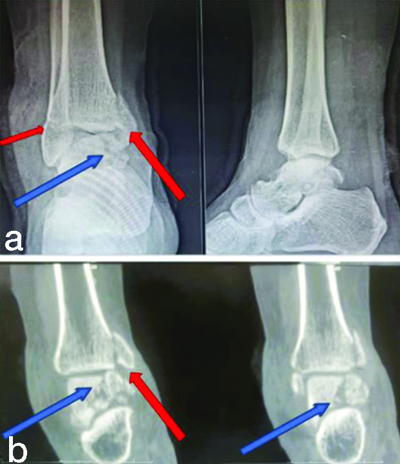
Radiographs revealed a displaced vertical fracture of the body of the talus, a vertical fracture of the medial malleolus and a transverse fracture of the lateral malleolus [Table/Fig-2]. There was no past medical or surgical history, nor any previous surgeries. A preanaesthetic evaluation was conducted and fitness was given as American Society of Anaesthesiologists (ASA) grade 1. The patient was planned for open surgical fixation of the ankle.
a) Anteroposterior (AP) and lateral radiographs of ankle; and b) Computed tomography coronal section of ankle showing fracture pattern. {Blue arrow showing talus fracture, Red arrow showing medial (large) and lateral (small) malleolus}.
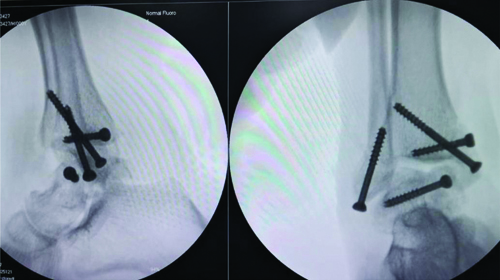
With the patient in the supine position, a medial approach was utilised along the medial malleolar fracture line to expose the talar fracture. The deltoid ligament was protected along with the medial malleolar fragment. The minimally comminuted talar fracture was reduced and fixed with Arbeitsgemeinschaft für Osteosynthesefragen (AO) cancellous lag screws under fluoroscopic guidance. The reduction was optimal due to minimal resorption of the comminuted ends. The medial and lateral malleoli were also fixed with cancellous screws [Table/Fig-3,4].
Intraoperative C-arm picture of fracture fixation.
Immediate postoperative radiograph of right ankle AP and lateral.

Postoperatively, the patient was advised against weight-bearing for six weeks [Table/Fig-5], progressing to full weight-bearing by 12 weeks. At the end of one year, there was a terminal limitation of ankle movements.
Postoperative radiograph of right ankle AP and lateral at six weeks postoperative.

Discussion
Talar body fractures are uncommon, accounting for less than 25% of all talus fractures [1]. Unlike talar neck fractures, the fracture line in talar body fractures extends into the articular surfaces of both the ankle and subtalar joints, leading to an increased risk of arthritis in both of these joints [2].
Inokuchi S et al., further classified vertical fractures into two groups based on the fracture angle in relation to the longitudinal axis of the talar trochlea. They categorised fractures with angles of less than 45 degrees to the talar trochlea as sagittal fractures, with 10-30 degrees in one group and 30-40 degrees in another group. In this case, the fracture line is about 20 degrees from the longitudinal axis of the talar trochlea. The fracture line is more clearly visible in the Anteroposterior (AP) view of the ankle X-ray for fractures in the 10-30-degree group, where the fracture line extends from the lateral sinus tarsi to the sulcus of the flexor hallucis longus [3]. The mechanism of injury varies based on fracture patterns.
The anatomy of the talus is unique with respect to its articulations, osseous structure and blood supply. Most of its surface is covered by articular cartilage and has no muscular or tendinous attachments. The main blood supply to the talar body comes from the posterior tibial artery, which gives rise to the artery of the tarsal canal, supplying the posterior and lateral two-thirds of the body. It also provides a deltoid branch that courses through the ligament and supplies blood flow to the medial aspect of the body [4].
In the present review of the literature consisting of 14 case reports, 7 cases (50%) were fixed through an anteromedial approach, 3 cases (21.4%) were fixed through a combined anteromedial and anterolateral approach and 2 cases (14.2%) were fixed through an anterolateral approach, one of which also required a lateral incision to fix a fibula fracture. Additionally, 2 cases (14.2%) were fixed through percutaneous fixation, one of which involved arthroscopic-assisted reduction [Table/Fig-6] [1,2,5-15].
Compilation of previous similar case reports [1,2,5-15].
| Authors | Year and place for study | Pattern of fracture | Approach | Fixation | Follow-up | Outcome | Complications |
|---|
| Mendonca AD et al., [7] | 2004
Wales, UK | Talar body fracture in sagittal and coronal plane with medial malleolus fracture. | Anteromedial | Talus fixed with one CC screw and medial malleolus fixed with 2 lag screws. | 6 months | Full ROM | None |
| Geary NP [11] | 2004
Wirral, UK | Talar body fracture in sagittal and coronal plane. | Arthroscopic assisted reduction and percutaneous fixation | Talus fixed with three CC screws. | Not mentioned | Not mentioned | Not mentioned |
| Shah K and Hakmi A [6] | 2004
London, UK | Sagittal plane fracture of talar body with medial malleolus fracture. | Closed percutaneous | Percutaneous two CC screw fixation for medial malleolus and talus fixed with two CC screws. | Not mentioned | Not mentioned | Not mentioned |
| Saidi H et al., [15] | 2008
Marrakesh, Morocco | Talar body fracture in sagittal plane and medial malleolus fracture. | Anteromedial | Talus fixed with two screws and medial malleolus fixed with two screws. | 6 months | Good, painless ROM | None |
| Clement ND et al., [10] | 2010
Edinburgh, UK | Medial talar body fracture in sagittal plane with pan-talar dislocation, medial malleolus fracture. | Anteromedial | Malleolus fixed with single malleolar screw, Talar body is excised and calcaneocuboid fixed with k-wires, bridging external fixator. | 15 months | Plantar flexion-20 degrees, dorsiflexion-10 degrees, inversion-20 degrees and eversion-10 degrees, with full power (5/5 MRC scale) in all planes | Minimal pain on prolonged walking, Ambulating using stick after 15 months |
| Mechchat A et al., [5] | 2014
Morocco | Talar body and neck fracture in sagittal and coronal plane with medial malleolus fracture. | Anteromedial | Talus fixed with two CC screws and medial malleolus fixed with malleolar screw and k-wire. | 14 months | Plantar flexion-20 Dorsiflexion-10 Inversion-20 Eversion-10 AOFAS- 87/100 | Minimal post-traumatic osteoarthritic changes of the ankle joint, no collapse of the talar body and no joint incongruity |
| Arkesh M et al., [2] | 2016
New Delhi, India | Talar body fracture in sagittal plane, medial malleolus fracture. | Anteromedial and anterolateral | Talus fixed with 2 Herbert screws from either direction and medial malleolus fixed with two partially threaded
4.5 CC screws. | 6 months | Loss of 5 degrees terminal dorsiflexion compared to normal | Mild pain on prolonged walking |
| Oesman I and Nugroho A [1] | 2019
Jakarta, Indonesia | Talar body fracture in both sagittal and coronal plane with medial malleolus fracture. | Anteromedial and anterolateral | ORIF with plate fixation for talus and tension band wiring for medial malleolus. | 1 year | Full range of movements | None |
| Lahrach K et al., [9] | 2019
Morocco | Talar body fracture in sagittal plane. | Anteromedial | Malleolus fixed with two malleolar screws; Talus fixed with two CC screws. | 6 months | Full recovery | None |
| Chen KM et al., [14] | 2020
Taichung, Taiwan | Talar body fracture in both sagittal and coronal plane with talar neck comminution, bimalleolar fracture. | Anteromedial and anterolateral. | Mini-hook plate for lateral malleolus, tension band wiring for medial malleolus, single Herbert screw for talus fracture. | 10 months | 90 on the Baird and Jackson Scoring System and 95 on the American orthopaedic foot and ankle society ankle- hindfoot scale | None |
| Jha AK et al., [13] | 2021
Jamshedpur, India. | Sagittal plane fracture of talar body and neck. | Anteromedial | Talus fixed with two cannulated screws and medial malleolus fixed with malleolar screws and k-wire. | 14 months | AOFAS score- 87. plantar flexion-20 degrees, dorsiflexion-10 degrees and eversion-10 degrees | Minimal post-traumatic osteoarthritic changes of the ankle joint. |
| Kumar PS [8] | 2021
Navi Mumbai, India | Talar body fracture in both sagittal and coronal plane with medial malleolus fracture. | Anteromedial | Talus fixed with two Herbert screws and medial malleolus fixed with two malleolar screws. | 1 year | Full range of movements equal to opposite side | Occasional pain on prolonged standing and walking |
| Van Rooijen JL et al., [12] | 2023
Maastricht, Netherlands | Talar body fracture in sagittal plane with anterolateral intra-articulated tibia fracture and distal fibula fracture with syndesmotic injury. | Anterolateral and lateral | Emergency External fixation.
14 days later-talus fixed with two 4.5 Herbert screws, tillaux fragment fixed with 4 mm cannula tied screw, fibula fixed with 3.5 mm locking bridging plate and syndesmoses fixed with positional screw through the plate. | Online follow-up for 12 months | Full weight bearing in 3 months | Some of the hardware was removed due to irritation 12 months
after the initial surgery |
CC: Cancellous compression; ROM: Range of motion; AOFAS: American orthopaedic foot and ankle score; ORIF: Open reduction and internal fixation; MRC: Medical research council
Two-screw fixation of the talus was performed in 9 cases (64.2%), while single-screw fixation was done in 2 cases (14.2%). Three-screw fixation was used in 1 case (7.14%) and mini-plate fixation was applied in another case (7.14%). In 1 case (7.14%), a small fragment in the posteromedial body was excised.
A total of 9 cases (64.2%) reported good outcomes with normal or near-normal range of movements, although two of these cases experienced minimal pain during prolonged walking as a complication. A total of 3 cases (21.4%) had poor outcomes with decreased range of movements at their final follow-up, with two cases exhibiting osteoarthritic changes in the ankle joint. The outcomes for the other 2 cases (14.2%) were not mentioned.
Through the present review, the most preferred approach was the anteromedial approach with osteotomy of the medial malleolus, which preserves the blood supply of the talar body through a branch to the deltoid ligament. In the present case, the anteromedial approach utilised the fracture window of the medial malleolus. The usual fixation for sagittal fractures involves either a single screw or double screw fixation, performed from the medial side or from both the medial and lateral sides.
Sneppen et al., defined sagittal fractures as those with a vertical line closer to the sagittal plane [15]. Complications such as avascular necrosis and post-traumatic osteoarthritis are common in talar body fractures due to the involvement of the articular surfaces on either side, particularly in Sneppen type C (sagittal shearing) and type D (posterior tubercle) fractures [15]. However, this specific pattern of sagittal shear fracture of the talar body, along with the medial malleolus, has an advantage due to the intact deltoid ligament, which preserves the blood supply on the medial side.
Conclusion(s)
Considering the rarity and associated complications, the fixation of talar body fractures in the sagittal plane, along with bimalleolar fractures, is challenging. Proper planning must be done regarding the timing of surgery, taking into account the swelling and soft tissue status. Adequate anatomic reduction and rigid fixation, combined with good surgical techniques and postoperative rehabilitation, are key to achieving favourable clinical outcomes.
CC: Cancellous compression; ROM: Range of motion; AOFAS: American orthopaedic foot and ankle score; ORIF: Open reduction and internal fixation; MRC: Medical research council
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jul 06, 2024
Manual Googling: Sep 21, 2024
iThenticate Software: Nov 20, 2024 (13%)
[1]. Oesman I, Nugroho A, A rare combination of closed fracture of right talar body Sneppen 2 with associated medial malleolus: A case reportInt J Surg Case Rep 2019 65:20-26.Epub 2019 Oct 1610.1016/j.ijscr.2019.10.01031678695PMC6838554 [Google Scholar] [CrossRef] [PubMed]
[2]. Arkesh M, Gaba S, Das S, Palanisamy JV, Trikha V, A rare combination of sagittal plane fracture of talar body with medial malleolus fracture: Case report and review of literatureJ Clin Orthop Trauma 2016 7(Suppl 1):30-34.Epub 2016 Oct 2710.1016/j.jcot.2016.10.00328018067PMC5167511 [Google Scholar] [CrossRef] [PubMed]
[3]. Inokuchi S, Kiyohisa O, Usami N, Classification of fractures of the talus: Clear differentiation between neck and body fracturesFoot Ankle Int 1996 17(12):748-50.10.1177/1071100796017012068973897 [Google Scholar] [CrossRef] [PubMed]
[4]. Sundararajan SR, Badurudeen AA, Ramakanth R, Rajasekaran S, Management of talar body fracturesIndian J Orthop 2018 52(3):258-68.10.4103/ortho.IJOrtho_563_1729887628PMC5961263 [Google Scholar] [CrossRef] [PubMed]
[5]. Mechchat A, Bensaad S, Shimi M, Elibrahimi A, Elmrini A, Unusual ankle fracture: A case report and literature reviewJ Clin Orthop Trauma 2014 5(2):103-06.Epub 2014 Jun 710.1016/j.jcot.2014.05.00325983480PMC4085359 [Google Scholar] [CrossRef] [PubMed]
[6]. Shah K, Hakmi A, Unusual ankle injury- A case reportThe Foot 2004 14(3):169-72.10.1016/j.foot.2004.03.005 [Google Scholar] [CrossRef]
[7]. Mendonca AD, Maury AC, Makwana NK, A simultaneous fracture of the tibia and talar bodyFoot and Ankle Surgery 2004 10(1):45-47.10.1016/S1268-7731(03)00109-7 [Google Scholar] [CrossRef]
[8]. Kumar PS, Sagittal and coronal plane fracture of talar body, an unusual combination with medial malleolus fracture: A case reportJournal of Clinical Orthopaedics 2023 8(2) [Google Scholar]
[9]. Lahrach K, El Kadi K, Marzouki A, Boutayeb F, Talar body fracture combined with medial malleolar fracture: A case report and literature reviewPan Afr Med J 2019 32:5710.11604/pamj.2019.32.57.616631223349PMC6560992 [Google Scholar] [CrossRef] [PubMed]
[10]. Clement ND, Phillips SN, Biant LS, The Edinburgh variant of a talar body fracture: A case reportJ Orthop Surg Res 2010 5:9210.1186/1749-799X-5-9221143899PMC3006367 [Google Scholar] [CrossRef] [PubMed]
[11]. Geary NP, Arthroscopically assisted internal fixation of a talus body fractureInjury 2004 35(1):86-89.10.1016/S0020-1383(02)00374-114728962 [Google Scholar] [CrossRef] [PubMed]
[12]. van Rooijen JL, Theeuwen DMJ, van Montfort G, Bransen J, Poeze M, A “logsplitter” like injury of the ankle: A case reportFoot & Ankle Surgery: Techniques, Reports & Cases 2023 3(3):10030510.1016/j.fastrc.2023.100305 [Google Scholar] [CrossRef]
[13]. Jha AK, Kumar R, Baranwal AK, Unusual ankle fracture: A literature reviewGlobal Journal for Research Analysis 2021 10(11):70-71.10.36106/gjra/6502351 [Google Scholar] [CrossRef]
[14]. Chen KM, Ko CY, Ho TY, Chen HT, Hsu HC, Hung CH, A combination of bimalleolar fracture and fracture on talar body and neck: A rare case reportMedicine 2020 99(26):e2086210.1097/MD.000000000002086232590787PMC7328999 [Google Scholar] [CrossRef] [PubMed]
[15]. Saidi H, Ayach A, Fikry T, Unusual fracture of the body of the talus: A case report and literature reviewMed Chir Pied 2008 24(1):22-24.10.1007/s10243-007-0139-y [Google Scholar] [CrossRef]