Infraumbilical surgeries are associated with moderate to severe postoperative pain due to the abdominal wall incision, which causes irritation of nerve roots and myofascial structures [1]. Uncontrolled postoperative pain can negatively impact ambulation, increasing the risk of complications such as deep vein thrombosis, atelectasis and prolonged hospital stays [1,2]. Effective postoperative analgesia is crucial for facilitating rehabilitation, ensuring early recovery and improving patient satisfaction [2].
Opioids, though considered the gold standard for postoperative pain management, are associated with side effects like nausea, vomiting, constipation, pruritus and respiratory depression, especially when administered systemically or neuraxially [3,4]. Also, opioids and Non Steroidal Anti-inflammatory Drugs (NSAIDS) have been reported to cause inadequate pain control in post hernia surgery patients [5]. Therefore, alternative analgesic regimens with a better safety profile are needed, particularly for patients who cannot tolerate haemodynamic instability. Incorporating regional nerve blocks as part of an opioid-sparing multimodal analgesic technique can help achieve this goal [6].
The TAP block is a widely used analgesic method for postoperative pain relief in infraumbilical surgeries [7,8]. First described by Rafi AN, the TAP block involves injecting local anaesthetic into the fascial plane between the two anterior abdominal wall muscles, namely the internal oblique and transversus abdominis, where it blocks the nerves supplying the anterolateral abdominal wall (T7 to L1) [8]. By blocking these nerves, this technique provides effective analgesia for the skin, muscles and parietal peritoneum of the anterior abdominal wall [9]. The block can be performed using landmark-based techniques or with ultrasound guidance for improved accuracy and safety [7,10].
Ropivacaine is a long-acting amide local anaesthetic commonly used for TAP blocks due to its better safety profile compared to bupivacaine [3,11]. However, the duration of analgesia provided by ropivacaine alone may be limited. Adjuvants like dexamethasone and dexmedetomidine have been investigated to prolong the duration of the block and improve the quality of analgesia [11-13].
Dexamethasone is a potent anti-inflammatory glucocorticoid that has been shown to extend the duration of peripheral nerve blocks when used as an adjuvant to local anaesthetics [12,13]. Its effects are mediated through the inhibition of nociceptive C-fibre activity and the release of inflammatory mediators.
Dexmedetomidine is a highly selective alpha-2 adrenergic receptor agonist that has analgesic, sedative and sympatholytic properties [11]. When added to local anaesthetics, dexmedetomidine enhances the duration and quality of analgesia by causing hyperpolarisation of nerve membranes and inhibiting the conduction of pain signals. It significantly prolongs the duration of sensory and motor blockade in various regional anaesthesia techniques [14,15].
While both dexamethasone and dexmedetomidine have shown promise as adjuvants in TAP blocks, there is limited data directly comparing their efficacy [1,9,11,15,16]. Thus, present study aimed to compare the postoperative analgesic efficacy of dexmedetomidine versus dexamethasone as adjuvants to ropivacaine in landmark-guided TAP block for infraumbilical surgeries. The primary objective was to compare the duration of analgesia (the time of first rescue analgesia) and the quality of pain relief, as assessed by the Visual Analogue Scale (VAS), between the two groups. The secondary objective was to compare the postoperative haemodynamic changes and side effects. The findings of present study could help identify the best drug combinations used in TAP block to improve the quality and duration of postoperative analgesia in patients undergoing infraumbilical surgeries. It was hypothesised that dexmedetomidine, as an adjuvant to ropivacaine in the TAP block, would provide superior postoperative analgesia.
Materials and Methods
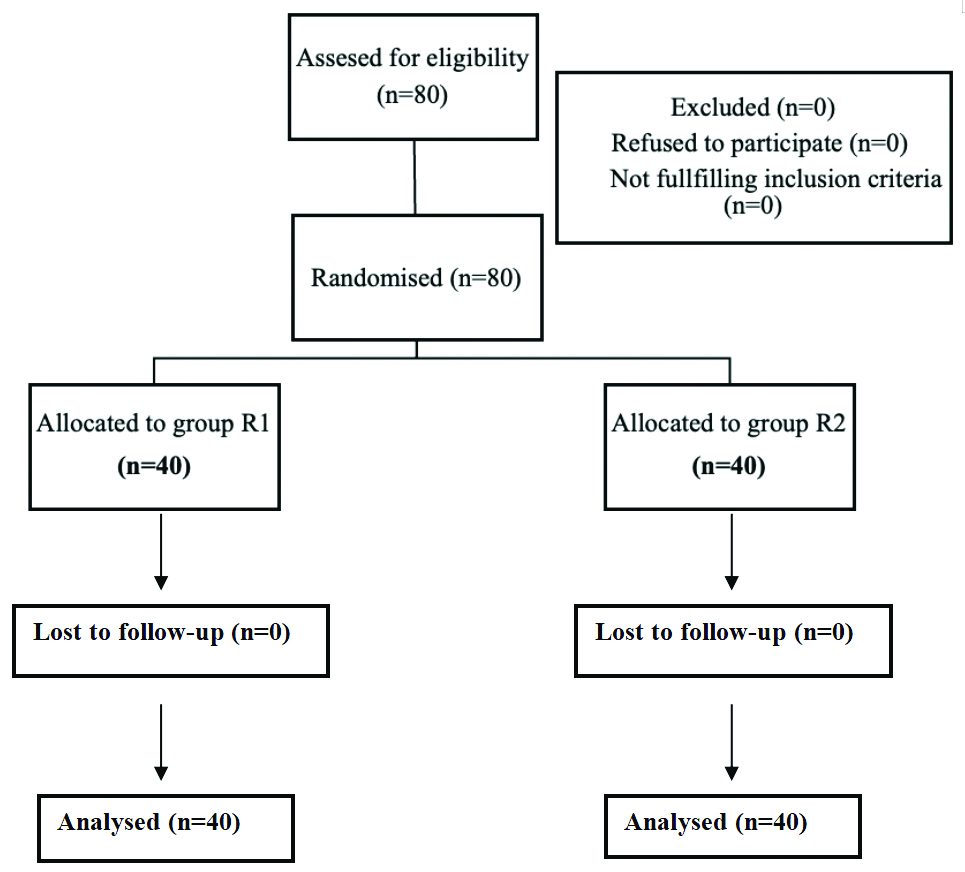
Present randomised double-blinded prospective clinical study was conducted in the Department of Anaesthesia, Shrimati Bhikhiben Kanjibhai Shah Medical Institute and Research Centre (SBKS MIRC), Piparia, Vadodara, Gujarat, India. After obtaining approval from the Institutional Ethical Committee (SVIEC/UN/MEDI/BNPG23/AUG/24/72), the study was carried out over a period of 18 months (from March 2023 to September 2024) on patients undergoing elective infraumbilical surgeries (open abdominal hysterectomy and bilateral open inguinal hernia repair) under spinal anaesthesia. Written informed consent was obtained from all participants. This study conformed to Institutional Ethics Committee standards and the Helsinki Declaration. No names or initials were used in the study. The Consolidated Standards of Reporting Trials (CONSORT) statement [Table/Fig-1] was followed to conduct this single-centre, double-blinded Randomised Controlled Trial (RCT) with two parallel groups.
Inclusion criteria: Patients aged 18-60 years, belonging to the American Society of Anaesthesiologists (ASA) classification Grade I and II (well-controlled systemic diseases), who underwent elective open abdominal hysterectomies and bilateral open inguinal hernia repair under spinal anaesthesia were included in the study.
Exclusion criteria: Patients who were not willing to participate, had arrhythmias or heart block, were on beta blockers, had coagulation disorders or were on anticoagulant therapy, had infections or deformities or scars at the proposed puncture site, had allergies to the study drug, were classified as ASA Grade III (uncontrolled systemic disease of the heart, liver, kidney, hypertension, or diabetes) or IV, were underweight or obese {Body Mass Index (BMI) <18.5 kg/m2 or ≥30 kg/m2}, or underwent surgeries with prolonged duration (≥3 hours) or involving excessive tissue manipulation or major blood loss were excluded from the study.
Sample size calculation: The sample size was calculated using Process Automation Software System (PASS) 15 (NVSS: National Vital Statistics System). A pilot study was performed with 15 patients in each group, which detected a predicted difference of 35% for the duration of postoperative analgesia between the two groups, with a type I error (α) of 0.05 and a power of 0.8 for the study. The calculated sample size was 75. To minimise the effect of data loss, 40 patients were recruited in each group.
Study Procedure
In this parallel group design study, patients who met the inclusion criteria were divided into two groups of 40 patients each, based on a randomised computer-generated sequence. Both the assessor and the patients were blinded to the group allocation, using opaque sealed envelope methods.
Group-R1 received Inj. Ropivacaine 0.2% (3 mg/kg)+Inj. Dexamethasone (0.1 mg/kg) [7], while Group-R2 received Inj. Ropivacaine 0.2% (3 mg/kg)+Inj. Dexmedetomidine (1 μg/kg) [7] in bilateral landmark-guided TAP block. The total volume of the study drug in both groups was made up to 50 mL after adding normal saline, with 25 mL given on each side. As per the envelope, the study drug was prepared and administered to the assigned group by an anaesthesiologist not included in the study.
Preanaesthetic evaluation was conducted one day prior to the surgery and patients were educated on the assessment of postoperative evaluation using the Visual Analogue Scale (VAS) [17]. They were instructed not to take solid food six hours prior and clear fluids two hours prior to surgery. After thoroughly explaining the procedure, informed consent was documented.
Intravenous fluid was administered through an 18-gauge intravenous cannula before the surgery. Intravenous Inj. Glycopyrrolate 0.004 mg/kg and Inj. Ondansetron 0.1 mg/kg were given as premedication.
Surgery commenced after administering spinal anaesthesia using Inj. Hyperbaric Bupivacaine 0.5% (4 mL) and achieving a sensory level of T7. After the surgery was completed, bilateral TAP block was administered using the landmark technique, wherein a 23-gauge 1.5-inch blunt-tipped needle was placed in the triangle of Petit at the mid-axillary line, immediately above the iliac crest. A total of 25 mL of the study drug was given on each side after two pop sounds were heard (one pop sound when the needle passed through the external oblique muscle and another when the internal oblique muscle was crossed) following negative aspiration.
Postoperative pain was assessed using the VAS every 30 minutes for the first two hours and then hourly until the VAS reached ≥4, as evaluated by an independent, blinded observer. The time from TAP block administration (taken as zero) to the first administration of rescue analgesia (Inj. Diclofenac 75 mg) at VAS ≥4 was documented as the duration of analgesia [7]. Haemodynamic parameters, including Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Heart Rate (HR) and Saturation (SpO2), were monitored at the same intervals. Any adverse effects were recorded.
The data obtained from the case reports of each of the study participants were decoded and analysed after the end of the study.
Statistical Analysis
The sample size of 80 patients, with 40 patients in each group, was determined using MedCalc 12.5 software. The collected data were tabulated for assessment. Numerical/continuous variables were presented as mean and Standard Deviations (SD), while categorical variables were presented as frequencies and percentages. Tests such as the unpaired Student’s t-test and/or Analysis of Variance (ANOVA) were used for numerical variables whenever appropriate for intergroup comparisons, while the Chi-square test was used for categorical variables. A p-value <0.05 was considered statistically significant, while a p-value <0.001 was regarded as highly significant.
Results
All selected patients were able to complete the study without any dropouts. Both groups were comparable in terms of age, weight, gender, ASA classification, type of surgery and total duration of surgery (p-value >0.05) [Table/Fig-2]. The time duration to first rescue analgesia was significantly longer in Group-R2 compared to Group-R1 (308.18±12.3 vs. 239.78±14.23 minutes, p<0.0001) [Table/Fig-3].
Comparison of demographic parameters.
| Parameters | Group-R1 | Group-R2 | p-value |
|---|
| Age (Years) (Mean±SD) | 40.15±7.46 | 39.5±5.59 | 0.6604 |
| Weight (kg) (Mean±SD) | 60.23±6.76 | 61.03±5.03 | 0.5499 |
| Gender (n, %) | Male: 19 (47.5%) | Male: 18 (45%) | 0.823 |
| Female: 21 (52.5%) | Female: 22 (55%) |
| ASA Grade (n, %) | I: 26 (65%) | I: 29 (72.5%) | 0.6295 |
| II: 14 (35%) | II: 11 (27.5%) |
| Type of surgery (n, %) | Open abdominal hysterectomy: 21 (52.5%) | Open abdominal hysterectomy: 22 (55%) | 0.823 |
| Bilateral open inguinal hernia: 19 (47.5%) | Bilateral open inguinal hernia: 18 (45%) |
| Mean duration of surgery (Minutes) | 124.13±10.36 | 122.25±7.68 | 0.3594 |
Unpaired Student’s t-test and Chi-square test were used as statistical test; p-value ≤0.05 statistically significant
Time of first rescue analgesia.
| Parameter | Group-R1 | Group-R2 | p-value |
|---|
| Mean±SD | Mean±SD |
|---|
| Duration to rescue analgesia | 239.78±14.23 | 308.18±12.3 | <0.0001 |
The postoperative pain intensity assessed by VAS scores was significantly lower in Group-R2 compared to Group-R1 at all time points from 30 minutes to six hours post-block (p<0.0001) [Table/Fig-4]. The median (interquartile range) VAS scores were consistently lower in the dexmedetomidine group, suggesting a better quality of analgesia [Table/Fig-5].
Comparison of postoperative VAS score.
| Time (in hours) | Group-R1 | Group-R2 | p-value |
|---|
| Mean±SD | Mean±SD |
|---|
| 0 | 4.35±0.58 | 4.4±0.63 | 0.7129 |
| 0.5 | 0.25±0.44 | 0.1±0.3 | 0.0787 |
| 1 | 1.05±0.5 | 0.35±0.48 | <0.0001 |
| 1.5 | 1.73±0.45 | 0.98±0.16 | <0.0001 |
| 2 | 2.28±0.55 | 1.1±0.3 | <0.0001 |
| 3 | 2.73±0.45 | 1.6±0.55 | <0.0001 |
| 4 | 3.55±0.6 | 2.3±0.52 | <0.0001 |
| 5 | 4.33±0.49 | 3.2±0.65 | <0.0001 |
| 6 | NA | 4.1±0.31 | NA |
NA: Rescue analgesia given
Comparison of median (interquartile range) VAS scores postoperative VAS score.
| Time (in hours) | Group-R1 | Group-R2 | p-value |
|---|
| Median (Q1-Q3) | Median (Q1-Q3) |
|---|
| 0 | 4 (4-5) | 4 (4-5) | NA |
| 0.5 | 0 (0-0.25) | 0 (0-0) | NA |
| 1 | 1 (1-1) | 0 (0-1) | <0.0001 |
| 1.5 | 2 (1-2) | 1 (1-1) | <0.0001 |
| 2 | 2 (2-3) | 1 (1-1) | <0.0001 |
| 3 | 3 (2-3) | 2 (1-2) | <0.0001 |
| 4 | 4 (3-4) | 2 (2-3) | <0.0001 |
| 5 | 4 (4-5) | 3 (3-4) | <0.0001 |
| 6 | NA | 4 (4-4) | NA |
NA: Rescue analgesia given
There were no statistically significant differences in the haemodynamic parameters {heart rate, systolic blood pressure, diastolic blood pressure, Mean Arterial Pressure (MAP) and SpO2} between the two groups (p>0.05) [Table/Fig-6]. Additionally, there were no significant incidences of side effects such as bradycardia, hypotension, nausea, vomiting, respiratory depression, dry mouth, or excessive sedation in either group during the study period.
Comparison of haemodynamic parameters.
| Time (hours) | Heart rate (bpm) Group-R1 | Heart rate (bpm) Group-R2 | Systolic BP (mmHg) Group-R1 | Systolic BP (mmHg) Group-R2 | Diastolic BP (mmHg) Group-R1 | Diastolic BP (mmHg) Group-R2 | Mean arterial pressure (mmHg) Group-R1 | Mean arterial pressure (mmHg) Group-R2 | Oxygen saturation (SpO2) Group-R1 | Oxygen saturation (SpO2) Group-R2 |
|---|
| 0 | 83.3±5.9 | 83.6±6.1 | 119.58±4.4 | 119±4.65 | 75.6±4.99 | 74.05±4.09 | 88.25±4.31 | 89.68±2.96 | 99.03±0.62 | 98.95±0.64 |
| 0.5 | 94.15±5.71 | 92.25±8.53 | 108.98±4.35 | 107.53±4.61 | 67.2±4.98 | 65.8±2.95 | 81.13±4.29 | 79.71±3.98 | 98.2±0.85 | 98.23±1.19 |
| 1 | 92.15±5.78 | 91.43±8.04 | 110.7±4.21 | 109.28±4.55 | 67.58±5.11 | 66.3±3.09 | 81.95±4.36 | 80.63±3.17 | 98.33±0.76 | 98.38±0.81 |
| 1.5 | 91.08±5.94 | 90.63±7.93 | 111.13±4.31 | 109.85±4.41 | 68.23±5.06 | 66.9±3.04 | 82.53±4.33 | 81.22±3.07 | 98.53±0.75 | 98.45±0.81 |
| 2 | 90.2±5.63 | 89.98±7.79 | 112.4±4.04 | 110.83±4.56 | 68.8±5.13 | 67.48±3.15 | 83.33±4.32 | 81.93±3.19 | 98.68±0.69 | 98.55±0.81 |
| 3 | 89.33±5.69 | 88.68±7.54 | 113.93±4.23 | 112.48±4.67 | 70.2±5.28 | 68.65±3.35 | 84.78±4.57 | 83.26±3.37 | 98.78±0.62 | 98.68±0.73 |
| 4 | 88.58±5.58 | 87.9±7.24 | 114.88±4.03 | 113.43±5.13 | 70.88±5.34 | 69.33±3.41 | 85.54±4.58 | 84.03±3.59 | 98.88±0.52 | 98.73±0.64 |
| 5 | 87.83±5.68 | 87.35±7.11 | 116.33±4.11 | 114.65±4.93 | 71.6±5.46 | 70.23±3.86 | 86.51±4.64 | 85.03±3.85 | 98.85±0.58 | 98.83±0.59 |
| 6 | 86.9±5.91 | 86.6±7.28 | 117.13±4.29 | 115.75±5.13 | 72.35±5.67 | 70.48±4.21 | 87.28±4.85 | 85.48±4.36 | 98.9±0.63 | 98.85±0.62 |
| 7 | 86.08±5.75 | 86.03±6.96 | 118.23±4.39 | 116.7±5.15 | 72.93±5.75 | 71.05±4.34 | 88.03±4.94 | 86.22±4.41 | 98.95±0.69 | 98.9±0.59 |
| 8 | 85.5±5.85 | 85.68±6.62 | 118.93±4.56 | 117.5±5.47 | 73.75±5.82 | 71.65±4.48 | 88.81±5.05 | 86.9±4.54 | 98.95±0.69 | 98.93±0.62 |
| 9 | 84.98±5.62 | 85.28±6.41 | 119.55±4.61 | 118.3±5.38 | 74.6±5.85 | 72.63±4.63 | 89.58±5.12 | 87.65±4.58 | 99±0.64 | 98.95±0.64 |
| 10 | 84.3±5.87 | 84.7±6.31 | 120.28±4.61 | 118.93±5.54 | 75.08±6.08 | 73.13±4.78 | 90.14±5.26 | 88.39±4.71 | 99±0.64 | 98.95±0.64 |
| 11 | 83.85±5.78 | 84.28±6.14 | 120.7±4.77 | 119.35±5.54 | 75.68±6.37 | 73.58±4.74 | 90.68±5.47 | 90.23±4.58 | 99±0.64 | 98.95±0.64 |
| 12 | 83.45±5.94 | 83.95±6.07 | 120.95±4.84 | 119.95±5.77 | 76.35±6.54 | 74.1±4.78 | 91.22±5.68 | 89.38±4.89 | 99±0.64 | 98.95±0.64 |
Discussion
In the present prospective randomised clinical study, dexmedetomidine provided a longer duration and better quality of postoperative analgesia compared to dexamethasone as an adjuvant to ropivacaine in TAP block for infraumbilical surgeries, with comparable haemodynamic parameters and incidences of adverse effects, thus accepting the hypothesis.
Postoperative pain management is a crucial component of perioperative care, as inadequate pain control can lead to delayed recovery, prolonged hospital stays and an increased risk of chronic pain [1,2]. The TAP block has emerged as an effective regional analgesic method for abdominal surgeries, providing effective analgesia to the skin, muscles and parietal peritoneum of the anterior abdominal wall by blocking the sensory nerves in the TAP [3]. However, the duration of analgesia with local anaesthetics alone may be limited, prompting the use of adjuvants to prolong the block duration, improve the quality of analgesia and decrease local anaesthetic toxicity [8,13].
The present study compared the efficacy of dexmedetomidine and dexamethasone as adjuvants to ropivacaine in TAP block for infraumbilical surgeries for postoperative analgesia. The baseline demographic profiles of patients in both study groups were comparable. The duration of postoperative analgesia, defined as the time from TAP block administration (taken as zero) to the first rescue analgesia (Inj. Diclofenac 75 mg) administration at VAS ≥4, was 22.19% longer in the dexmedetomidine group than in the dexamethasone group. Additionally, it provided better quality of analgesia, evidenced by significantly lower VAS scores at all time intervals post study drug administration until rescue analgesia was demanded.
Through an extensive literature search, it was observed that various authors investigated the effectiveness of TAP block in different surgeries using different local anaesthetics with varying doses of dexmedetomidine and/or dexamethasone as adjuvants. [Table/Fig-7] describes those studies and their findings [1,6,9,11,15,16,18-22].
Summary of different studies on TAP block using dexmedetomidine and/or dexamethasone as adjuvants [1,7,9,11,15,16,18-22].
| S. No. | Author name | Year | Place of study | Intervention | Parameters assessed | Conclusion |
|---|
| 1 | Gupta A et al., [1] | 2019 | New Delhi, India | Dexamathasone 4 mg vs control with ropivacaine 0.375% in ultrasound-guided TAP block in caesarean section | Time to first rescue analgesia, total amount of analgesia required in first 24 h postoperatively, VAS score and incidence of nausea and vomiting. | Dexamathasone significantly prolonged postoperative analgesia |
| 2 | Singla N et al., [7] | 2021 | Tamil Nadu, India | Dexamethasone 0.1 mg/kg vs Dexmedetomidine 1 μg/kg with ropivacaine 3 mg/kg in US guided TAP block in caesarean section | Time to initial self-reporting of postoperative pain, time to first rescue analgesic demand, Visual Analogue Scale (VAS) for pain haemodynamic parameters and adverse effects. | Dexmedetomidine better than dexamethasone better in proving prolonged postoperative analgesia |
| 3 | Xue Y et al., [9] | 2018 | China | Dexmedetomidine 1 μg/kg vs control with 0.375% ropivacaine in ultrasound-guided TAP block in gynaecological laproscopy under general anaesthesia | Dosage of propofol, duration of the operation, time of awakening, spontaneous breathing, (VAS) scores, incidence of nausea, vomiting, and respiratory depression. | Dexmedetomidine as adjuvant to ropivacaine improves postoperative analgesia |
| 4 | Zeng Y et al., [11] | 2020 | China | 0.5, 1, 2 μg/kg dexmedetomidine as adjuvant to 0.3% Ropivacaine in ultrasound-guided TAP block in laparotomy for gynecologic malignancies | Numerical Rating Scale (NRS), Ramsay Sedation Scale (RSS) scores, the first request time for analgesia bolus, oxycodone hydrochloride consumption, the plasma concentration of ropivacaine, the incidence of postoperative complications and adverse events, and patient satisfaction. | Postoperative analgesia was prolonged in 2 μg/kg dexmedetomidine due to excessive sedation |
| 5 | Garg K et al., [15] | 2021 | Chandigarh, India | 1 μg/kg dexmedetomidine vs control with 0.5 mL/kg of 0.2% ropivacaine in ultrasound-guided TAP block in paediatric laparoscopic surgeries | Vital signs, pain, sedation, time to first rescue analgesic and total analgesic consumption for 24 h. | Dexmedetomidine as adjuvant to ropivacaine improves postoperative analgesia |
| 6 | Zeng H et al., [16] | 2024 | Sichuan, China | 10 mg dexamethasone vs 1 μg/kg dexmedetomidine vs 1 μg/kg dexmedetomidine+10 mg dexamethasone with 0.25% ropivacaine in ultrasound-guided TAP block in laprotomy for gastric cancer patients | Incidence of moderate-to-severe pain in 24 h on movement, pain score, opioids use, recovery quality and adverse effects. | Combination with dexamethasone and dexmedetomidine as adjuvants for TAP block provided prolonged duration of analgesia |
| 7 | Bansal P and Sood D [18] | 2018 | Punjab, India | 50 μg of dexmedetomidine vs control with 3 mg/kg of ropivacaine in ultrasound-guided TAP block in caesarean section | Time to initial reporting of pain, time to first rescue analgesia, quality of block and side-effects. | Dexmedetomidine delays time to onset of pain and use of rescue analgesia |
| 8 | Yarramsetti VR et al., [19] | 2022 | Andhra Pradesh, India | 20 μg dexmedetomidine vs 8 mg dexamethasone with 10 mL of 0.5% bupivacaine+10 mL of 2% lignocaine adrenaline in US guided TAP block in caesarean delivery | Pain up to 12 hours of surgery based on a Visual Analog Scale (VAS). | Dexmedetomidine was more effective when compared to dexamethasone in TAP block for postoperative analgesia |
| 9 | Partani S et al., [20] | 2024 | Rajasthan, India | 0.1 mg/kg dexamethasone vs 0.5 μg/kg dexmedetomidine vs control with 0.25% levobupivacaine in US guided TAP block in unilateral inguinal herniorrhaphy | VAS score, time for request of first analgesia (TFA), total number and total dose of rescue analgesic in 24 hours. | Both dexmedetomidine and dexamethasone were comparable |
| 10 | Kartalov A, et al., [21] | 2015 | Macedonia | General anaesthesia vs GA+unilateral TAP block with 0.5% ropivacaine vs GA+unilateral TAP block with 0.5% ropivacaine+4 mg Dexamethasone in Inguinal Hernia Repair | VAS at rest at 2, 4, 6, 12 and 24 hours after the operation and the total analgesic consumption of morphine over 24 hours. | TAP block with dexamethasone was better for postoperative analgesia |
| 11 | Abdel-wahab AH et al., [22] | 2021 | Egypt | Dexamethasone (4 mg vs 8 mg) with 0.5% bupivacaine in unilateral US guided TAP block in inguinal hernia repair | Time of the first analgesic request, and the secondary outcome measure was the VAS scale in the first postoperative 24 h. | Both groups were comparable |
| 12 | Present study | 2024 | Gujarat, India | Dexamethasone 0.1 mg/kg vs dexmedetomidine 1 μg/kg with 0.2% ropivacaine in bilateral landmark guided TAP block for abdominal hysterectomy and bilateral inguinal hernia repair | Visual Analog Scale (VAS) score, time to request for first rescue analgesia and haemodynamic parameters. | Dexmedetomidine provided longer duration and better quality of postoperative analgesia without significant side-effects |
The findings of the current study were consistent with those of various authors [7,9,11,15,18,19], who concluded that dexmedetomidine has higher efficacy, providing a significantly longer duration of analgesia and lower VAS scores at the time of the first analgesic request compared to dexamethasone at different doses as an adjuvant to local anaesthetic agents in TAP block.
The present study demonstrated that a lower dose of dexmedetomidine at 1 μg/kg was effective with minimal side effects. Zeng Y et al., compared different doses of dexmedetomidine (0.5, 1 and 2 μg/kg) in TAP block and found that while the duration of analgesia was significantly prolonged at the 2 μg/kg dose, it was also associated with excessive sedation [11].
Xue Y et al., compared dexmedetomidine as an adjuvant to 0.375% ropivacaine versus plain 0.375% ropivacaine in TAP block against intravenous analgesics and found that pain control was significantly more effective in the TAP block with dexmedetomidine [9]. This suggests that the TAP block can significantly improve pain management in the postoperative period compared to intravenous analgesics. As an adjuvant to local anaesthetics, dexmedetomidine has proven to be more effective than dexamethasone in other peripheral nerve blocks (e.g., brachial plexus block, caudal block) as well [23-25].
In contrast to the findings of the current and previously mentioned studies [7,9,11,15,18,19], where dexmedetomidine was found to be more effective, Partani S et al., found equal efficacy of dexmedetomidine and dexamethasone as adjuvants to levobupivacaine in TAP block for unilateral inguinal herniorrhaphy [20]. Maagaard M et al., conducted a meta-analysis and trial sequential analysis on the effects of combined dexamethasone and dexmedetomidine as adjuncts to peripheral nerve blocks. They found that the combination increased the duration of analgesia compared to placebo and dexmedetomidine alone [26]. Furthermore, this combination provided a similar duration of analgesia to that of dexamethasone and concluded that it is reasonable to use dexamethasone as the sole adjunct if the goal is to increase the duration of analgesia.
Postoperative haemodynamic parameters such as heart rate, SBP, DBP and respiratory rate were comparable between the groups in present study. Similar findings were observed by Garg K et al., in their study, which indicated no significant difference in the postoperative haemodynamic parameters between both groups [15]. However, in contrast, Singla N et al., reported that 10% of patients in the dexmedetomidine group experienced hypotension and bradycardia, while the dexamethasone group maintained stable haemodynamics [7]. This may be due to a decrease in the release of noradrenaline from the sympathetic nervous system, which might have exacerbated the decrease in systemic vascular resistance observed in their pregnant study patients.
In the current study, none of the patients experienced nausea, vomiting, respiratory depression, or sedation. Similar results were noted by Kartalov A et al., and Abdel-Wahab AH et al., where no major postoperative side effects were reported between both study groups [21,22].
Although various studies have suggested the efficacy of either dexamethasone or dexmedetomidine, this study demonstrated the dose-specific superiority of dexmedetomidine over dexamethasone [7,9,11,15,16,18-21]. This knowledge can help in modifying TAP block techniques for managing postoperative analgesia in infraumbilical surgery and can positively impact total systemic opioid consumption, patient satisfaction and long-term outcomes such as chronic pain and quality of life.
The present study has several strengths, including its randomised design, the use of expert guidance for precise TAP block administration and the comprehensive assessment of postoperative pain and haemodynamic parameters.
At the same time, there are various factors that might have affected the outcome of the study. Since pain is a subjective experience, many elements of the biopsychosocial components can impact pain assessment. This can be influenced by a family or personal history of mental health disorders, pre-existing chronic pain conditions, substance abuse, or opioid dependence, which may lead to lower pain thresholds and desensitisation to previously used analgesics. The VAS scale, when used for assessing pain, requires patients to express abstract sensory experiences using a linear measure, which may vary according to their cognitive skills and understanding, potentially impacting the pain assessment. In addition to these factors, disparities in anaesthetic sensitivity due to different ethnic backgrounds can significantly affect the outcome of this study. Furthermore, the time point at which the TAP block begins to take effect and the time at which the sensory effects of spinal anaesthesia begin to wear off could not be differentiated, which may be important in assessing postoperative analgesia provided by the TAP block.
Limitation(s)
Despite the attempt to compare these promising adjuvants in TAP block for postoperative pain relief in infra-umbilical surgeries, present study has several limitations. Firstly, postoperative analgesia and side effects were monitored for only 24 hours after surgery and thus, the complete analgesic efficacy and any delayed side effects of these drugs during the 48-hour postoperative period could not be assessed. Secondly, pain scores were measured at rest and pain and analgesic requirements during mobilisation could not be monitored, which is important as early ambulation is crucial for these patients. Thirdly, total analgesic consumption in both groups during the postoperative period was not assessed, which could have strengthened the study results. Additionally, a comparison with a placebo group or intravenous control was not conducted, making it impossible to ascertain whether the effects of dexamethasone or dexmedetomidine were due to systemic absorption or through perineural action. Lastly, as this is a single-centre hospital-based study, it lacks generalisability. These limitations can be addressed in further studies.
Conclusion(s)
For patients undergoing infra-umbilical surgeries, 0.2% ropivacaine with dexmedetomidine administered in the bilateral TAP block provided a longer duration and better quality of postoperative analgesia without significant side effects compared to dexamethasone as an adjuvant. Thus, it can be safely applied in patients undergoing such surgeries to improve postoperative pain relief and expedite the recovery process. Future research can assess the effectiveness of TAP block with these adjuvants administered preoperatively to evaluate their effect on intraoperative analgesia, as well as the effectiveness of these adjuvants on long-term outcomes such as chronic pain and quality of life.
Unpaired Student’s t-test and Chi-square test were used as statistical test; p-value ≤0.05 statistically significant
NA: Rescue analgesia given
NA: Rescue analgesia given