One of the goals of orthodontic treatment is to achieve stable occlusal relationships and facial aesthetics by correcting malocclusion [1]. The tendency of the teeth to return to their pretreatment positions after orthodontic treatment is known as relapse [2]. The relapse of teeth following orthodontic treatment has been the subject of ongoing interest, and numerous studies in the past have reported on this phenomenon [1,3-5]. The tendency for relapse is claimed to be highest during the immediate post-debonding period [6]. Various factors have been attributed to this tendency, including continued growth, improper muscular balance, persisting oral habits, the type of retainer used, and ICW [7,8].
The goal of the retention phase of orthodontic treatment is to maintain the positions of teeth after correction, using retainers, which may be either removable or fixed [9]. In a review by Littlewood SJ et al., the effects of different retention procedures on the stability of tooth positions following orthodontic treatment were studied. It was found that multi-stranded bonded retainers were slightly better at reducing relapse in the lower arch than thermoplastic retainers [10].
In recent years, self-ligating brackets have gained popularity in orthodontics due to their increased efficacy and efficiency [11]. Self-ligating bracket systems are categorised into two types based on the slot closure mechanics: active and passive brackets [12]. The passive self-ligating bracket system offers less frictional resistance compared to other ligation systems. This means that the forces exerted by the arch wire are transferred directly to the teeth and their supporting structures without being absorbed or altered by the ligature system [13]. Self-ligating brackets have many advantages over conventional bracket systems, including reduced treatment time, better patient acceptance, and increased efficiency [14]. The Damon self-ligating system claims to expand the arch in the posterior region through bodily movement [15,16]. However, there is a lack of strong evidence regarding the influence of self-ligating bracket systems compared to conventional bracket systems on relapse.
The present study aimed to evaluate the retention of orthodontic treatment performed with two different bracket systems.
Materials and Methods
An ambispective cohort study was conducted at Saveetha Dental College and Hospitals in Chennai Tamil Nadu, India from January 2024 to March 2024. The patients who received orthodontic treatment at the Department of Orthodontics between 2019 and 2022 were included in the study. Each patient was informed about the treatment plan, and their consent was obtained before participation. Ethical clearance for the study was granted by the Institutional Human Ethics Committee (IHEC) of Saveetha Dental College and Hospitals, with reference number: IHEC/SDC/ORTHO-2304/24/209.
Inclusion criteria:
Adult patients treated with either the MBT 022 bracket system (Ormco Mini-Diamond) or the passive self-ligating system (Damon® Q).
All permanent teeth erupted except for the third molars.
Class I molar relationship with mild to moderate crowding of 4-6 mm, treated without tooth extraction and retained with lower bonded retainers and upper Begg’s wrap-around retainers.
Availability of study models, photographs, and radiographs taken before treatment (T0) and at debonding (T1) from the same center.
Exclusion criteria:
Patients who received any other treatment in addition to typical conventional or passive-ligating systems.
Patients in whom the retainers failed or patients who did not use the removable retainers were excluded.
Patients with periodontal diseases, craniofacial abnormalities (such as cleft lip and palate), or those prescribed single-arch treatment.
Study Procedure
Records of 50 patients who fulfilled the selection criteria were enrolled in the study. Sample size calculation could not be performed in present study, as the sample size was dependent on the number of patients who reported at T2.
All 50 patients were called for oral prophylaxis two years after debonding (T2), but only 41 attended. For all 41 patients, lateral cephalograms were taken, and intraoral scanning was performed. These patients were divided into two groups: group 1 included 20 patients treated with the conventional MBT 022 bracket system (Ormco Mini-Diamond), while group 2 consisted of 21 patients treated with the standard torque version of passive self-ligating brackets (Damon® brackets). Ni-Ti archwires were used for the leveling and aligning phase in patients treated with the conventional McLaughlin Bennett Trevisi (MBT) bracket system. Patients treated with the conventional bracket system did not receive any appliances for arch expansion, and the achieved arch expansion post-treatment was solely due to archwire expansion.
Intraoral scans were taken to obtain digital models of the patients using the Runyes 3D intraoral scanner (Runyes Quickscan - Ningbo Runyes Medical Instrument Co., China) for all patients before the start of orthodontic treatment (T0) and at the time of debonding (T1). Intraoral scans and lateral cephalograms were conducted for all 41 patients who reported at the two-year recall (T2).
Digital models were obtained, and measurements were performed using the 3Shape Ortho Analyser software. Lateral cephalograms were analysed using the Facad® Ortho Tracing Software by Ilexis AB, Sweden.
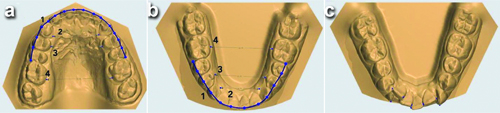
Parameters measured on digital models: The ICW, IPW, IMW, and AP at T0, T1, and T2 were measured. Contact Point Displacement (CPD) at T1 and T2 was calculated by measuring the labiolingual displacements of the anatomic contact points from the mesial of the right canine to the mesial of the left canine using a digital calliper with 0.1 mm accuracy [Table/Fig-1].
a) Occlusal view of the maxillary model showing 1- Arch Perimeter (AP), 2- Inter Canine Width (ICW), 3- Interpremolar (IPW) and 4- Intermolar Width (IMW); b) Occlusal view of the mandibular model showing 1- Arch Perimeter (AP), 2- Inter Canine Width (ICW), 3- Interpremolar (IPW) and 4- Intermolar Width (IMW); c) Occlusal view of the mandibular model showing contact point displacement measurement.
The LII is an index used to quantify the alignment of the mandibular anterior teeth. It was calculated by summing the five CPDs taken at T1 and T2 [17]. A higher difference between the LII calculated at T1 and T2 indicates a greater degree of relapse.
The Peer Assessment Rating (PAR) [18] was performed on the digital models by two examiners (MB and RKJ) at all time points (T0, T1, T2). Upper and lower labial segment alignment, buccal occlusion, overjet, overbite, and centerline were assessed for all patient models. A score was assigned to each characteristic contributing to malocclusion, and the sum of all the obtained scores represented the deviation from normal occlusion. The higher the score, the greater the level of malocclusion. An increase in the PAR score from T1 to T2 indicates that a relapse has occurred. The PAR reduction rate was calculated using the following formula:

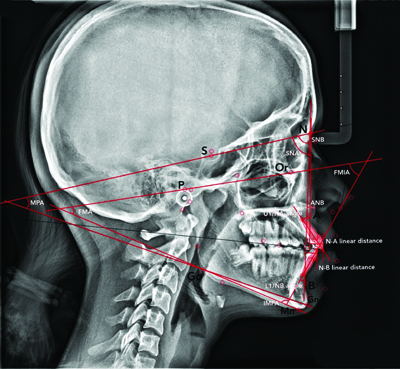
Parameters measured on lateral cephalograms: Sella, Nasion, A point (SNA), Sella Nasion B Point (SNB), A Point, Nasion, B Point (ANB), Mandibular Plane Angle (MPA), the upper incisor to NA (U1/NA) angle and linear distance, the lower incisor to NB (L1/NB) angle and linear distance, the Frankfort-mandibular Plane Angle (FMA), the Incisor-Mandibular Plane Angle (IMPA), and the Frankfort-mandibular Incisor Angle (FMIA). These measurements were taken at T1 and T2 [Table/Fig-2,3].
Lateral cephalogram showing SNA, SNB, ANB, Mandibular Plane Angle (MPA), upper incisor to NA (U1/NA) angle and linear distance, lower incisor to NB (L1/NB) angle and linear distance, Frankfort-mandibular Plane Angle (FMA), Incisor-mandibular Plane Angle (IMPA), and Frankfort-mandibular Incisor Angle (FMIA).
Description of the parameters measured of digital models and lateral cephalogram.
| 3D model parameters | Description | Cephalometric parameters | Description |
|---|
| ICW | The distance between the cusp tips of the right and left maxillary or mandibular canines. | SNA | The angle between the sella-nasion plane and the nasion-A plane |
| IPW | The distance between the distal pits of the right and left maxillary and mandibular first premolars. | SNB | The angle between the sella-nasion plane and the nasion-B plane |
| IMW | The distance between the mesial pits of the right and left maxillary and mandibular first molars. | ANB | The angle between the nasion-A plane and the nasion-B plane |
| AP | The distance from the mesial surface of the first permanent molar around the dental arch to the same point in the opposite side. | U1/NA angle | The angle between the long axis of the upper incisors and the nasion-A line |
| | U1/NA linear distance | The distance between the anterior-most point on the labial surface of the upper incisors and the nasion-A line |
| LII | Contact Point Displacement (CPD) is calculated by measuring the LL displacements of the anatomic contact points from the mesial of the right canine through the mesial of the left canine. LII is calculated by the addition of five CPDs. | L1/NB angle | The angle between the long axis of the lower incisors and the nasion-B line |
| | L1/NB linear distance | The distance between the anterior-most point on the labial surface of the lower incisors and the nasion-B line |
| | MPA | The angle between the SN plane and Go-Gn |
| | FMA | The angle between the FH plane and the mandibular plane |
| | IMPA | The angle between the long axis of the lower incisors and the mandibular plane |
| | FMIA | The angle between the FH plane and the long axis of the lower incisors |
ICW: Intercanine width; IPW: Interpremolar width; IMW: Intermolar width; AP: Arch perimeter; LII: Little’s irregularity index; CPD: Contact point displacement; LL: Labiolingual; S: Sella; N: Nasion; Go: Gonion; Gn: Gnathion
Statistical Analysis
The statistical analysis was performed using Statistical Package for Social Sciences (SPSS) version 26.0 software. Descriptive statistics, including the mean and standard deviation, were computed, followed by a normality assessment using the Shapiro-Wilk test. Since the data were normally distributed, a paired t-test was used to test the differences between the measured parameters at T1 and T2, while an independent t-test was applied to assess the differences between groups 1 and 2. The level of significance was set at p-value <0.05.
Results
Group 1 consisted of 13 females and 7 males, while group 2 included 15 females and 6 males. There were no significant differences in the mean age of patients in both groups, with a mean age of 29.5±5.8 years at the 2-year follow-up (T2).
Study Model Parameters
Intragroup comparisons: A significant reduction was noted in the maxillary Intermolar Width (IMW) (p-value <0.001) and maxillary Anterior-Posterior (AP) dimension (p-value=0.01) for group 1 at T2 [Table/Fig-4]. A significant reduction was observed in the maxillary ICW (p-value <0.001), IPW (p-value <0.001), IMW (p-value=0.04), and the Mandibular Alignment Index (LII) (p-value=0.01) for group 2 at T2 [Table/Fig-4].
Intragroup comparison of the model parameters.
| Paired samples | Group 1 | Group 2 |
|---|
| Mean±SD at T1 | Mean±SD at T2 | T1-T2 Mean±SD | p-value | Mean±SD at T1 | Mean±SD at T2 | T1-T2 Mean±SD | p-value |
|---|
| Maxillary ICW | 33.5±2.79 | 33.9±2.09 | -0.36±0.79 | 0.18 | 34.1±1.32 | 33.8±1.43 | 0.37±0.18 | <0.001* |
| Maxillary IPW | 37.27±1.99 | 37.02±1.7 | 0.25±0.28 | 0.21 | 35.89±1.55 | 34.48±1.53 | 0.40±0.14 | <0.001* |
| Maxillary IMW | 45.16±0.85 | 44.74±0.87 | 0.41±0.10 | <0.001* | 41.94±1.09 | 41.67±0.89 | 0.27±0.36 | 0.04* |
| Maxillary AP | 75.04±5.51 | 73.63±4.70 | 1.41±1.56 | 0.01* | 71.38±3.82 | 71.79±5.38 | -0.48±.57 | 0.36 |
| Mandibular ICW | 25.7±2.26 | 25.92±2.02 | -0.14±0.27 | 0.12 | 25.1±0.85 | 25.2±0.52 | -0.22±0.34 | 0.84 |
| Mandibular IPW | 32.09±1.89 | 32.19±1.68 | -0.10±0.24 | 0.21 | 29.63±2.05 | 29.80±1.87 | -0.16±0.42 | 0.24 |
| Mandibular IMW | 38.67±0.95 | 38.63±0.53 | 0.04±0.78 | 0.86 | 35.84±0.33 | 36.23±0.32 | 0.38±0.12 | 0.11 |
| Mandibular AP | 63.08±2.78 | 63.85±2.44 | -0.77±1.93 | 0.23 | 59.06±4.64 | 59.08±4.05 | -0.024±0.73 | 0.92 |
| LII | 2.14±0.64 | 2.08±1.15 | 0.06±0.73 | 0.77 | 0.93±1.17 | 1.17±1.23 | -0.23±0.24 | 0.01* |
*p-value <0.05, Paired t-test; ICW: Intercanine width; IPW: inter-premolar width; IMW: Intermolar width; AP: Arch perimeter; LII: Little’s irregularity index
Intergroup comparisons: Significant differences in relapse (T1-T2) were noted in maxillary IPW (p-value <0.001), IMW (p-value <0.001), AP (p-value=0.04), and LII (p-value=0.03) [Table/Fig-5]. Relapse of maxillary IPW and IMW was significantly greater in group 2 (p-value <0.001). Relapse in mandibular AP was significantly higher (p-value=0.04) in group 1.
Intergroup comparisons of model parameters of both maxilla and mandible.
| Independent samples | p-values of intergroup comparison at T1 | p-values intergroup comparison at T2 | p-values of relapse intergroup comparison (T1-T2) |
|---|
| Maxillary ICW | 0.83 | 0.78 | 0.87 |
| Maxillary IPW | 0.05 | 0.14 | <0.001* |
| Maxillary IMW | 0.08 | <0.001* | <0.001* |
| Maxillary AP | 0.54 | 0.82 | 0.04* |
| Mandibular ICW | 0.45 | 0.29 | 0.39 |
| Mandibular IPW | 0.10 | 0.008* | 0.83 |
| Mandibular IMW | 0.09 | 0.00* | 0.16 |
| Mandibular AP | 0.28 | 0.005* | 0.22 |
| LII | 0.05 | 0.04* | 0.03* |
*Independent t-test, p-value <0.05
Cephalometric Parameters
Intragroup comparisons: There was a significant increase in the U1/NA angle and L1/NB angle in group 2 at T2, as well as in the Incisor-Mandibular Plane Angle (IMPA) for both groups 1 and 2 at T2 (p-value <0.001) [Table/Fig-6].
Intragroup comparison of the cephalometric parameters.
| Paired samples | Group 1 | Group 2 |
|---|
| Mean±SD at T1 | Mean±SD at T2 | T1-T2 Mean±SD | p-value | Mean±SD at T1 | Mean±SD at T2 | T1-T2 Mean±SD | p-value |
|---|
| SNA | 82.89±2.79 | 83.26±1.94 | -0.37±0.75 | 0.15 | 81.60±0.46 | 81.47±0.87 | 0.13±0.91 | 0.66 |
| SNB | 80.33±2.26 | 80.65±1.67 | 0.32±0.98 | 0.33 | 79.89±0.56 | 80.42±0.59 | -0.53±0.04 | 0.08 |
| ANB | 2.56±0.39 | 2.58±0.59 | 0.02±0.36 | 0.86 | 1.71±0.44 | 1.05±0.64 | 0.13±0.53 | 0.45 |
| U1/NA angle | 31.23±3.90 | 32.27±3.58 | -1.04±1.70 | 0.06 | 35.5±1.38 | 37.92±1.52 | -2.41±0.14 | <0.001* |
| U1/NA linear distance | 4.28±2.9 | 4.94±1.87 | -0.66±0.35 | 0.23 | 4.02±1.6 | 5.02±2.1 | -1±1.82 | 0.14 |
| L1/NB angle | 26.91±2.72 | 28.01±2.92 | -1.90±0.17 | 0.37 | 27.52±0.68 | 29.55±2.72 | -2.3±0.24 | <0.001* |
| L1/NB linear distance | 4.69±2.03 | 5.24±1.59 | -0.55±0.39 | 0.30 | 4.04±1.20 | 4.91±2.4 | -0.87±0.89 | 0.09 |
| MPA | 29.36±3.2 | 30.06±0.98 | -0.30±1.2 | 0.11 | 29.18±1.82 | 29.98±0.54 | -0.8±1.63 | 0.08 |
| FMA | 23.91±1.09 | 25.85±1.67 | -1.88±0.47 | 0.10 | 24.74±2.48 | 25.37±1.50 | -0.63±0.80 | 0.07 |
| FMIA | 53.00±3.61 | 54.84±1.80 | -1.84±0.64 | 0.14 | 54.20±2.88 | 55.23±1.98 | -1.03±0.68 | 0.34 |
| IMPA | 99.31±6.11 | 105.92±5.11 | -6.61±6.39 | <0.001* | 98.01±2.86 | 101.45±2.08 | -3.44±4.25 | <0.001* |
*p-value <0.05, Paired t-test; U1/NA: Upper incisor to NA plane; L1/NB: Lower incisor to NB plane
Intergroup comparisons: Significant differences in relapse (T1-T2) were noted in the U1/NA angle, L1/NB angle, and IMPA (p values of 0.01, 0.002, and 0.04, respectively) [Table/Fig-7]. The U1/NA angle and L1/NB angle increased significantly in group 2. IMPA was significantly increased in group 1 (p-value <0.01) [Table/Fig-7].
Intergroup comparison of the cephalometric parameters.
| Independent samples | p-values of intergroup comparison at T1 | p-values intergroup comparison at T2 | p-values of relapse intergroup comparison (T1-T2) |
|---|
| SNA | 0.21 | 0.38 | 0.08 |
| SNB | 0.41 | 0.19 | 0.36 |
| ANB | 0.12 | 0.09 | 0.23 |
| U1/NA angle | 0.22 | 0.003* | 0.01* |
| U1/NA linear distance | 0.45 | 0.06 | 0.05 |
| L1/NB angle | 0.11 | 0.02* | 0.002* |
| L1/NB linear distance | 0.18 | 0.16 | 0.46 |
| MPA | 0.09 | 0.07 | 0.73 |
| FMA | 0.15 | 0.55 | 0.17 |
| FMIA | 0.07 | 0.26 | 0.38 |
| IMPA | 0.08 | 0.01* | 0.04* |
*p-value <0.05, Unpaired t-test
PAR scores: The PAR reduction rate (%) from T0 to T1 was 97.15±4.41 for group 1 and 96.85±5.8 when comparing T0 with T2. For group 2, the PAR reduction rate (%) from T0 to T1 was 98.05±2.1 and 93±2.1 for T0 to T2 [Table/Fig-8].
Mean and Standard Deviation (SD) of PAR scores at different time points.
| Groups | PAR score |
|---|
| Mean±SD at T0 | Mean±SD at T1 | Mean±SD at T2 |
|---|
| Group 1 | 20.01±7.32 | 0.57±0.82 | 0.63±0.44 |
| Group 2 | 21.58±8.20 | 0.42±0.94 | 1.51±1.73 |
Discussion
The stability of the results achieved after orthodontic treatment depends on various factors, such as the amount of force used during treatment, the degree of change in arch dimensions [19], the type of retainers used [8], and the persistence of oral habits [7]. Despite the advantages of self-ligating brackets over conventional ones, the question of whether self-ligating systems exhibit better stability post-treatment remains debatable. In the present study, stability was assessed in terms of changes in transverse dimensions in digital models, cephalometric changes, and changes in the PAR index over two years. The retention protocol was uniform for all patients, with a lingual bonded retainer and Begg’s wrap-around retainer provided to all patients at T1.
Transverse dimensions: In present study, it was observed that self-ligating brackets exhibited more relapse than conventional brackets at T2. While the conventional bracket group experienced a significant decrease in the maxillary Intermolar Width (IMW) post-treatment, the self-ligating bracket group demonstrated relapse in all three measured widths: maxillary Intercanine Width (ICW), IPW, and IMW. These findings differ from those of a study conducted by Yu Z et al., which aimed to assess the long-term stability of orthodontic treatment by evaluating 60 subjects divided into two groups-one treated with self-ligating brackets (SL) and the other with conventional brackets (CL) [16]. Digital models were utilised to assess the PAR index and LII for the patients, and the follow-up period extended to more than five years post-retention. There were no significant changes in the maxillary ICW and IMW for either group. The discrepancies in the findings may be attributed to the fact that their sample consisted of patients with 5 mm or less crowding pretreatment. Additionally, the mean age of their sample was lower than that of the sample in the present study.
In a study by Willeit FJ et al., 56 non extraction cases treated using passive self-ligating brackets were examined for transverse stability six years after treatment [20]. All parameters were measured using digital models obtained at different time points: pretreatment, post-debonding, 1 year post-treatment, and 6 years post-treatment. The upper and lower IPW showed a significant decrease (p-value <0.05) at the 6-year recall, while the lower Intermolar Width (IMW) decreased significantly (p-value <0.05) 1 year post-debonding. No relapse was detected in the canine region, which was attributed to the fact that all patients had received a bonded lingual retainer.
Anteroposterior dimension: The present study demonstrated an increase (p-value <0.05) in the proclination of the upper and lower incisors in patients treated with self-ligating brackets. The Incisor-Mandibular Plane Angle (IMPA) increased in both groups but was significantly higher (p-value <0.05) in patients treated with conventional brackets at the 2-year follow-up. These results are similar to those obtained in a study by Basciftci FA et al., where the L1/NB angle, L1/NB linear distance, and IMPA increased significantly (p-value <0.05) in patients treated with self-ligating brackets from the time of debonding to two years post-treatment [21]. The similarities in findings could be attributed to the use of comparable retention protocols; both studies implemented fixed retainers for all patients.
Atik E and Taner T compared patients treated with conventional brackets to those treated with Quad Helix appliances paired with the passive self-ligating system at three time points: pretreatment, debonding, and three years post-treatment [19]. When comparing cephalometric measurements at the time of debonding and three years post-treatment, they found no significant differences (p>0.05) in the U1/NA angle, linear distance, L1/NB angle, linear distance, and IMPA between both groups. The use of a Quad Helix in addition to the passive self-ligating system could be responsible for the stability of the results post-treatment.
Changes in LII: Yu Z et al., reported an increase in the LII for both groups during the follow-up period, but this change was not significant (p>0.05) [16]. In contrast, in the present study, LII increased for each group, and there was a significant difference in LII between the two groups (p-value <0.05). An increase (p-value <0.05) in LII was noted in the non extraction group treated with self-ligating brackets at the 1-year follow-up in a study conducted by Sahaypour B [22].
Changes in PAR: In the present study, relapse was observed at the 2-year recall in both groups. These results are similar to those obtained by Basciftci FA et al., who reported a gradual relapse from six months to two years after treatment [21].
Limitation(s)
In present study, each subject received treatment from different clinicians, which may introduce variability in the outcomes. Additionally, we were unable to perform sample size calculations since the number of participants depended on how many patients attended their scheduled appointments at the second time point (T2). To enhance the validity of present study findings, future research should be conducted to address these limitations and explore the effects with a more controlled approach.
Conclusion(s)
While both groups showed some relapse after treatment, subjects treated with passive self-ligating brackets experienced a significant relapse in the maxillary transverse widths in the canine, premolar, and molar regions, as well as in lower anterior crowding, compared to those treated with conventional ligation. Proclination of the upper anterior teeth increased significantly at T2 in subjects treated with the self-ligation system. This highlights the need for tailored retention strategies after orthodontic treatment to mitigate relapse in patients treated with passive self-ligating brackets.