Neuraxial blockade is the preferred mode of anaesthesia for lower limb orthopaedic surgeries. It offers a rapid onset, superior analgesia, a lower failure rate and is cost-effective. It provides greater pain relief compared to intravenous (i.v.) or epidural routes [1]. The use of intrathecal adjuvants has become popular in helping to prolong postoperative analgesia, improve patient satisfaction and promote fast recovery. Neuraxial opioids, though effective, are associated with undesirable side-effects, like delayed respiratory depression, nausea, vomiting, urinary retention and pruritus, that limit their use in the ward [2].
The hypnotic effects of benzodiazepines are mediated by alterations in potential-dependent calcium ion flux [3,4]. They also exhibits a muscle relaxant effect via its action on the glycine receptors in the spinal cord [5]. Magnesium sulphate is a pharmacological agent used in various clinical conditions, such as tachyarrhythmia, myocardial and neuronal ischaemia, asthma, and seizures in preeclampsia [6]. Midazolam, a benzodiazepine, is used primarily for anxiolysis, amnesia, and sedation [7]. Magnesium also potentiates opioid nociception and prolongs the duration of anaesthesia [7]. The analgesic properties of magnesium sulphate are primarily related to the regulation of calcium influx into cells [8] and antagonism of NMDA receptors [9].
Currently, researchers have focused on non opioid drugs that potentiate bupivacaine’s analgesic effects [10-12]. The present study aimed to address the research gap on alternative intrathecal adjuvants, specifically exploring the potential of midazolam and magnesium sulphate beyond their routine i.v. administration. The present study hypothesised that intrathecal midazolam and magnesium sulphate, as adjuncts to hyperbaric bupivacaine, might be useful in maintaining haemodynamic stability during spinal anaesthesia in tibia-fibula fracture surgeries. This combination may hasten the onset of spinal block, prolong the duration of anaesthesia, improve postoperative analgesia, and provide haemodynamic stability.
Materials and Methods
The present double-blinded (patient and investigator were blinded) prospective, randomised clinical study was conducted in the Department of Anaesthesiology at Dhiraj Hospital, Sumandeep Vidyapeeth, Piparia, Vadodara, Gujarat, India, from February 2021 to December 2022. Study was conducted following Institutional Ethical Committee approval (SVIEC/ON/Medi/BNPG20/D21031).
Inclusion criteria: Patients who were willing to sign the informed written consent, undergoing elective and emergency infraumbilical surgeries, classified as ASA grade I and II, of either gender, and aged 18-65 years were included in the study.
Exclusion criteria: Patients, who refused to participate, had a height of less than 152 cm, had systemic diseases (such as heart disease, liver disease, kidney disease, anaemia, shock, septicaemia, uncontrolled hypertension), coagulation disorders, or were on anticoagulant therapy. Additionally, patients with local infection at the site of the proposed puncture for spinal anaesthesia, spinal deformities, those who required a change of anaesthesia at any time during the surgery for any reason, or had a known allergy to the study drugs were also excluded from the study.
Sample size calculation: Sample size estimation was based on the duration of sensory block from a study conducted by Singh A et al., [13]. The duration of sensory block in their study was normally distributed with standard deviations of 26.4 minutes and 41.7 minutes in the magnesium sulphate and midazolam groups, respectively. The difference in mean duration between the groups was at least 15 minutes. Therefore, a sample size of 32 in each group was determined to be sufficient to reject the null hypothesis with a power of 95% and a 5% level of significance. Sample size and power were calculated using a sample size calculator.
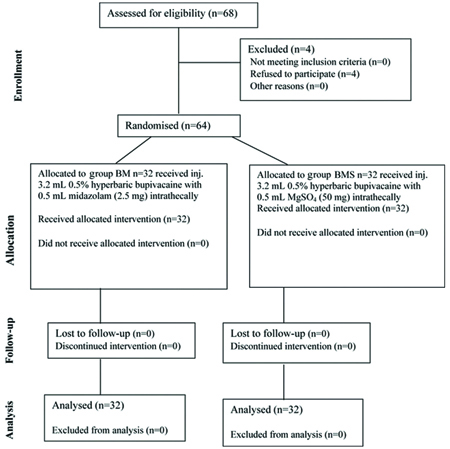
Sixty-four patients (both genders aged 18-65 years and of ASA grade I or II were divided into two equal groups: the BMS (magnesium sulphate group) and the BM (Midazolam group) for elective tibia-fibula surgeries under spinal anaesthesia [Table/Fig-1]. The drug was administered by a consultant anaesthesiologist who was not involved in the study.
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
Study Procedure
All patients fasted for eight hours. Patients’ informed and written consent were obtained from the patients for their agreement to accept the spinal neuraxial block. Upon arrival in the procedure room, an 18-gauge intravenous (i.v.) line was secured in the unaffected limb, and Ringer’s lactate was started as preloading at a rate of 10 mL/kg.
HR, continuous Electrocardiogram (ECG) monitoring, and non invasive measurements of SBP, DBP, mean arterial pressure MAP and SpO2 were recorded. All patients were premedicated as Institute protocol with inj. glycopyrrolate 0.2 mg and injection (inj.) ondansetron 4 mg. With the patient in a sitting position and under all aseptic and antiseptic precautions, a 25 G Quincke spinal needle was inserted in the midline at L3-4 interspace. After the free flow of clear Cerebrospinal Fluid (CSF), group BM (Midazolam group) received 0.5% hyperbaric bupivacaine 3.2 mL+2.5 mg preservative-free midazolam (0.5 mL), totaling 3.7 mL. Group BMS (magnesium sulphate group) received 0.5% hyperbaric bupivacaine 3.2 mL+50 mg magnesium sulphate (0.5 mL), also totalling 3.7 mL [14], administered over 0.2 mL per second by the consultant anaesthetist not involved in the study. Patients were placed in a supine position immediately after injection. Patients were randomised using the chit method, where a random chit labeled either R or RD was picked, and the patient was assigned to the study group accordingly. To reduce the bias, the study was double-blinded, meaning that both the patients and investigator were blinded.
Assessment of sensory blockade: Data were collected on the onset of sensory block, which was definedf as the time between the intrathecal injection and the loss of pinprick sensation at the L1 level. The duration of sensory block was measured from the intrathecal injection to the point at which there was a regression of two segments from maximally attained level.
Assessment of motor blockade by modified Bromage scale [15]:
Score 0: patient can move the hip, knee, and ankle;
Score 1: the patient is unable to move hip but able to move knee and ankle;
Score 2: the patient is unable to move hip and knee but can move ankle;
Score 3: the patient is unable to move hip, knee and ankle.
Motor block onset time was defined as the interval between the intrathecal injection and the achievement of a grade 3 motor block. The length of motor block was noted as the time between the intrathecal injection and the return to a grade 0 motor block [15].
Assessment of sedation by Ramsay sedation scale [16]: The time of onset of sedation was noted when the score reached three. The duration of sedation was considered when the score returned to two. If the sensory block was at or above the T10 dermatome level surgeon was allowed to start the surgery. Intraoperatively, sensory and motor blocks, HR, SBP, DBP, SpO2, RR and sedation were assessed at 0, 2, 5, 10, 20 and 30 minutes, and then each 15 minutes until the end of the surgery.
Postoperatively, all patients were shifted to the recovery room and monitored for HR, SBP, DBP, SpO2, RR, rescue analgesia time [17], and complete recovery from sensory and motor blockade. All vital signs were recorded every 30 minutes postoperatively until patients were able to flex their ankle. For rescue analgesia, inj. diclofenac sodium 75 mg was given i.v.
Statistical Analysis
The differences between the groups in the demographic data and baseline values were analysed using unpaired t-tests. The analysis was performed using IBM SPSS version 22.0 statistics for Windows software. Data are presented as mean±standard deviation. A p-value of <0.05 was considered statistically significant. Chi-square test was used for categorical variables (Weight and ASA grade). Student’s t-test was used for a continuous variable (age).
Results
Among the total of 64 patients, group BM (n=32) had mean±SD age of 37.63±11.50 years and group BMS had mean±SD age of 40.81±11.93 years. According to the demographic parameters and ASA grading, both groups, BM and BMS, were comparable to each other and were statistically non significant (p-value >0.05) [Table/Fig-2].
| Parameters | Group BM | Group BMS | p-value |
|---|
| n | Mean±SD | n | Mean±SD |
|---|
| Age (years) | 32 | 37.63±11.50 | 32 | 40.81±11.93 | 0.84 |
| Weight (kg) | 32 | 64.09±7.28 | 32 | 63.69±11.94 | 0.87 |
| ASA I, n (%) | 10 (31.25) | 8 (25) | 0.57 |
| ASA II, n (%) | 22 (68.75) | 24 (75) |
Pulse rates between both groups were comparable overall but were statistically significant (p-value <0.05) at two minutes [Table/Fig-3]. Mean SBP, mean DBP and MAP [Table/Fig-4,5 and 6] was compared and was statistically significant between both groups at two and ten minutes. Significant hypotension was observed in group BM at two and ten minutes, but MAP was maintained. SpO2 was comparable and non significant in both the groups (p-value >0.05) [Table/Fig-7].
Comparison of HR between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 94.63±14.68 | 90.63±9.63 | 0.19 |
| 2 min | 76.12±10.70 | 87.56±7.76 | 0.005* |
| 5 min | 90.50±11.62 | 89.88±7.99 | 0.80 |
| 10 min | 91.75±8.85 | 90.44±8.99 | 0.55 |
| 20 min | 92.75±6.81 | 91.25±8.07 | 0.42 |
| 30 min | 90.50±11.62 | 89.88±7.99 | 0.80 |
| 45 min | 90.13±8.20 | 93.06±7.68 | 0.14 |
| 60 min | 88.13±12.70 | 88.25±9.02 | 0.96 |
| 75 min | 83.63±10.51 | 88.88±10.76 | 0.05* |
| 90 min | 90.13±8.20 | 93.06±7.68 | 0.14 |
| 105 min | 94.63±14.68 | 90.63±9.63 | 0.19 |
| 120 min | 87.38±8.52 | 90.19±4.98 | 0.11 |
| 135 min | 84.88±11.58 | 87.00±6.52 | 0.36 |
| 150 min | 91.75±8.85 | 90.44±8.99 | 0.55 |
| 165 min | 83.63±10.51 | 88.88±10.76 | 0.05* |
| 180 min | 87.38±8.52 | 90.19±4.98 | 0.11 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
Comparison of SBP between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 124.6±12.02 | 126.3±9.75 | 0.55 |
| 2 min | 94.81±19.69 | 123.0±8.34 | 0.0001* |
| 5 min | 118.5±15.65 | 121.1±14.45 | 0.48 |
| 10 min | 106.0±14.91 | 117.3±12.20 | 0.0016* |
| 20 min | 117.9±9.24 | 121.9±9.705 | 0.09 |
| 30 min | 120.3±8.46 | 119.8±8.06 | 0.80 |
| 45 min | 120.8±10.16 | 122.9±10.11 | 0.40 |
| 60 min | 124.5±9.81 | 126.6±8.70 | 0.36 |
| 75 min | 127.0±8.40 | 124.8±6.56 | 0.25 |
| 90 min | 128.6±5.11 | 129.6±7.55 | 0.53 |
| 105 min | 128.6±5.11 | 129.8±4.67 | 0.36 |
| 120 min | 127.5±6.32 | 125.2±7.42 | 0.18 |
| 135 min | 130.3±6.84 | 133.0±3.25 | 0.044* |
| 150 min | 128.1±7.91 | 126.8±6.11 | 0.46 |
| 165 min | 126.6±6.49 | 126.4±5.53 | 0.90 |
| 180 min | 128.1±7.16 | 126.6±7.15 | 0.40 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
Comparison of DBP between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 85.13±6.96 | 85.44±3.67 | 0.82 |
| 2 min | 74.06±8.76 | 83.31±5.78 | <0.0001* |
| 5 min | 79.38±11.19 | 77.56±7.78 | 0.45 |
| 10 min | 72.88±7.36 | 77.13±4.62 | 0.0075* |
| 20 min | 78.75±7.42 | 81.31±7.54 | 0.17 |
| 30 min | 79.13±9.42 | 80.25±8.06 | 0.60 |
| 45 min | 75.88±9.78 | 79.88±6.64 | 0.06 |
| 60 min | 77.31±7.94 | 80.13±8.53 | 0.17 |
| 75 min | 76.50±6.07 | 77.69±6.50 | 0.45 |
| 90 min | 76.56±6.12 | 77.19±6.32 | 0.68 |
| 105 min | 77.56±7.17 | 79.19±6.15 | 0.33 |
| 120 min | 81.81±7.35 | 83.06±7.00 | 0.48 |
| 135 min | 81.06±9.01 | 81.94±6.71 | 0.66 |
| 150 min | 78.25±3.86 | 79.56±4.81 | 0.23 |
| 165 min | 79.56±5.51 | 81.19±4.68 | 0.20 |
| 180 min | 79.44±6.37 | 81.81±5.91 | 0.12 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
Comparison of MAP between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 98±8.34 | 99±8.56 | 0.6 |
| 2 min | 81±12.57 | 96±6.63 | 0.001* |
| 5 min | 92±12.48 | 92±9.99 | 0.7 |
| 10 min | 84±9.42 | 90±7.48 | 0.006* |
| 20 min | 92±7.82 | 95±8.30 | 0.14 |
| 30 min | 93±8.82 | 93±8.06 | 1 |
| 45 min | 91±10.03 | 94±7.80 | 0.1 |
| 60 min | 93±8.57 | 95±8.59 | 0.3 |
| 75 min | 93±6.83 | 93±6.52 | 1 |
| 90 min | 94±5.68 | 95±6.73 | 0.4 |
| 105 min | 94±6.42 | 96±5.66 | 0.1 |
| 120 min | 97±6.99 | 97±7.14 | 1 |
| 135 min | 98±7.95 | 99±5.23 | 0.5 |
| 150 min | 95±5.22 | 95±5.24 | 1 |
| 165 min | 95±5.84 | 96±4.96 | 0.4 |
| 180 min | 95±6.63 | 97±6.32 | 0.2 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
Comparison of SpO2 between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 99.19±0.39 | 99.22±0.42 | 0.34 |
| 2 min | 99.16±0.36 | 99.16±0.36 | >0.99 |
| 5 min | 99.34±0.65 | 99.50±0.67 | 0.34 |
| 10 min | 99.19±0.39 | 99.16±0.36 | 0.74 |
| 20 min | 99.13±0.33 | 99.16±0.36 | 0.72 |
| 30 min | 99.19±0.39 | 99.16±0.36 | 0.74 |
| 45 min | 99.16±0.36 | 99.09±0.29 | 0.45 |
| 60 min | 99.22±0.65 | 99.47±0.71 | 0.15 |
| 75 min | 99.13±0.33 | 99.13±0.33 | >0.99 |
| 90 min | 99.19±0.39 | 99.16±0.36 | 0.74 |
| 105 min | 99.38±0.65 | 99.53±0.62 | 0.33 |
| 120 min | 99.34±0.60 | 99.53±0.62 | 0.22 |
| 135 min | 99.16±0.36 | 99.16±0.36 | >0.99 |
| 150 min | 99.13±0.33 | 99.19±0.39 | 0.49 |
| 165 min | 99.13±0.33 | 99.13±0.33 | >0.99 |
| 180 min | 99.28±0.63 | 99.47±0.67 | 0.25 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
RR was comparable and non significant in both the groups (p-value ≥0.05) [Table/Fig-8].
Comparison of RR between the groups.
| Time | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| 0 min | 16.13±0.49 | 16.31±0.89 | 0.30 |
| 2 min | 16.38±0.94 | 16.31±0.89 | 0.78 |
| 5 min | 16.38±0.94 | 16.19±0.78 | 0.38 |
| 10 min | 16.44±0.98 | 16.88±1.43 | 0.15 |
| 20 min | 16.56±1.16 | 16.94±1.52 | 0.27 |
| 30 min | 16.38±0.94 | 16.81±1.42 | 0.1 5 |
| 45 min | 16.50±1.13 | 17.00±1.52 | 0.14 |
| 60 min | 16.38±0.94 | 16.81±1.42 | 0.15 |
| 75 min | 16.56±1.16 | 16.88±1.51 | 0.35 |
| 90 min | 16.50±1.01 | 16.88±1.43 | 0.23 |
| 105 min | 16.69±1.30 | 16.88±1.51 | 0.59 |
| 120 min | 16.56±1.16 | 17.00±1.43 | 0.18 |
| 135 min | 16.38±0.94 | 16.81±1.42 | 0.15 |
| 150 min | 16.56±1.04 | 16.94±1.52 | 0.25 |
| 165 min | 16.63±1.18 | 16.94±1.52 | 0.36 |
| 180 min | 16.38±0.94 | 16.81±1.42 | 0.15 |
Student’s t-test; *The p-value <0.05 was considered statistically significant
Comparison of secondary outcomes between group BM and group BMS were presented in [Table/Fig-9]. In terms of complications, bradycardia was noted in a 6 (18.75%) cases cases in group BM after administering spinal anaesthesia. In group BM, significant hypotension was noted in a 7 (21.87%) cases immediately after administering spinal anaesthesia [Table/Fig-10].
Comparison of secondary outcomes between group BM and group BMS.
| Parameters | Group BMMean±SD | Group BMSMean±SD | p-value |
|---|
| Onset of sensory blockade | 3.18±0.81 | 4.06±0.98 | 0.0002* |
| Onset of motor blockade | 4.89±0.96 | 7.57±1.02 | <0.0001* |
| Onset of sedation | 31.78±5.32 | 31.88±6.44 | 0.94 |
| Time of two segment regression | 159.4±17.36 | 142.0±19.95 | 0.0004* |
| Duration of sensory blockade | 248±25.71 | 226.9±24.65 | 0.0014* |
| Duration of motor blockade | 220.6±27.55 | 194.7±25.01 | 0.0002* |
| Duration of sedation | 87.03±15.23 | 82.19±13.38 | 0.18 |
| Time to rescue analgesia | 335.47±33.87 | 286.88±24.65 | 0.0001* |
Student’s t-test: *The p-value <0.05 was considered statistically significant
Complications observed in both the groups.
| Complications | Group BMn (%) | Group BMSn (%) | p-value |
|---|
| Nausea | 1 (3.12) | 1 (3.12) | 1.00 |
| Vomiting | 2 (6.25) | 2 (6.25) | 1.00 |
| Rigours | 0 | 0 | - |
| Bradycardia | 6 (18.75) | 1 (03.12) | 0.045* |
| Hypotension | 7 (21.87) | 1 (03.12) | 0.023* |
| Respiratory depression | 0 | 0 | - |
Chi-square test; *The p-value <0.05 was considered statistically significant
Discussion
The present study compared the haemodynamic and analgesic effects of intrathecal bupivacaine with midazolam (group BM) versus bupivacaine with magnesium sulphate (group BMS) during surgical procedures. In the present study, it was found that the difference in demographic variables was statistically insignificant between both groups (p-value >0.05), thus accepting null hypothesis, which is in accordance with studies conducted by Singh A et al., and Attia J et al., [13,18].
A sudden fall in SBP and DBP was seen immediately after giving spinal anaesthesia in group BM than to group BMS, with p-value <0.05. Singh A et al., and Attia J et al., studied intrathecal bupivacaine with adjuvants midazolam vs MgSO4 to a total volume of 3.5 mL [13,18]. There was no statistically significant difference in pulse rate and BP results, which were contradictory to the present study’s findings. Limbu PM et al., studied intrathecal 3 mL of bupivacaine with adjuvants MgSO4 vs normal saline [19]. Their study showed that intraoperative haemodynamics were similar between groups at different time intervals. Rana S et al., studied intrathecal 1.7 mL bupivacaine with adjuvants MgSO4 vs fentanyl on parturients undergoing elective caesarean sections, showing that both groups were haemodynamically stable in the postoperative period, comparable, and insignificant (p-value ≥0.05). RR was comparable and non significant in both the groups (p-value ≥0.05) [20].
The onset of sensory block was significantly shorter in group BM (3.18±0.81 minutes) compared to group BMS (4.06±0.98 minutes), with p-value <0.05. This coincided with the study of Attia J et al., where the onset in Group-A was 3.7±1.13 minutes and in Group-B was 6.6±2.7 minutes [18]. In the study conducted by Singh A et al., they found that the onset of sensory block was faster in Group-MG (1.31±0.61 minutes) than in Group-MZ (1.87±0.71 minutes) [13].
The onset of motor block was significantly faster in group BM (4.89±0.96 minutes) than in group BMS (7.57±1.02 minutes), with p <0.05. The results coincided with the study of Attia J et al., [18], where the onset in Group-A (with 2.5 mg midazolam) was 3.1±1.13 minutes and in Group-B (with 50 mg magnesium sulphate) was 6.0±2.7 minutes. In the study by Singh A et al., the onset was faster in Group-MG (1.94±1.12 minutes) than in Group-MZ (2.21±0.89 minutes), which did not coincide with the present study [13].
The time of onset of sedation (when the sedation score reached 3) and duration of sedation (when sedation score returned to 2) were comparable in both groups and were statistically insignificant (p-value >0.05). These findings were contradictory to those of Kim MH et al., who found no episodes of sedation in the control group (receiving 1 mL of 0.5% heavy bupivacaine plus 0.2 mL of 0.9% saline intrathecally), as well as, in group BM1 (receiving 1 mL of 0.5% heavy bupivacaine plus 0.2 mL of 0.5% preservative-free midazolam) and group BM2 (receiving 1 mL of 0.5% heavy bupivacaine plus 0.4 mL of 0.5% preservative-free midazolam) [21].
In a study conducted by Lee JW et al., they compared analgesia between two groups: Group-C (receiving 0.5% isobaric tetracaine 10 mg plus 0.5% saline intrathecally) and Group-M (receiving 0.5% isobaric tetracaine 10 mg plus 50 mg magnesium sulphate intrathecally). They concluded that intrathecal MgSO4 provided better analgesic effects when added to bupivacaine [22].
The time of two-segment regression was compared and found to be statistically significant (p-value <0.05). It was significantly faster in group BMS (142.0±19.95 minutes) than in group BM (159.4±17.36 minutes). In a study conducted by A Gupta et al., in 2006 [14], no statistically significant difference was found (p-value >0.05) between the two groups: Group-B (receiving 3.5 mL of 0.5% hyperbaric bupivacaine plus 0.5 mL saline 0.9% intrathecally) (108.8±14.7 minutes) and group BM (receiving 3.5 mL of 0.5% hyperbaric bupivacaine plus 0.5 mL preservative-free midazolam 2.5 mg intrathecally) (107.4±15.3) minutes.
The duration of sensory block between the two groups was compared and found to be statistically significant (p-value <0.05). It was prolonged in group BM (248±25.71 minutes) compared to group BMS (226.9±24.65 minutes). The duration of sensory block was longer in group BM than in group BMS. The results for the duration of sensory block coincide with the studies of Singh A et al., and Attia J et al., [13,18].
The duration of motor block between the two groups was also compared and found to be statistically significant (p-value <0.05). It was prolonged in group BM (220.6±27.55 minutes) compared to group BMS (194.7±25.01 minutes). The results for the duration of motor block coincide with the studies of Singh A et al., and Attia J et al., [13,18].
The time to rescue analgesia was prolonged in group BM (335.47±33.87 minutes) compared to group BMS (286.88±24.65 minutes). In the study of Singh A et al., the time to rescue analgesia was longer in group midazolam (378.5 minutes) than in group magnesium sulphate (306.2 minutes), which coincided with the results of the present study [13].
Investigation has shown that intrathecal midazolam produces dose-dependent antinociception sufficient to produce anaesthesia for abdominal surgery [23]. Patients do not require opioid analgesics when subjected to painful somatic stimuli, like lower limb surgery. The function of the sympathetic nervous system remains unaltered after the administration of intrathecal midazolam [21]. Magnesium sulphate exhibits a significant anti-nociceptive effect, preventing central sensitisation from peripheral nociceptive stimuli [24]. Magnesium blocks calcium influx into the cell and non competitively antagonises the NMDA receptors [25].
In terms of complications, group BMS was significantly better than group BM. In many cases in group BM, there was a significant fall in BP (p-value <0.05) after administering spinal anaesthesia, which was corrected by giving an intravenous injection of 6 mg ephedrine. Regarding other complications like nausea, vomiting, rigours, and respiratory depression, both groups were comparable (p-value >0.05). Attia J et al., found that both magnesium sulphate and midazolam did not cause any obvious side effects, such as hypotension or bradycardia [18]. Limbu PM et al., found that the occurrence of hypotension, bradycardia and shivering were common adverse effects, which were comparable between the two groups, similar to studies that have been tabulated in [Table/Fig-11] [13,18,19].
Comparison of various studies which used intrathecal midazolam and magnesium sulphate [13,18,19].
| Author and year of study | Place of study and sample size | Sample size | Doses of drugs used | Comment on intraoperative haemodynamics | Postoperative haemodynamics |
|---|
| Attia J et al., 2016 [18] | Minia, Egypt | 60 | Group-C: 2.5 mL of 0.5% hyperbaric bupivacaine+0.5 mL 0.9% salineGroup-A: 2.5 mL of 0.5% hyperbaric bupivacaine+0.5 mL midazolam 2.5 mgGroup-B: 2.5 mL of 0.5% hyperbaric bupivacaine+0.5 mL magnesium sulphate 50 mg | There was no change in Heart Rate (HR) and Blood Pressure (BP). | Postoperatively, there were no any obvious side-effects like hypotension, bradycardia. |
| Limbu PM et al., 2017 [19] | Dharan, Nepal | 60 | Group-A: 3 mL of 0.5% hyperbaric bupivacaine+0.15 mL magnesium sulphate 75 mgGroup-B: 3 mL of 0.5% hyperbaric bupivacaine+0.15 mL NS | Occurrence of hypotension and bradycardia were comparable in both the groups. | There were no cases of hypotension or bradycardia in any of the groups. |
| Singh A et al., 2019 [13] | Madhya Pradesh, India | 60 | Group MZ: 3 mL of 0.5% hyperbaric bupivacaine+0.5 mL midazolam 2 mgGroup-MG: 3 mL of 0.5% hyperbaric bupivacaine+0.5 mL magnesium sulphate 50 mg | Comparison of pulse rates and Mean Arterial Pressure (MAP) in both the groups and were found comparable without any statistical significance. | No comments on postoperative haemodynamics. |
| Present study | Gujarat, India | 64 | Group BM: 3.2 mL of 0.5% hyperbaric bupivacaine+0.5 mL of midazolam 2.5 mgGroup BMS: 3.2 mL of 0.5% hyperbaric bupivacaine+0.5 mL of magnesium sulphate 50 mg | Incidence of bradycardia and hypotension were noted more in Group BM as compared to Group BMS (p-value <0.05). | Bradycardia and hypotension were seen in Group BM. |
Limitation(s)
The limitations of the study include the limited population of a single-centred. It does not include patients undergoing emergency surgeries, including polytrauma.
Conclusion(s)
Intrathecal preservative-free magnesium sulphate (50 mg) added to 0.5% hyperbaric bupivacaine provided better haemodynamic stability than intrathecal preservative-free midazolam (2.5 mg). However, intrathecal midazolam was more efficient regarding the onset and duration of sensory and motor blockade, and postoperative analgesia, compared to magnesium sulphate (50 mg).
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test; *The p-value <0.05 was considered statistically significant
Student’s t-test: *The p-value <0.05 was considered statistically significant
Chi-square test; *The p-value <0.05 was considered statistically significant