Pain is one of the most dreaded fears among patients undergoing surgery, and it is especially intense after orthopaedic procedures [1]. To improve analgesia, local anaesthetics are often used with various perineural adjuvants. These adjuvants have been employed, with variable degrees of success, to accelerate the onset and extend the duration of nerve block analgesia [2], without additional systemic adverse effects. They not only provide intraoperative anaesthesia but also prolong analgesia in the postoperative phase.
The supraclavicular brachial plexus block is a cost-effective and safe method that offers optimal operating conditions and efficient postoperative analgesia [2]. It provides a rapid onset of dense anaesthesia with a single injection, making it ideal for operations involving the arm and forearm by achieving a more complete block of the median, radial, ulnar, and musculocutaneous nerves. The brachial plexus is most compact at the level of the trunks formed by the C5-T1 nerve roots. It is a highly reliable method of regional anaesthesia for the upper limb, sometimes referred to as the “spinal anaesthesia of the upper limb” [3].
Adjuvants such as opioids, epinephrine, alpha-2 adrenergic agonists, anti-inflammatory drugs, midazolam, adenosine, ketamine [4], dexmedetomidine [5], steroids [6], magnesium sulfate [7], and clonidine [8] have been evaluated for their ability to enhance local anaesthetics by synergistically extending the duration of sensory and motor blocks and decreasing the cumulative dose requirement.
Dexamethasone has been shown to extend the analgesic duration of brachial plexus blocks without causing major intraoperative and postoperative complications. This effect is due to its local action on nociceptive C-fibers mediated through glucocorticoid receptors and its anti-inflammatory action [9]. It also suppresses ectopic neuronal discharge [10] by altering the function of potassium channels in excitable cells. Dexmedetomidine, an alpha-2 agonist, has been shown to prolong the duration of brachial plexus blocks without causing major intraoperative and postoperative complications. This effect is attributed to alpha-2 stimulation on presynaptic and postsynaptic receptors, which inhibits neuronal firing and leads to hypotension, bradycardia, sedation, and analgesia [10,11].
The novelty of present study lies in providing high-level evidence on the optimal adjuvant for enhanced postoperative pain management, opioid reduction, and improved patient outcomes by directly comparing perineural dexmedetomidine versus dexamethasone in supraclavicular brachial plexus block. While previous studies have individually assessed the efficacy of dexmedetomidine and dexamethasone as adjuvants in regional anaesthesia, direct comparisons between these two agents when used perineurally in supraclavicular brachial plexus blocks are limited [3-6,12-14]. The findings of this study have the potential to inform clinical practice guidelines and contribute to opioid-sparing strategies in perioperative care. Thus, the aim of present study was to compare the effects of dexmedetomidine and dexamethasone as perineural adjuvants in the supraclavicular brachial plexus block.
Materials and Methods
The present interventional study was conducted in the Department of Anaesthesiology at Dhiraj Hospital, Vadodara, Gujarat, India from October 2023 to April 2024. Institutional Ethical Committee approval (SVIEC/ON/MEDI/SRP/OCT/23/39) was obtained, and written informed consent was secured from all patients.
Inclusion criteria: Patients aged 18 to 65 years, classified as ASA physical status I or II, scheduled for elective upper limb surgeries under supraclavicular block, and with no known history of allergy or sensitivity to local anaesthetics of the ester and amide types were included in the study. Both male and female patients who were willing to sign the written informed consent were considered eligible.
Exclusion criteria: Exclusion criteria encompassed patients who were unwilling to participate, those with arrhythmia or heart block, and individuals with renal, hepatic, cardiovascular, or respiratory diseases. Patients classified as ASA physical status III or higher, pregnant or lactating women, those with a known allergy to the study drugs, patients requiring supplementation of general anaesthesia, and those with any contraindication to supraclavicular block were also excluded.
Sample size calculation: Sample size was calculated using the following formula using MedCalc12.5 software:
nA=knβ and nβ=(1+1/k) {(z1-α/2+z1-β2)/(μA-μB)}
1-β= φ (z-z1-α/2)+ φ (-z-z1-α/2),
z=(μA-μB)/((1/nA+1/nB)-2)
where,
K=na\nB is the matching ratio
σ is the standard deviation
φ is the standard normal distribution function
φ-1 is the standard normal quantile function
α is type I error
β is type II error, meaning 1-β is power
Values Considered:
Type I error (α): 0.05
Type II error (α): 0.20 (Power=80%)
Standard deviation (σ): 200 minutes (estimated from previous studies on the duration of postoperative analgesia) [3].
Minimal clinically significant difference (Δ=μ_A-μ_B): 125 minutes in the duration of postoperative analgesia [3].
Matching ratio (k): 1 (equal group sizes).
Sample size per group (n): 41 participants
Considering practical constraints and the need to maintain the study’s power, 40 patients were included in each group, resulting in a total sample size of 80 patients. This slight reduction from 41 to 40 patients per group is acceptable and does not significantly impact the study’s power.
Study Procedure
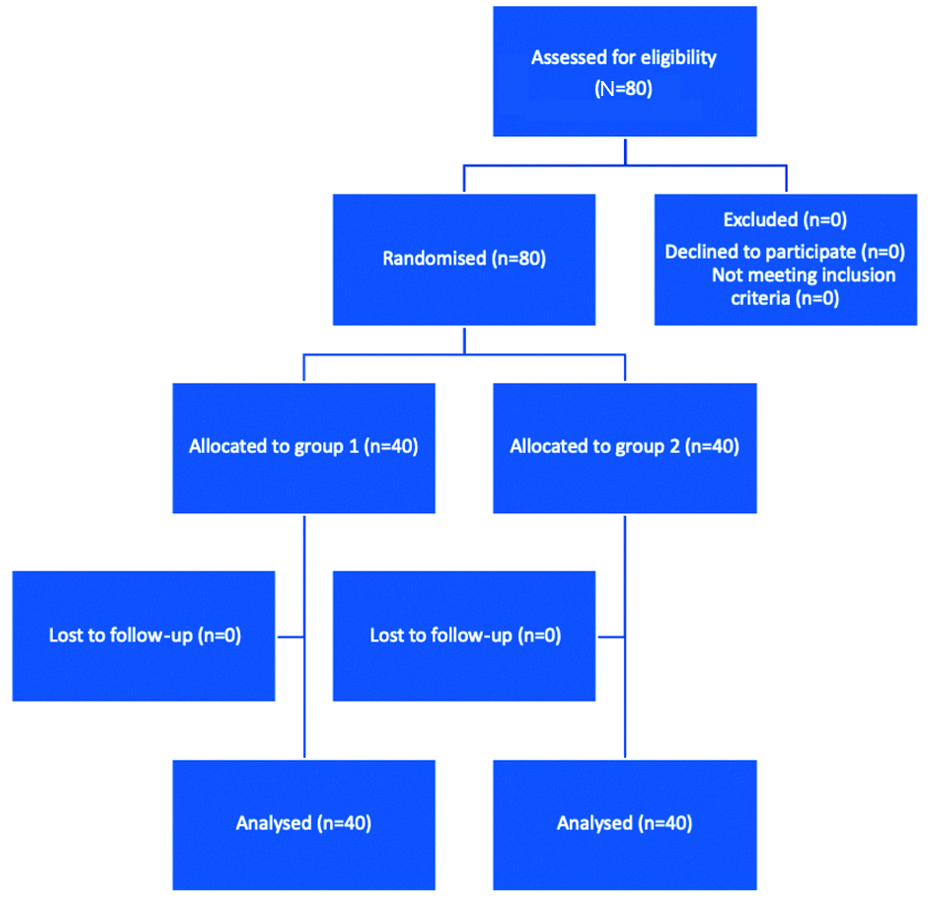
The patients were divided into two groups of 40 each using a closed envelope method. A Consolidated Standards of Reporting Trails (CONSORT) diagram is provided in [Table/Fig-1]. A detailed history was taken from each patient, and the purpose and protocol of the study were explained. After being moved to the premedication room, consent, history, and clinical status were reconfirmed. Routine monitors {Electrocardiogram (ECG), Non Invasive Blood Pressure (NIBP), SpO2} were attached, and baseline haemodynamic parameters {Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Mean Arterial Pressure (MAP) and SpO2} were noted at 0 min, 3 min, 5 min, 10 min, 15 min, 30 min, 45 min, 60 min, 90 min, and 120 min.
Progression of participants through the stages of a randomised study.
Group 1 received 12 cc of inj. lignocaine with adrenaline (0.2%), 13 cc of inj. bupivacaine (0.5%), 1.5 cc of inj. Normal Saline (NS), and 50 mcg of inj. dexmedetomidine. Total mixture: 27 cc [15].
Group 2 received 12 cc of inj. lignocaine with adrenaline (0.2%), 13 cc of inj. bupivacaine (0.5%), and 2 mL (8 mg) of inj. dexamethasone. Total mixture: 27 cc [16].
The drug was administered by an expert anaesthesiologist who was not involved in the study. Patients were observed after the successful block for haemodynamic changes, and the effects of the drugs were compared.
The Peripheral Nerve Stimulation (PNS)-guided supraclavicular block procedure involved patient positioning and skin disinfection. An insulated needle was inserted under PNS guidance into the supraclavicular fossa near the subclavian artery, where electrical impulses (0.5-1.5 mA) stimulated nerves to confirm placement. Local anaesthetic was then injected around the nerves. Efficacy was confirmed through sensory and motor assessments. The PNS device ensured precise needle placement, minimising the risk of nerve damage and optimising block success.
Preoperative assessment and preparation: All patients were informed about the purpose and nature of the study in understandable language and were included only after obtaining written consent. A comprehensive preoperative assessment was conducted, which included a detailed medical history, general examination, airway assessment, and evaluation of the block site. Vital signs and a systemic examination were also performed. Routine preoperative investigations were completed, and patients were instructed to fast for six hours for solids and four hours for liquids before the procedure. Written and informed consent was obtained, and an intravenous line was secured. Patients were educated on how to use the Visual Analogue Scale (VAS) for pain assessment.
Equipment and drug preparation: The necessary equipment, including an anaesthesia workstation, a Peripheral Nerve Stimulator (PNS), and a hypodermic block needle, was prepared. The required drugs were also made available: glycopyrrolate, ondansetron, bupivacaine (0.5%), lignocaine with adrenaline (0.2%), dexmedetomidine, dexamethasone, and emergency medications (atropine, ephedrine, mephentermine, and lignocaine 2%).
Intraoperative management: The patients were connected to multichannel monitors, and their vital signs were recorded. Glycopyrrolate and ondansetron were administered as premedication according to weight-based dosages. Under the guidance of an expert anaesthesiologist, a PNS-guided supraclavicular block was administered after identifying the anatomical landmarks.
Assessment of sensory blockade: The level of sensory blockade was assessed using the pinprick method. Data were collected on the onset of sensory block, defined as the time from drug injection to the loss of pinprick sensation.
Assessment of motor blockade [16]: Motor blockade was assessed using a 3-point scale, where: 0 indicated normal motor function with full flexion and extension of the elbow, wrist, and fingers; 1 indicated decreased motor strength, allowing movement of the fingers and/or wrist only; and 2 indicated complete motor blockade, with an inability to move the fingers. Assessments were conducted by the same observer at 5-minute intervals following drug injection until complete motor blockade was achieved. This systematic evaluation ensured accurate monitoring of motor function and allowed for precise documentation of the onset and duration of the blockade [16].
Adverse effects were noted in the Adverse Drug Reaction (ADR) form, and complications were recorded and treated accordingly. Postoperatively, all patients were transferred to the recovery room, where their vitals were monitored; the duration of sensory block and the duration of motor blockade were noted. Postoperative pain was assessed using the VAS at 30 minutes, one hour, three hours, five hours, seven hours, and 10 hours intervals. The duration of effective analgesia was recorded, along with the number of rescue analgesics required in the 24 hours following the procedure.
Duration of effective analgesia: Time interval between injection of drug to VAS ≥4.
Time of rescue analgesia needed: The time in minutes when Inj. Diclofenac sodium 1.5 mg/kg had to be administered intravenously for analgesia was noted [17].
Statistical Analysis
Variables such as patient demographics, surgical details, haemodynamics during and after surgery, duration of sensory and motor blocks, postoperative pain scores (VAS), and complications were observed. After a preliminary study involving 10 patients (5 per group), a sample size of 80 was calculated using MedCalc 12.5 software. The comparison of gender, ASA classification, and the presence of any complications was performed using the Chi-square test. Age, duration of surgery, duration of sensory and motor blocks, and haemodynamic parameters were presented as mean±SD and analysed using the t-test. A p-value of less than 0.05 was considered statistically significant, while a p-value of less than 0.001 was considered highly significant.
Results
A total of 80 patients were enrolled in the study, with 40 patients in each group. The demographic parameters, including age, weight, duration of surgery, gender distribution, and ASA physical status, were recorded. Group 1 had a significantly lower average age (35.38±9.03 years) compared to Group 2 (46.40±13.12 years) (p=0.000039), and the duration of surgery was longer in Group 1 (p=0.0159), though this had no significant impact on the study results. There were no significant differences between the groups regarding weight (p=0.0598), gender distribution, or ASA physical status [Table/Fig-2].
Results of demographic parameters.
| Parameters | Group 1 | Group 2 | p-value |
|---|
| Age (years) | 35.38±9.03 | 46.40±13.12 | 0.000039 |
| Weight (kg) | 59.73±11.60 | 64.03±8.24 | 0.0598 |
| Duration of surgery (minutes) | 94.6±15.7 | 87.5±9.0 | 0.0159 |
| Male gender | 20 (50.00%) | 20 (50.00%) | 1 |
| Female gender | 20 (50.00%) | 20 (50.00%) |
| ASA Grade I | 26 (65.00%) | 20 (50.00%) | 0.7403 |
| ASA Grade II | 14 (35.00%) | 20 (50.00%) |
Significant variations in heart rate were observed between the two groups at multiple time points. Group 2 generally exhibited higher heart rates at 5, 10, 45, 60, and 120 minutes post-administration (p<0.05). In contrast, Group 1 had higher heart rates at 15 and 30 minutes (p<0.05). No significant difference was noted at 90 minutes (p=0.6741) [Table/Fig-3].
Comparison of heart rate at various intervals post-anaesthesia.
| Time interval | Heart rate | p-value |
|---|
Group 1
(Mean±SD) | Group 2
(Mean±SD) |
|---|
| 0 min | 74.03±8.25 | 78.20±6.07 | 0.0118 |
| 3 min | 73.80±7.88 | 76.97±7.65 | 0.0714 |
| 5 min | 66.55±4.53 | 76.85±6.07 | <0.001 |
| 10 min | 69.78±4.10 | 76.78±7.53 | <0.001 |
| 15 min | 76.85±6.07 | 72.83±5.11 | 0.0019 |
| 30 min | 78.62±5.39 | 71.78±6.75 | <0.001 |
| 45 min | 71.35±5.91 | 77.20±4.55 | 1.62×10-6 |
| 60 min | 73.38±8.51 | 78.75±3.78 | <0.001 |
| 90 min | 76.72±7.20 | 76.10±5.99 | 0.6741 |
| 120 min | 74.78±7.85 | 79.45±6.14 | 0.004 |
The analysis of Systolic Blood Pressure (SBP) revealed statistically significant differences between the groups at various time points: at zero minutes (p<0.001), three minutes (p=0.0014), five minutes (p=0.0132), 10 minutes (p=0.0028), 15 minutes (p=0.0034), 30 minutes (p<0.001), and 60 minutes (p=0.0104). Group 2 exhibited higher SBP at certain intervals [Table/Fig-4].
Comparison of Systolic Blood Pressure (SBP) at various intervals post-anaesthesia.
| Time interval | SBP (mmHg) | p-value |
|---|
Group 1
(Mean±SD) | Group 2
(Mean±SD) |
|---|
| 0 min | 119.85±10.81 | 112.10±6.76 | <0.001 |
| 3 min | 110.10±8.72 | 116.40±8.27 | 0.0014 |
| 5 min | 114.40±6.06 | 110.85±6.45 | 0.0132 |
| 10 min | 111.20±7.52 | 106.80±5.00 | 0.0028 |
| 15 min | 112.55±7.73 | 108.28±4.51 | 0.0034 |
| 30 min | 112.25±7.21 | 120.75±9.82 | <0.001 |
| 45 min | 116.05±8.01 | 113.60±5.23 | 0.1091 |
| 60 min | 114.15±7.25 | 110.75±3.81 | 0.0104 |
| 90 min | 117.15±7.45 | 117.95±7.73 | 0.6389 |
| 120 min | 115.15±7.60 | 117.45±7.86 | 0.1873 |
Diastolic Blood Pressure (DBP) also demonstrated significant differences at five minutes (p=0.0002), 10 minutes (p<0.001), 15 minutes (p=0.0002), 30 minutes (p<0.001), 45 minutes (p=0.0105), 60 minutes (p<0.001), and 120 minutes (p<0.001) [Table/Fig-5].
Comparison of Diastolic Blood Pressure (DBP) at various intervals post-anaesthesia.
| Time interval | DBP (mmHg) | p-value |
|---|
Group 1
(Mean±SD) | Group 2
(Mean±SD) |
|---|
| 0 min | 73.50±9.38 | 70.30±6.57 | 0.0811 |
| 3 min | 75.45±8.29 | 77.55±6.02 | 0.1986 |
| 5 min | 67.60±5.46 | 72.75±6.25 | 0.0002 |
| 10 min | 73.65±7.90 | 67.30±4.47 | <0.001 |
| 15 min | 67.05±2.68 | 71.30±6.33 | 0.0002 |
| 30 min | 69.50±6.76 | 79.10±5.96 | <0.001 |
| 45 min | 70.40±6.08 | 74.30±7.18 | 0.0105 |
| 60 min | 70.30±5.74 | 76.45±4.11 | <0.001 |
| 90 min | 74.60±6.87 | 72.65±13.58 | 0.4203 |
| 120 min | 72.75±6.61 | 117.45±7.86 | <0.001 |
SpO2 levels remained within normal limits for both groups throughout the observation period, with significant differences noted at three minutes (p=0.0007), five minutes (p<0.001), 10 minutes (p<0.001), 15 minutes (p<0.001), 45 minutes (p=0.0024), and 60 minutes (p<0.001) [Table/Fig-6].
Comparison of SPO2 at various intervals post-anaesthesia.
| Time interval | SpO2 | p-value |
|---|
Group 1
(Mean±SD) | Group 2
(Mean±SD) |
|---|
| 0 min | 99.45±0.68 | 99.45±0.68 | 1 |
| 3 min | 99.05±0.22 | 99.45±0.68 | 0.0007 |
| 5 min | 99.85±0.36 | 99.00±0.00 | <0.001 |
| 10 min | 99.95±0.22 | 99.00±0.00 | <0.001 |
| 15 min | 99.03±0.16 | 99.47±0.51 | <0.001 |
| 30 min | 99.15±0.36 | 96.47±15.65 | 0.2833 |
| 45 min | 99.72±0.45 | 99.38±0.54 | 0.0024 |
| 60 min | 99.95±0.22 | 98.90±0.67 | <0.001 |
| 90 min | 99.03±0.16 | 99.00±0.00 | 0.3204 |
| 120 min | 99.00±0.00 | 99.00±0.00 | 1 |
The onset of sensory blockade was significantly faster in Group 2 (13.00±1.89 minutes) compared to Group 1 (14.38±2.19 minutes) (p=0.0036). There was no significant difference in the onset of motor blockade between Group 1 (16.20±2.14 minutes) and Group 2 (15.70±1.99 minutes) (p=0.2824). The duration of sensory block was significantly longer in Group 2 (971.00±84.76 minutes) than in Group 1 (694.38±28.08 minutes) (p<0.001). Similarly, the duration of motor block was prolonged in Group 2 (918.75±65.80 minutes) compared to Group 1 (632.60±23.09 minutes) (p<0.001) [Table/Fig-7].
Comparison of onset and duration of sensory and motor blocks and duration of post-op analgesia.
| Parameters | Group 1
(Mean±SD) | Group 2
(Mean±SD) | p-value |
|---|
| Onset of sensory block | 14.38±2.19 | 13.00±1.89 | 0.0036 |
| Duration of sensory block | 694.38±28.08 | 971.00±84.76 | <0.001 |
| Onset of motor block | 16.20±2.14 | 15.70±1.99 | 0.2824 |
| Duration of motor block | 632.60±23.09 | 918.75±65.80 | <0.001 |
| Duration of post-op analgesia | 811.12±17.23 | 1051.00±90.18 | <0.001 |
| Time of first rescue analgesia | 826.50±13.92 | 1116.75±93.96 | <0.001 |
The duration of postoperative analgesia was significantly extended in Group 2 (1051.00±90.18 minutes) compared to Group 1 (811.12±17.23 minutes) (p<0.001). The time to the first rescue analgesia was also significantly longer in Group 2 (1116.75±93.96 minutes) than in Group 1 (826.50±13.92 minutes) (p<0.001) [Table/Fig-7]. VAS scores were comparable between the groups during the initial postoperative hours; however, at the 10-hour mark, Group 2 reported significantly lower VAS scores (p=0.0241) [Table/Fig-8].
Comparison of VAS scores at various time intervals.
| Time interval | VAS score | p-value |
|---|
Group 1
(Mean±SD) | Group 2
(Mean±SD) |
|---|
| 30 min | 0.00±0.00 | 0.00±0.00 | 1 |
| 1 h | 0.00±0.00 | 0.00±0.00 | 1 |
| 3 h | 0.00±0.00 | 0.00±0.00 | 1 |
| 5 h | 0.00±0.00 | 0.00±0.00 | 1 |
| 7 h | 0.00±0.00 | 0.00±0.00 | 1 |
| 10 h | 2.25±0.63 | 1.77±1.14 | 0.0241 |
No significant complications or adverse effects were noted in either group throughout the study period.
Discussion
The key findings of the present study indicate that dexamethasone, when used as a perineural adjuvant in supraclavicular brachial plexus block, significantly prolongs the duration of sensory and motor blockade compared to dexmedetomidine. Patients in the dexamethasone group experienced extended postoperative analgesia and a delayed need for the first rescue analgesia. Both dexamethasone and dexmedetomidine provided effective pain control in the initial postoperative period; however, dexamethasone demonstrated superior long-term analgesic effects.
Regarding the onset of sensory block, present study found that dexamethasone resulted in a faster onset (13.00±1.89 minutes) compared to dexmedetomidine (14.38±2.19 minutes), which was statistically significant (p=0.0036). This finding aligns with multiple studies, including Baloda R et al., who observed a reduced onset time for sensory block when dexamethasone was added to levobupivacaine (mean 8.17 minutes vs. 10.20 minutes; p<0.001) [17]. Similarly, Shrestha BR et al., confirmed a faster sensory block onset with dexamethasone [18]. The faster onset with dexamethasone may be attributed to its anti-inflammatory properties, which enhance nerve block effectiveness and its potential to decrease local anaesthetic absorption through vasoconstriction.
In terms of the duration of sensory block, dexamethasone significantly prolonged the duration (971.00±84.76 minutes) compared to dexmedetomidine (694.38±28.08 minutes) (p<0.001). Movafegh A et al., and Sehmbi H et al., found similar results, demonstrating a prolonged sensory block duration with the addition of dexamethasone [19,20]. This is consistent with Baloda R et al.’s findings (mean 923 minutes vs. 657.5 minutes; p<0.0001) [17]. The extended duration can be explained by dexamethasone’s ability to reduce perineural inflammation and inhibit nociceptive signal transmission.
For the onset of motor block, although the difference was not statistically significant in the present study (p=0.2824), dexamethasone showed a slightly faster onset (15.70±1.99 minutes) compared to dexmedetomidine (16.20±2.14 minutes). Biradar PA et al., reported a faster motor block onset with dexamethasone, supporting its efficacy in expediting motor block onset [21].
The duration of motor block was significantly longer with dexamethasone (918.75±65.80 minutes) than with dexmedetomidine (632.60±23.09 minutes) (p<0.001). This finding is corroborated by studies like Islam S et al., (2011) [22], which demonstrated a significantly prolonged motor block with dexamethasone, aligning with Baloda R et al., observations (mean 798.83 minutes vs. 540 minutes; p<0.001) [17]. Dexamethasone’s modulation of potassium channels and suppression of ectopic neuronal discharge contribute to this prolonged effect.
Regarding postoperative analgesia, dexamethasone provided a longer duration (1051.00±90.18 minutes) compared to dexmedetomidine (811.12±17.23 minutes) (p<0.001). Tandoc MN et al., observed a prolonged analgesia duration with dexamethasone, indicating its effectiveness in enhancing postoperative pain management [23]. The extended time to first rescue analgesia in the dexamethasone group mirrors these findings, suggesting sustained analgesic effects.
The VAS scores were significantly lower at the 10-hour mark in the dexamethasone group, indicating better long-term pain control. Shrestha BR et al., [18] found lower postoperative VAS scores with dexamethasone, supporting the results of present study as well as those of Baloda R et al., [17].
In terms of haemodynamic parameters, patients in the dexmedetomidine group experienced more fluctuations, including hypotension and bradycardia, likely due to dexmedetomidine’s sympatholytic properties as an alpha-2 adrenergic agonist. Dexamethasone did not significantly affect heart rate or blood pressure, providing a more stable haemodynamic profile. Studies by Choi S et al., and Persec J et al., found no significant changes in heart rate or blood pressure with dexamethasone, which aligns with present findings [3,24].
The SpO2 levels remained within normal limits and were comparable between the two groups throughout the study. This is consistent with the reports by Baloda R et al., and Sehmbi H et al., who found no significant changes in SpO2 levels with either adjuvant [17,20].
Limitation(s)
This is a single-centre study, and the participants belonged to the same ethnic background. A multi-centre study that includes various ethnic groups may improve the quality of the research.
Conclusion(s)
The present prospective randomised study compared the efficacy of perineural dexamethasone and perineural dexmedetomidine in supraclavicular blocks for upper limb orthopaedic surgeries. The results demonstrated that perineural dexamethasone provided longer-lasting analgesia compared to perineural dexmedetomidine. Additionally, patients in the dexamethasone group reported reduced pain scores and decreased opioid consumption for postoperative analgesia. Notably, no significant differences were observed in motor block onset or adverse effects between the two groups. Overall, the study concluded that perineural dexamethasone offers superior postoperative analgesia, prolonging pain relief by 3.7 hours and reducing opioid requirements. Therefore, for upper limb orthopaedic surgeries, perineural dexamethasone in supraclavicular blocks is recommended for its enhanced analgesic benefits.