The word ‘rugae’ is Greek in origin and signifies ‘seam.’ It indicates the point at which two distinct pieces, which have been embryologically separated from one another, converge to form a tissue or organ. Anatomical folds behind the incisive papillae on the anterior palate are called rugae, plica palatine, or transverse ridge folds [1]. During the third month (12th week to 14th week) of intrauterine life, palatal rugae emerge and cover the majority of the palatal shelves [2]. These are distinct structures whose positions and patterns remain constant throughout an individual’s lifetime. A child’s ability to suckle their finger, speak and taste food is physiologically aided by palate relief [3,4].
On each side, there are four to six palatal rugae. The complex interactions between mesenchymal and epithelial cells, which are governed by a family of homeobox genes, influence their growth and development. By the time intrauterine life comes to an end, the anterior rugae grow more prominent, and the posterior ones vanish, leading to an uneven distribution of the pattern [3]. They are protected from injury, trauma and extreme temperatures by the surrounding soft and hard tissues, which include the tongue, lips, cheeks, teeth, and underlying bone [5-9]. Research has demonstrated that the location of the dorsum of the tongue is crucial for the developmental stage of the palatal rugae. Different types of malocclusion also cause variations in the position of the tongue. Rugae are comparatively noticeable during the prenatal period. They are well-formed and have a typical orientation pattern at birth. They take on the final form of each person’s features during adolescence. Once formed, they may undergo alterations in size as a result of palate growth, but they never alter their shape [10,11]. While certain habits, such as thumb sucking or continuous pressure from braces and orthodontic therapy, as well as, orthodontic extractions, may cause localised alterations in the palatal rugae, the rugae remain stable and have been utilised for dental cast superimposition, which observes and tracks the movement of teeth in orthodontics [12,13].
In the world, dental malocclusions rank third in terms of frequency of occurrence. The most widely recognised factor responsible for this condition is genetic predisposition. An acceptable prognosis at a high level can be achieved with minimal orthodontic and surgical intervention whenever developing malocclusion is detected early and intercepted [10].
The relationship between the maxillary and mandibular permanent first molars, as proposed by Angle, is the cornerstone of the commonly employed classification system for dental malocclusion. Despite being seen as less flexible, Angle’s classification has been recognised as an effective approach that minimises intraobserver bias [10].
Since palatal rugae remain stable and unique to each person (like fingerprints), they have been deemed relevant for human identification. They serve as reliable reference points in orthodontics when superimposing cephalometric tracings taken before (pre) and after (post) treatment [14]. The study of palatal rugae is referred to as ‘palatoscopy’, sometimes known as ‘rugoscopy’ [15]. Allen, in 1889, suggested the application of palatal rugae patterns to aid in personal identification. Trobo Hermosa, a Spanish investigator, coined the phrase ‘palatal rugoscopy’ [16,17]. The classification by Thomas et al., serves as the framework for palatal rugae pattern identification. Rugae are categorised according to their number, length, shape and pattern of identification [18].
Thus, the aim of the present study was to investigate potential correlations between Angle’s classification of malocclusion and the palatal rugae pattern. Objectives were to identify the most common palatal rugae characteristics in Angle’s classification of malocclusion and to determine whether this may serve as an additional criterion to aid in the evaluation of malocclusion. This study seeks to address the deficiency in the current literature, as, to the knowledge of the authors, no similar research has been conducted in the Chengalpattu district, Tamil Nadu, India.
Materials and Methods
A cross-sectional observational study was conducted in the Department of Oral and Maxillofacial Pathology at SRM Kattankulathur Dental College and Hospital, Chengalpattu, Tamil Nadu, India. Data was collected from the years 2021 to 2024 and data analysis was done from October 2023 to April 2024. Study was carried the Institutional Ethics Committee (IEC) provided ethical clearance prior to the commencement of the study (Ethics Clearance Number: SRMIEC-ST0724-1466).
Inclusion criteria: Individuals from between the ages of 18-35 years, individuals who do not wear braces and have not undergone any previous orthodontic treatment, and individuals who do not have any fixed or removable partial dentures were included in the study.
Exclusion criteria: Individuals with palatal and lip anomalies, such as cleft palate and cleft lip, as well as, those with braces and partial dentures, were excluded from the study. Individuals with a prior history of orthodontic treatment were also eliminated.
Sample size: A convenience sampling was carried out for the study, which consisted of archival pretreatment dental casts of 105 individuals (class I: 38, class II: 57 and class III: 10), irrespective of gender, spanning ages from 18-35 years [Table/Fig-1].
Angle’s classification of malocclusion.

Study Procedure
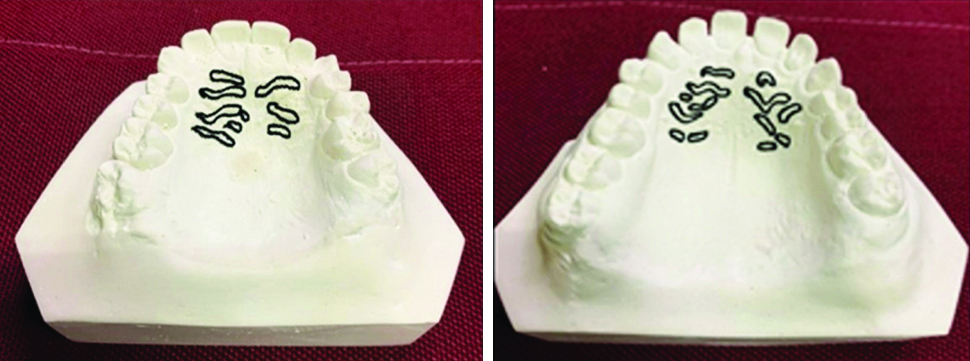
Upon analysing the archival pretreatment dental data of various subjects, only those who met the inclusion criteria were selected. All subjects were divided into class I, class II, and class III of Angle’s malocclusion without considering the aetiology of malocclusion. The number of subjects per class varied. The evaluation of the malocclusions was conducted clinically. The 105 samples were distributed according to malocclusion groups as follows: class I: 38, class II: 57 and class III: 10. The casts and records were retrieved from the Department of Orthodontics, where the archival casts belonged to patients who were healthy and did not have any diagnosed congenital abnormalities, inflammation, or trauma. There were no air bubbles or voids in any of the chosen casts, particularly in the anterior part of the palate. The rugae patterns of the study models were drawn using a pencil in good lighting and with the aid of a hand lens for magnification [Table/Fig-2].
Rugae pattern drawn and analysed on dental casts.
Using an High Definition (HD) camera, pictures of the casts were taken, printed and analysed further. To evaluate the pattern of palatal rugae, Thomas and Kotze’s classification was used [Table/Fig-3] [5].
Thomas and Kotze’s classification of palatal rugae [5].
Based on their shape, palatal rugae are divided into four types as: a) Straight; b) Curved; c) Wavy; d) Circular
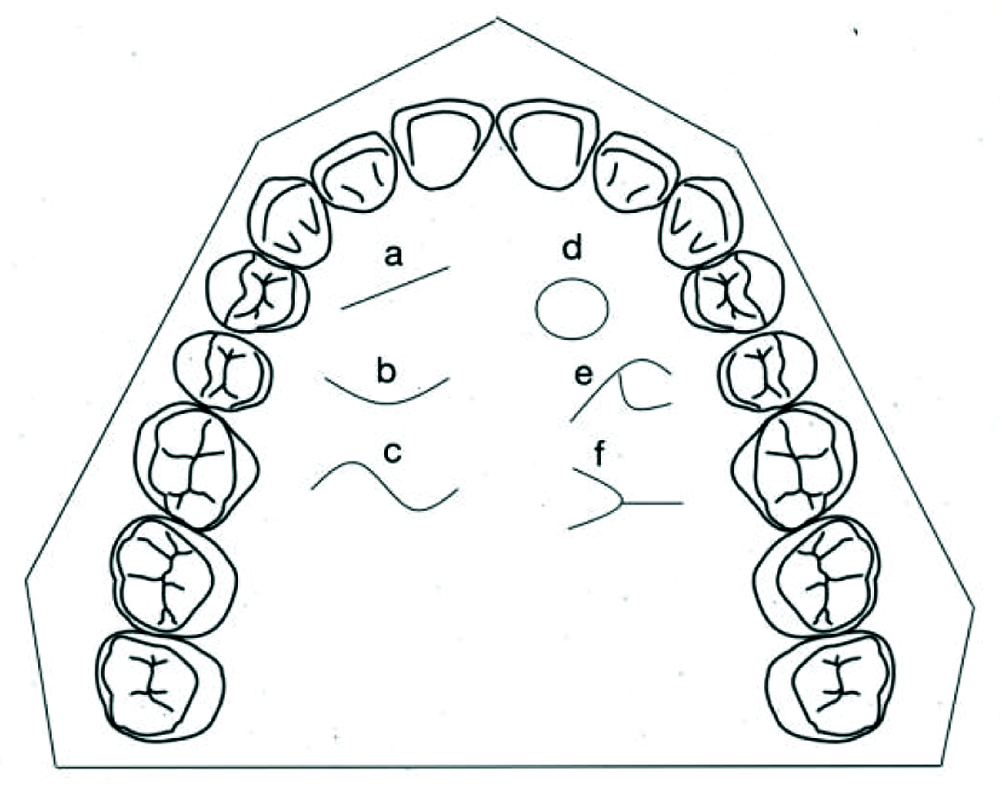
The joining of two rugae at the point of termination or origin was described as unification [Table/Fig-2] [5,19,20]. There were two categories for unification:
Diverging: Two rugae that shared the same origin but branched apart immediately were classified as diverging rugae.
Converging: Two rugae with distinct origins that joined at their lateral regions were regarded as converging rugae.
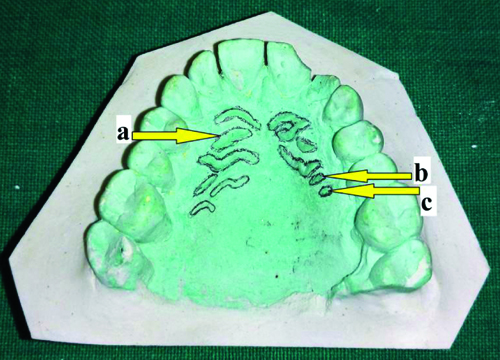
According to Lysell, the rugae were classified based on their lengths [Table/Fig-4] [14,21]. They were categorised as follows:
Lysell’s classification of palatal rugae [14,21]: a) Primary (5 mm or more); b) Secondary (3-5 mm); c) Fragmentary (less than 2 mm).
Statistical Analysis
After the analysis of the data was completed, the data was sent for statistical analysis. Statistics and Data (Stata) 17 software was used for this analysis. When a non normal distribution was observed using the Shapiro-Wilk test, which was applied to check for data normality, a non parametric test was conducted. The mean and Standard Deviations (SD) of the descriptive statistics were computed. To compare mean variations in the length and number of palatal rugae across the three classification groups, the Kruskal-Wallis test was used. The Chi-square test was employed to compare the pattern and orientation of palatal rugae between the three groups. Statistical significance was defined as a p-value of ≤0.05.
Results
A total of 105 archival pretreatment casts were evaluated. The data collected were from individuals between the ages of 18 years and 35 years, with a mean age of 26.5±23.64 years. This study was conducted irrespective of gender.
The total number of rugae, as well as, the pattern and orientation of the rugae in class I, class II and class III malocclusions, were evaluated both individually and collectively. According to the mean±SD length of rugae, class I malocclusions had more primary rugae (1.39±1.34 mm) than class II malocclusions (0.59±1.17 mm) and class III malocclusions (0.5±0.97 mm). In contrast to the straight pattern (p-value=0.1498), the rugae pattern analysis revealed that both wavy and curved patterns exhibited preponderance in all three classes of malocclusion (wavy: p-value=0.0001 and curved: p-value=0.0013). In all three malocclusion groups, the convergent orientation type (0.39±0.6) was more prevalent than the divergent orientation type (0.29±0.52).
However, the differences in the pattern, number, length and orientation of the palatal rugae between the malocclusion groups were not statistically significant [Table/Fig-5]. The results, however, did not indicate a specific pattern that is unique to any one type of malocclusion.
Statistical results comparing Angle’s classification of malocclusion with physical properties of palatal rugae.
| Parameters | Classification | Total | p-value |
|---|
| Class I | Class II | Class III |
|---|
| (N=38) | (N=57) | (N=10) | (N=105) |
|---|
| Length (mean±SD) (mm) | Primary (5 mm or more) | 1.39±1.34 | 0.59±1.17 | 0.5±0.97 | 0.87±1.27 | 0.0003 |
| Secondary (3 mm-5 mm) | 4.5±1.46 | 4.28±1.60 | 5±1.15 | 4.42±1.51 | 0.3764 |
| Fragmentary (less than 2 mm) | 0.73±1.11 | 1.14±1.36 | 1.7±1.70 | 1.04±1.33 | 0.1735 |
| p-value | 1 | 0.9999 | 0.9969 | 1 | - |
| Pattern (mean±SD) (n) | Wavy | 1.92±1.12 | 0.79±0.90 | 1.3±0.68 | 1.24±1.09 | 0.0001 |
| Curved | 1.71±1.27 | 2.14±1.12 | 0.70.82 | 1.84±1.22 | 0.0013 |
| Straight | 1.73±1.37 | 1.66±1.22 | 2.5±1.27 | 1.77±1.29 | 0.1498 |
| p-value | 1 | 1 | 0.9868 | 1 | - |
| Orientation (mean±SD) (n) | Converging | 0.39±0.59 | 0.33±0.55 | 0.7±0.82 | 0.39±0.6 | 0.3265 |
| Diverging | 0.29±0.46 | 0.32±0.57 | 0.2±0.42 | 0.29±0.52 | 0.8582 |
| p-value | 0.999 | 0.9983 | 0.9525 | 1 | - |
Discussion
The present study investigated the patterns, lengths and orientation of palatal rugae, as well as, their relationship to Angle’s classification of malocclusion. Although specific tendencies emerged among the malocclusion groups, the variation in outcomes illustrates the complexity of these structures.
Palatal rugae may differ depending on the type of malocclusion. Class I rugae are well-developed and symmetric, demonstrating maxillary-mandibular linkage. A narrower maxillary arch and more space between the upper and lower teeth render class II rugae anteriorly uneven, compressed and elongated. Class III rugae are more irregular and larger due to their position, as the maxilla adapts to accommodate the forward-positioned mandible, resulting in a wider arch [10]. Therefore, the correlation of the pattern of palatal rugae with Angle’s classification of malocclusion can help predict any dentoskeletal abnormalities in the future [22].
The present study classified specific rugae patterns according to various classes of malocclusion. In all three classes, statistically, wavy and curved patterns were appreciated more than the straight pattern. However, individually, class I malocclusion was identified as being characterised predominantly by wavy rugae, whereas class II malocclusion exhibited curved rugae patterns as the most prevalent. Class III malocclusion was characterised by rugae patterns that were notably straight. These results align with the findings of Dhiman I et al., who identified similar rugae characteristics in class II malocclusion, despite small variations observed in other classes [1].
Variations in length were particularly noticeable in the primary rugae. Class II malocclusion demonstrated the longest primary rugae, a result consistent with previous research by Dhiman I et al., [1]. This discovery indicates that the length of the rugae may function as a potential diagnostic marker for class II malocclusion, facilitating the early detection of skeletal anomalies.
The observed variations in length and patterns among malocclusion groups were statistically significant, corroborating the findings of Fatima F et al., who also noted minor relationships with low clinical importance [15]. The current study supports the idea that palatal rugae serve as distinctive identifiers, in comparison to existing literature.
Indira A et al., observed that no two individuals possess identical rugae patterns, and these structures lack bilateral symmetry, rendering them a dependable characteristic for forensic identification [23]. Nonetheless, research conducted by Alzahrani SK et al., revealed no substantial link between rugae patterns and malocclusion, highlighting the variety and the impact of sample size, technique, and demographic diversity [24].
Regional discrepancies in rugae patterns have been documented, with research by Paliwal A et al., identifying wavy patterns as the most prevalent across populations in Madhya Pradesh and Kerala, India [21]. This corresponds with the current study’s results for class I malocclusion and emphasises the influence of genetic and environmental factors on rugae formation. This diversity indicates the necessity for extensive, widespread investigations to validate these correlations and examine their universality.
Abazi MS et al., discovered that class I malocclusion presented gender-specific rugae configurations, with females primarily exhibiting a straight pattern and males a wavy pattern. Conversely, class II malocclusion exhibited a straight rugae pattern in both genders, while class III malocclusion demonstrated a prevalence of wavy patterns in females and curved patterns in males [3]. The present study similarly noted diverse patterns among malocclusion classes, underscoring the impact of malocclusion type on rugae formation.
Jose LK et al., documented irregular rugae patterns in class I, a forking pattern in class II, and wavy patterns in class III malocclusion. Their findings demonstrated a link between rugae length and malocclusion classes, notably class II and class III [10]. The present study supports such results, as distinct rugae patterns were observed in various malocclusion types. This is consistent with Thoke B et al., who observed notable differences in the number, length, and pattern of palatal rugae among malocclusion groups [25]. The results of the present study similarly demonstrated heterogeneity in these characteristics. Similar studies from the literature have been tabulated in [Table/Fig-6] [1,3,10,15,23-25].
| S. No. | Author’s names and year | Place of study | Sample size | Parameters assessed | Conclusion(s) |
|---|
| 1. | Dhiman I et al., 2021 [1] | Himachal Pradesh, India | 90 | Length, number, pattern and direction | i. All types of rugae were significantly distributed more on the right-side as compared to left-side on the palate.
ii. Length of the primary palatal rugae was found more in class II followed by class III and class I malocclusion.
iii. Among the pattern of rugae, curved pattern were more evident on both right and left-sides of all malocclusion groups.
iv. Horizontal directed orientation is more predominant on the right-side and posteriorly directed on the left-side of the first primary palatal rugae. |
| 2. | Fatima F et al., 2019 [15] | Pakistan | 184 | Length, pattern and orientation | i. The study found an association between the number of palatal rugae and the pattern of primary rugae with the Angle’s classes of malocclusion.
ii. However, the length and the orientation of the primary palatal rugae showed variable results. |
| 3. | Indira A et al., 2012 [23] | Bengaluru, India | 100 | Pattern | i. Based on this study, no two individuals have palates alike in their rugae configuration.
ii. Hence, palatal rugae can be one of the tools for personal identification in forensic odontological identification in the Indian context. In view of these findings, palatal rugae could be used as a personal print for identification. |
| 4. | Alzahrani SK et al., 2023 [24] | Taif, Saudi Arabia | 100 | Length, pattern, direction | i. Wavy and complex rugae were prevalent in class I and III malocclusions and showed statistically significant difference between class 1, 2 and 3 malocclusions (p=0.00, 0.014 and 0.016, respectively).
ii. The wavy pattern was higher in class I and horizontal and complex higher in class III. |
| 5. | Abazi MS et al., 2014 [3] | Pristina, Kosovo | 100 | Pattern, unification, length | i. Palatal rugae patterns in class I, II and III malocclusions show no significant difference between female and male subjects.
ii. In class I malocclusion, the straight pattern was dominant in female subjects and the wavy pattern was dominant in male subjects.
iii. The straight pattern was dominant in males and females with class II malocclusion.
iv. In class III malocclusion, the wavy pattern was dominant in female subjects and the curved pattern was dominant in male subjects. |
| 6. | Jose LK et al., 2022 [10] | Kerala, India | 120 | Length, pattern | i. The first primary rugae on both sides is longest in class III malocclusion. The second primary rugae on left-side is longest in class II. The third primary rugae on left-side is longest in class III group.
ii. Irregular pattern was observed more in class I malocclusion in first rugae on right and left-sides and second rugae on right and left-sides.
iii. Forking pattern was observed more in class II malocclusion in first and second rugae on right-side and third rugae in both sides.
iv. Wavy pattern was observed more in class III in first rugae on both sides and in second pattern on left-side.
v. The current study showed Palatal rugae length has definite co-relation with class II and class III malocclusion. Palatal rugae pattern has definite co-relation with all three Angles classes of malocclusion. |
| 7. | Thoke B et al., 2023 [25] | Sri Ganganagar, Rajasthan, India | 600 | Length, number, pattern and direction | i. Class I had a greater number and length of primary rugae as compared to class II and class III.
ii. Curved and wavy patterns of the primary palatal rugae were more noticeable on both the right and left sides in all malocclusion groups.
iii. The different malocclusion groups showed that the primary palatine third rugae were more commonly anteriorly directed in class I and posteriorly directed in class III. |
| 8. | Present study | Chengalpattu, Tamil Nadu, India | 105 | Length, pattern, number and orientation | i. The study found an association between the number of palatal rugae and the pattern of primary rugae with the Angle’s classes of malocclusion.
ii. Class I malocclusions had more primary rugae than class II malocclusions and class III malocclusions.
iii. Curved and wavy patterns of the primary palatal rugae were more in all malocclusion groups.
iv. In all malocclusion groups, convergent orientation type was more prevalent than divergent type. |
Nevertheless, in alignment with the extensive literature, no unique pattern was identified as conclusive for any particular malocclusion class, highlighting the intrinsic complexity and variety of palatal rugae. The present study enhances the existing evidence regarding the diagnostic use of palatal rugae in orthodontics. The discovered changes in rugae patterns, although not conclusive, offer significant insights into their function in recognising and forecasting dentoskeletal abnormalities. Additional study, especially longitudinal and multipopulational studies, is advised to improve the clinical relevance of palatal rugoscopy.
Limitation(s)
The present study was a single-centre study, and a manual method for tracing the rugae was used. To validate the usefulness of utilising palatal rugae for the early detection of malocclusion, more research is required. Scanners and other digital technologies can be employed in future research to add interest to this topic.
Conclusion(s)
The current study observed a significant relationship between the pattern and orientation of palatal rugae and Angle’s classification of malocclusion. However, no unique pattern was identified for any particular class of malocclusion. Further research needs to be conducted on this topic with a larger and equal sample size in each class of malocclusion.