The techniques of spinal anaesthesia for below-umbilical surgeries offer a faster onset, effective sensory and motor blockade and prolonged postoperative analgesia in lower limb procedures [1]. These techniques have several advantages over balanced anaesthesia, including a reduced stress response to surgery, decreased incidence of nausea and vomiting and less cardiorespiratory depression [2].
Ropivacaine is gaining popularity due to its reduced risk of cardiotoxicity and central nervous system toxicity [3]. It provides less motor blockade with greater sensory-motor differentiation compared to other local anaesthetics [4]. Hyperbaric ropivacaine, prepared by adding 5-8% dextrose to an isobaric solution of ropivacaine, has recently been introduced as a commercial formulation. This hyperbaric preparation offers a shorter time for mobilisation and micturition, along with a lower incidence of hypotension, especially in geriatric patients with cardiac pathology [5].
Levobupivacaine, the pure S-enantiomer of bupivacaine, is a safer alternative for regional anaesthesia than racemic bupivacaine. Pharmacodynamic studies have shown that it has less affinity for and weaker depressant effects on myocardial and central nervous system vital centers. Additionally, levobupivacaine demonstrates a superior pharmacokinetic profile [6,7].
The earlier commercial preparation of 0.75% ropivacaine was not available and it was not possible to make a 7.5 mg/mL formulation by adding dextrose; hence, more studies are needed to obtain efficacy for this dosage. Thus, this study aimed to compare the sensory and motor blockade, the time of two-segment regression for rescue analgesia, haemodynamic effects and sedative effects between hyperbaric 0.5% levobupivacaine and hyperbaric 0.75% ropivacaine.
Materials and Methods
This prospective, double-blinded, randomised clinical study was conducted in the Department of Anaesthesiology, Shrimati Bhikhiben Kanjibhai Shah Medical Institute and Research Centre (a tertiary care institute), Sumandeep Vidyapeeth Deemed to be University, Piparia, Vadodara, Gujarat, India, from September 2023 to July 2024, after obtaining approval from the Institutional Ethical Committee (SVIEC/UN/MEDI/SRP/SEP/23/22).
Inclusion and Exclusion criteria: A total of 40 patients of either gender, aged 18 to 65 years, belonging to ASA I and II, who were scheduled for elective infraumbilical surgeries and undergoing neuraxial block were included in the present study. Patients with systemic diseases such as cardiovascular disease, hepatic disease, renal disease, anaemia, or shock, as well as those with coagulation profile disorders or who were on treatment and patients with local infections at the puncture site for spinal anaesthesia, spine deformities, or known allergies to the drug were excluded from the present study.
Sample size calculation: To identify the difference in postoperative analgesia duration between the two groups, a minimum sample size of 20 per group was needed, with a 95% confidence level and an 80% power of analysis [8].
Study Procedure
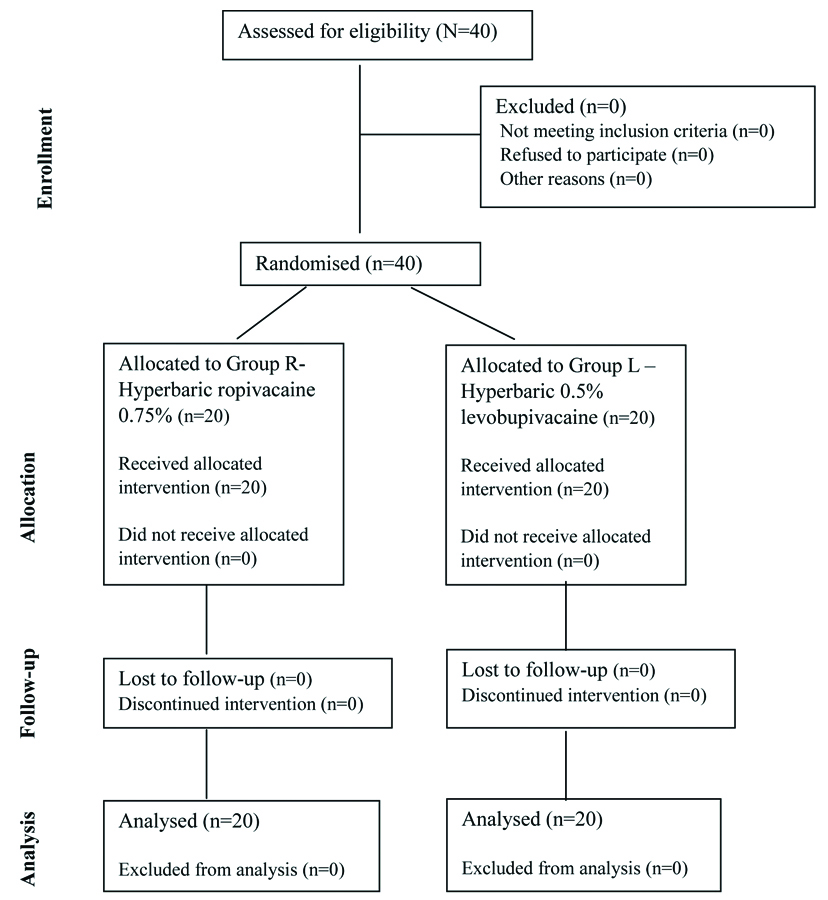
A detailed preanaesthetic history was taken one day prior to surgery. All routine investigations were completed. The procedure was explained and written informed consent was obtained in the participant’s native language. The patients were divided into two equal groups: R (Ropivacaine group) and L (Levobupivacaine group) for infraumbilical surgeries under spinal anaesthesia [Table/Fig-1]. Patients were randomised using the chit method, where a random chit labelled either R or L was picked and the patient was assigned to the study group accordingly. This is a double-blinded study where both the patients and the investigator were blinded.
Consolidated Standards of Reporting Trials (CONSORT) flowchart.
Upon arrival at the operating theatre, crystalloid inj. Ringer’s lactate was started at 10 mL/kg using Holiday Segar’s formula [9]. Baseline parameters such as Heart Rate (HR), Systolic and Diastolic Blood Pressure (SBP, DBP) and arterial SpO2 were recorded. Patients were premedicated with inj. glycopyrrolate 0.2 mg, inj. pantoprazole 40 mg and inj. ondansetron 4 mg intravenously. With patients in the sitting position, painting and draping of the patient’s back were performed with povidone-iodine solution. The identification of the level using the intercrestal line (Tuffier’s line), which passes through the L4-L5 intervertebral space, was conducted. A 23-gauge spinal needle was inserted through the midline at the L3-L4 interspace. The study drug was administered by a consultant anaesthesiologists not involved in the study.
Patients in Group R received 0.75% hyperbaric ropivacaine (3.5 mL)+0.1 mL 0.9% normal saline (total 3.6 mL) and Group L received 0.5% hyperbaric levobupivacaine (3.5 mL)+0.1 mL 0.9% normal saline (total 3.6 mL). After a clear free flow of cerebrospinal fluid, the study drug was injected over 10-20 seconds. Patients were then placed supine immediately after injection. The parameters monitored were HR, blood pressure (SBP, DBP) and arterial SpO2.
Sensory block was assessed using a 3-point pinprick scale [10]. The onset of sensory block was defined as the time between intrathecal injection and the loss of pinprick sensation at the L1 level [10]. The duration of sensory block was the time from intrathecal drug administration to the complete resolution of anaesthesia [10].
Motor blockade was assessed using the Bromage scale [7]. The motor block onset time was defined as the interval between intrathecal injection and achieving a grade 3 motor block [7]. The length of motor block was noted as the time between intrathecal injection and achieving a grade 0 motor block [7].
The sedative effect was assessed using the Ramsay sedation scale [11], where the time of onset of sedation was considered when the score reached 3. The duration of sedation was counted from the time the score returned to 2.
Postoperatively, pain scores were assessed using Prince Henry’s visual rating scale [12], where Grade 0 indicated no pain on cough; Grade 1 indicated pain on cough but not on deep breathing; Grade 2 indicated pain on deep breathing but not at rest; Grade 3 indicated slight pain at rest; and Grade 4 indicated severe pain at rest. The Visual Rating Scale (VRS) was assessed every 30 minutes postoperatively for up to six hours. Rescue analgesia was provided as inj. diclofenac 75 mg intravenously if the VRS was greater than or equal to 3 [12].
All parameters were monitored intraoperatively at 0, 5, 10, 15, 20, 30 and 45 minutes and then every 30 minutes until the completion of the surgery. If hypotension was observed, 6 mg of intravenous mephentermine was administered. In the case of bradycardia, 0.6 mg of intravenous atropine was given.
Statistical Analysis
The data were collected and tabulated. With a 95% confidence level and 80% power of analysis, means and Standard Deviations (SD) were presented as numerical variables, while categorical variables were presented as frequencies and percentages. For numerical variables, the unpaired Student’s t-test was used for between-group comparisons and for categorical variables, the Chi-square test was employed. A p-value of <0.05 was considered statistically significant.
Results
Both Groups R and L were demographically comparable in terms of age, gender, weight, ASA grading and duration of surgery [Table/Fig-2]. As depicted in [Table/Fig-3], it was observed that following spinal anaesthesia, HRs were comparable and stable in both groups. There were a few cases in which, during the first 20 minutes, a lesser drop in HR was observed with hyperbaric ropivacaine compared to hyperbaric levobupivacaine. In [Table/Fig-4,5 and 6], there was a smaller decrease in SBP with hyperbaric ropivacaine compared to hyperbaric levobupivacaine. The decrease in SBP and DBP was less than 20% in Group L; therefore, inj. mephentermine 6 mg i.v. and inj. atropine 0.6 mg i.v. were not administered. This indicates that hyperbaric ropivacaine was more haemodynamically stable than hyperbaric levobupivacaine. Mean Arterial Pressure (MAP) was maintained in both groups, with a higher mean arterial pressure observed in Group R, which was statistically significant (p<0.05). Arterial SpO2 and respiratory rates remained within normal limits and were comparable between the two groups (p>0.05) both intraoperatively and postoperatively. No adverse effects, such as shivering, nausea, or vomiting, were observed in either group.
Demographic parameters of both the groups.
| Parameters | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| Age (years) | 45.00±7.1 | 51.95±8.03 | 0.078 (NS) |
| Weight (kg) | 61.50±8.26 | 62.5±7.11 | 0.6286 (NS) |
| Gender |
| Male | 18 (90%) | 18 (90%) | 0.8618 (NS) |
| Female | 2 (10%) | 2 (10%) |
| ASA n (%) |
| I | 8 (40%) | 6 (30%) | 0.7911 (NS) |
| II | 12 (60%) | 14 (70%) |
| Duration of surgery (mins) | 87±49.63 | 88±34.08 | 0.91(NS) |
*NS: Not significant
Comparison of HR (beats per minute) in Group-R and Group-L.
| Time (Minutes) | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| 0 | 88.10±12.82 | 79.30±11.39 | 0.02 (S) |
| 2 | 90.50±13.84 | 79.95±12.40 | 0.01 (S) |
| 5 | 92.00±14.13 | 79.70±11.49 | 0.004 (S) |
| 10 | 91.00±11.40 | 82.40±11.20 | 0.02 (S) |
| 20 | 87.60±15.28 | 80.00±11.53 | 0.08 (S) |
| 30 | 83.79±13.95 | 78.40±10.77 | 0.18 (NS) |
| 45 | 86.38±15.04 | 78.30±10.10 | 0.06 (NS) |
| 60 | 87.08±19.02 | 79.11±11.17 | 0.15 (NS) |
| 75 | 88.40±14.45 | 77.64±11.96 | 0.07 (NS) |
| 90 | 85.80±13.58 | 77.45±11.28 | 0.14 (NS) |
| 105 | 84.80±10.88 | 84.80±10.88 | 1 (NS) |
| 120 | 87.60±16.86 | 76.75±14.73 | 0.17 (NS) |
| 135 | 86.00±17.61 | 75.00±8.25 | 0.2 (NS) |
| 150 | 86.86±10.88 | 81.00±7.07 | 0.5 (NS) |
Comparison of SBP (mmHg) in Group-R and Group-L.
| Time (Minutes) | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| 0 | 125.30±15.30 | 120.80±8.06 | 0.25 (NS) |
| 2 | 124.40±12.94 | 116.70±8.59 | 0.03 (S) |
| 5 | 122.50±13.70 | 114.20±9.92 | 0.03 (S) |
| 10 | 118.90±13.03 | 112.60±8.51 | 0.07 (NS) |
| 20 | 119.30±15.24 | 111.70±10.09 | 0.07 (NS) |
| 30 | 121.58±15.25 | 110.30±8.47 | 0.006 (S) |
| 45 | 122.63±14.02 | 108.70±7.20 | 0.0005 (S) |
| 60 | 120.77±17.79 | 109.00±8.04 | 0.018 (S) |
| 75 | 121.40±12.04 | 110.73±9.69 | 0.03 (S) |
| 90 | 125.00±10.34 | 112.36±10.54 | 0.01 (S) |
| 105 | 127.00±11.17 | 110.50±10.07 | 0.005 (S) |
| 120 | 129.80±12.13 | 110.00±9.20 | 0.001 (S) |
| 135 | 124.89±14.77 | 115.00±12.73 | 0.4 (NS) |
| 150 | 125.14±18.22 | 110.00±10.2 | 0.2 (NS) |
Comparison of DBP (mmHg) in Group-R and Group-L.
| Time (Minutes) | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| 0 | 82.80±13.60 | 75.40±7.20 | 0.03 (S) |
| 2 | 81.40±12.48 | 73.60±5.45 | 0.01 (S) |
| 5 | 79.90±11.53 | 74.20±7.05 | 0.06 (NS) |
| 10 | 76.20±13.64 | 74.40±7.10 | 0.63 (NS) |
| 20 | 77.70±13.49 | 75.85±6.76 | 0.58 (NS) |
| 30 | 78.42±12.95 | 75.75±5.99 | 0.42 (NS) |
| 45 | 80.13±13.48 | 74.90±6.44 | 0.13 (NS) |
| 60 | 80.77±13.60 | 74.44±6.71 | 0.05 (S) |
| 75 | 82.60±16.14 | 74.55±4.57 | 0.12 (NS) |
| 90 | 86.20±12.09 | 75.45±6.14 | 0.01 (S) |
| 105 | 88.40±13.49 | 74.25±1.04 | 0.01 (S) |
| 120 | 87.40±14.11 | 76.00±1.51 | 0.03 (S) |
| 135 | 85.78±14.16 | 74.00±5.66 | 0.29 (NS) |
| 150 | 81.43±19.69 | 76.00±5.14 | 0.72 (NS) |
Comparison of MAP (mmHg) in Group-R and Group-L.
| Time | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| 0 | 97±14.17 | 90±7.73 | 0.05 (S) |
| 2 | 96±12.63 | 88±6.83 | 0.01 (S) |
| 5 | 93±12.25 | 88±8.34 | 0.1 (NS) |
| 10 | 90±13.44 | 87±7.90 | 0.3 (NS) |
| 20 | 91±14.07 | 88±8.20 | 0.4 (NS) |
| 30 | 92±13.72 | 87±7.15 | 0.1 (NS) |
| 45 | 94±13.66 | 86±6.96 | 0.02 (S) |
| 60 | 94±15.00 | 86±7.49 | 0.03 (S) |
| 75 | 95±14.77 | 87±7.11 | 0.03 (S) |
| 90 | 99±11.51 | 88±8.27 | 0.001 (S) |
| 105 | 101±12.72 | 86±5.38 | 0.001 (S) |
| 120 | 102±13.45 | 87±4.74 | 0.001 (S) |
| 135 | 99±14.36 | 87±9.35 | 0.003 (S) |
| 150 | 96±19.20 | 87±7.83 | 0.05 (S) |
The onset of sensory blockade at the T10 level, motor blockade and time to rescue analgesia in Group R were slower than in Group L, with p<0.05. The time to two-segment regression in Group R was comparable to Group L, with p>0.05. The duration of sensory blockade, motor blockade and time for rescue analgesia were significantly prolonged in Group L compared to Group R, with p<0.05. No sedative effects were observed in either group [Table/Fig-7].
Comparison of sensory and motor block characteristics between Group-R and Group-L.
| Characteristics | Group-R Mean±SD | Group-L Mean±SD | p-value |
|---|
| Onset of sensory block at T10* | 7.3±3.5 | 4.2±1.4 | 0.012 (S) |
| Onset of motor block* | 5.84±3.16 | 2.2±0.8 | 0.001 (S) |
| Time of two segment regression | 87.35±15.02 | 79.50±13.76 | 0.06 (NS) |
| Duration of sensory block* | 214.60±27.47 | 260.50±40.19 | 0.0001 (S) |
| Duration of motor block* | 197.70±20.46 | 241.5±38.01 | 0.0001 (S) |
| Time to rescue analgesia* | 183.0±25.77 | 241.00±24.47 | 0.0001 (S) |
| Ramsay sedation score at all times | 2 | 2 | NA |
*p<0.05 - Significant (S)
In Group R, a VRS of 3 was achieved in 50% of patients at two hours and 30 minutes and in 35% at three hours. In Group L, 50% achieved a VRS of 3 at four hours and 40% at four hours and 30 minutes. These differences were statistically significant (p=0.001) [Table/Fig-8].
Time duration when patient’s VRS score returned to 3 postoperatively.
| Time (hours) | Group-R
n (%) | Group-L
n (%) |
|---|
| 1 | 0 | 0 |
| 1.5 | 0 | 0 |
| 2 | 2 (10%) | 0 |
| 2.5 | 10 (50%) | 0 |
| 3 | 7 (35%) | 1 (5%) |
| 3.5 | 0 | 1 (5%) |
| 4 | 1 (5%) | 10 (50%) |
| 4.5 | 0 | 8 (40%) |
Various types of surgeries were included in the study; consequently, varying times for rescue analgesia were observed in patients. This variability was due to the different levels of incision in each surgery, which influenced the time to rescue analgesia [Table/Fig-9].
Details of types of surgeries and their mean time for rescue analgesia.
| S. No. | Types of surgeries | n (%) | Mean time for rescue analgesia (Minutes) Mean±SD |
|---|
| 1 | Haemorrhoidectomy | 5 (12.5%) | 250±20.2 |
| 2 | Anal fistulectomy | 5 (12.5%) | 178±18.5 |
| 3 | Inguinal hernioplasty | 4 (10%) | 227.5±20.8 |
| 4 | Urological surgeries | 5 (12.5%) | 237.5±25.1 |
| 5 | Debridement | 9 (22.5%) | 236.6±28.4 |
| 6 | Knee surgeries | 2 (5%) | 210±19.6 |
| 7 | Tibia and femur surgeries | 10 (25%) | 190±17.8 |
Discussion
The research indicated a higher quality of analgesia as well as prolonged sensory and motor block with the efficacy of spinal anaesthesia in the present study using 0.5% hyperbaric levobupivacaine. However, there was a decrease in HR and blood pressure with 0.5% hyperbaric levobupivacaine compared to 0.75% ropivacaine. The sedative effect and duration of analgesia were comparable in both groups. No side-effects, such as shivering, nausea, or vomiting, were reported.
The present study suggests that ropivacaine can be used for shorter duration procedures like fistulectomy, haemorrhoidectomy and urological procedures such as stent removal, where postoperative pain is generally less compared to larger incision surgeries like lower limb tibia and femur surgeries. The latter procedures are not only longer in duration but also associated with greater pain due to increased surgical manipulation; therefore, in such cases, levobupivacaine may provide a superior blockade.
In the present study, the demographics were comparable, which was also observed in the studies conducted by Sanansilp V et al., and Singh G et al., [13,14]. Haemodynamic changes such as HR, mean SBP and mean DBP were more stable in Group-R compared to Group-L. There was less hypotension and bradycardia observed with hyperbaric ropivacaine compared to hyperbaric levobupivacaine. This indicates that haemodynamics were more stable in Group-R with higher levels of blocks. SpO2 and respiratory rate were comparable and insignificant in both groups (p>0.05). This was also observed in the study conducted by Ghimire R and Gyawali M which stated that hyperbaric ropivacaine (3 mL, 0.5%) had a shorter duration and better haemodynamics than hyperbaric bupivacaine (3 mL, 0.5%) when administered intrathecally [15].
The onset of sensory blockade at the T10 level and motor blockade in Group-R was slower than in Group-L, with p<0.05. This was also observed in the study conducted by Sanansilp V et al., where the onset of sensory blockade with hyperbaric 0.5% levobupivacaine was 2.2 minutes and the onset of motor blockade was 2.9 minutes [13]. This contrasts with the study conducted by Singh G et al., where the onset of sensory and motor blockade in Group-R and Group-L was much slower than in the present study [14]. This difference is likely due to the lower concentration of the hyperbaric drug used and the manual addition of dextrose rather than using the newer preparation.
The time to two-segment regression was slower in Group-R than in Group-L, with p>0.05. This difference is not statistically significant. The study conducted by Singh G et al., also reported similar results for the time of two-segment regression in Group-R and Group-L [14]. In the present study, the duration of sensory blockade, motor blockade and time for rescue analgesia was significantly prolonged in Group-L compared to Group-R, with p<0.05. The sedative effects were comparable in both groups. In the study by Singh G et al., the duration of sensory and motor blockade and time for rescue analgesia was comparatively much shorter than in the present study, probably due to the superior stability of the drug mixture used in the present study and the higher concentration of hyperbaric solution [14]. According to older literature, 1.5 times the amount of ropivacaine is required to produce the same effect as levobupivacaine, which can also be observed from the values in the present study. The use of a 1 to 1.5 equipotency ratio between levobupivacaine and ropivacaine or bupivacaine resulted, nevertheless, in a shorter duration of spinal anaesthesia, even if this was not associated with a shorter home discharge time [16].
Kalbande JV et al., conducted a study to compare hyperbaric ropivacaine and hyperbaric bupivacaine and concluded that 0.75% hyperbaric ropivacaine, when intrathecally administered at 22.5 mg, provided clinically effective anaesthesia for elective infraumbilical surgeries [17]. Comparative analysis reveals that at an equipotent dose, this local anaesthetic matches hyperbaric bupivacaine in several critical parameters, including sensory blockade duration, blockade height consistency and haemodynamic stability. Moreover, it offers the distinct advantage of a shorter motor blockade duration while maintaining adequate postoperative analgesia, positioning ropivacaine as a promising alternative in regional anaesthetic protocols for lower abdominal surgical interventions.
The study conducted by Kumar M et al., also suggests that levobupivacaine provides a similar neuraxial blockade to bupivacaine but with fewer side-effects [18]. Yăgana O et al., compared different densities of hyperbaric levobupivacaine in arthroscopic knee surgeries and suggested that with an increase in density, the sensory and motor block duration was lengthened [19]. Kulkarni KR et al., compared hyperbaric ropivacaine with hyperbaric bupivacaine and concluded that ropivacaine demonstrated distinct anaesthetic characteristics compared to bupivacaine [20]. The ropivacaine group exhibited a slower sensory block onset (4.5 minutes versus 3.2 minutes) and a shorter total sensory block duration (155 minutes versus 190.5 minutes). Notably, patients receiving ropivacaine experienced significantly more rapid motor block recovery (120 minutes compared to 190 minutes) and achieved urinary catheterisation faster (257 minutes versus 358 minutes). These statistically significant differences (p<0.05) suggest that ropivacaine offers potential advantages in terms of reduced blockade duration and quicker patient recovery, potentially enhancing postsurgical patient comfort and mobility. Similar results were observed in the present study with hyperbaric ropivacaine.
Hyperbaric ropivacaine is an excellent agent of choice for patients with cardiac pathology and provides better haemodynamic stability when compared to hyperbaric levobupivacaine, although hyperbaric levobupivacaine provides superior sensory and motor blockade and better analgesia. Cappelleri G et al., concluded that doses as small as 7.5 mg of 0.5% ropivacaine heavy or 5 mg of 0.5% levobupivacaine heavy were adequate for short-lasting spinal anaesthesia for daycare knee arthroscopy, with faster home discharge compared to 7.5 mg of 0.5% levobupivacaine heavy [21].
Gohil PJ et al., conducted a study that showed hyperbaric ropivacaine at a 0.75% concentration was evaluated as a potential equivalent alternative to hyperbaric bupivacaine at 0.5% for patients requiring lower limb orthopaedic surgical procedures [22]. The study found that the two local anaesthetics demonstrated comparable efficacy, suggesting that ropivacaine could provide surgeons and anaesthesiologistss with a reliable alternative to traditional bupivacaine formulations when performing orthopaedic interventions on the lower extremities, with more haemodynamic stability, which was also observed in the present study. A total of 25% of cases in the present study were lower limb orthopaedic surgeries.
The present study includes various different surgeries to understand how the study drug works in different procedures, which is also a limitation, as varying incision levels provide varying durations of analgesia. However, since it is a novel study, it can guide researchers on the various procedures that can be conducted using these drugs. More extensive research can be conducted using the present study as a small guide.
Limitation(s)
The present study is a short research study, as it was conducted over a period of six months. Future studies with larger sample sizes will be required for a better understanding of both groups. The present study included various types of surgeries, which resulted in different levels of incision and varying times for rescue analgesia in the patients.
Conclusion(s)
A 0.5% hyperbaric levobupivacaine used in infra-umbilical surgeries is more efficient in terms of the onset and duration of sensory and motor blockade, time for two-segment regression and time for rescue analgesia compared to 0.75% hyperbaric ropivacaine. This study implies that in haemodynamically unstable patients, 0.75% hyperbaric ropivacaine can provide a less complicated neuraxial blockade with an equally dense block, while levobupivacaine offers a superior effect in terms of the duration of blockade and analgesia. This makes levobupivacaine useful for longer-duration surgeries, while ropivacaine is suitable for shorter-duration procedures.
*NS: Not significant
*p<0.05 - Significant (S)