The I-gel is a second-generation Supraglottic Airway Device (SAD) featuring a thermoplastic elastomer gel cuff that eliminates the need for inflation, as well as a gastric side channel for gastric tube insertion and gas venting [1,2]. SADs deliver anaesthetic gases and oxygen above the vocal cords, circumventing the drawbacks of endotracheal intubation, such as tissue damage and exaggerated haemodynamic responses. Despite their advantages, SADs can provoke stress responses, including hypertension, tachycardia and bronchospasm, which are generally short-lived and manageable [3]. Proper depth of anaesthesia is crucial during I-gel insertion to prevent complications such as coughing, gagging and laryngospasm [4,5].
Thiopentone, an ultra-short-acting barbiturate, is cheaper than propofol and causes less hypotension and pain during injection; however, it lacks good jaw relaxation and may lead to coughing and laryngospasm [9].
Materials and Methods
The interventional study was conducted at a tertiary care hospital in the Anaesthesiology Department of Dhiraj General Hospital in Piparia, Vadodara, Gujarat, India from August 1, 2023, to July 31, 2024. Ethical approval was obtained from the Institutional Ethical Committee before the study (SVIEC/ON/MEDI/SRP/JULY/23/124).
Inclusion and Exclusion criteria: Patients of either gender, aged between 18 and 60 years, who belonged to ASA grade I or II, scheduled for elective surgeries and undergoing general anaesthesia, were included in this study [Table/Fig-1]. Patients with limited mouth opening (less than 2 cm), an increased risk of aspiration, or a history of symptomatic gastroesophageal reflux or hiatal hernia were excluded from the study.
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
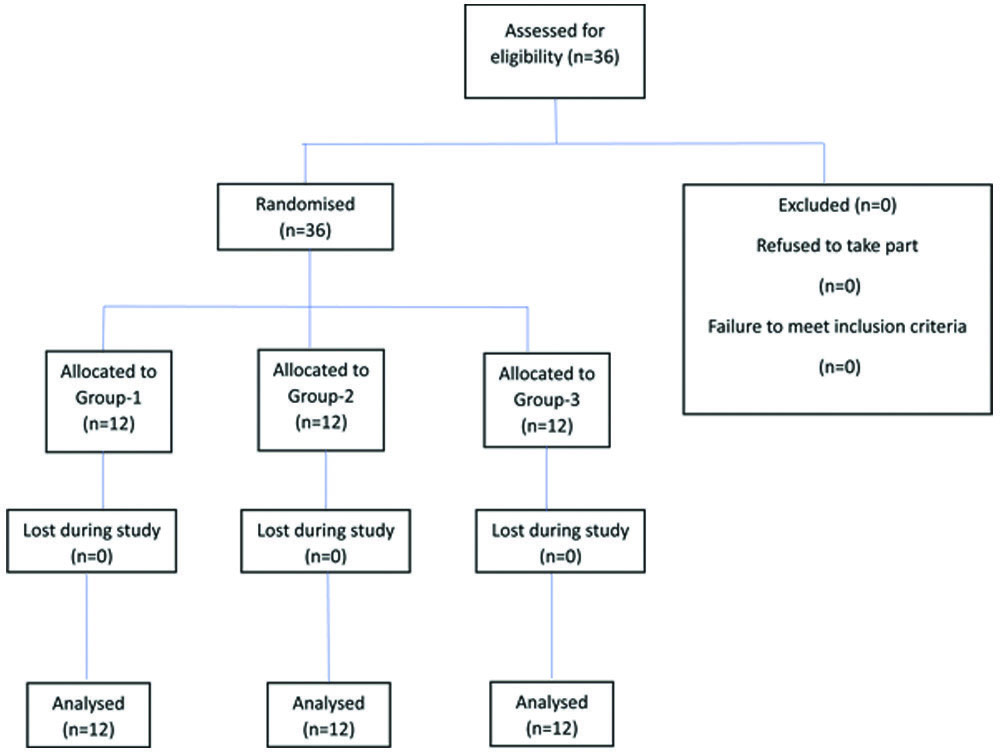
Sample size calculation: The StatCalc Epi info 7.1.1 (Fleiss) software was used to calculate the sample size for each group based on the ease of I-gel insertion conditions among three groups. For a type one error of 0.05 and a type two error of 0.2, with a power of 80% and a confidence interval of 95%, the sample size was determined to be 36 patients, with 12 patients in each group.
Study Procedure
These patients were randomly divided into three groups (12 patients in each group) using a computer-generated random number table from StatTrek. A sealed envelope was prepared and opened by the consultant anaesthesiologist, who administered the induction agent according to the group assignment. The procedure for inserting the I-gel was performed by another anaesthesiologist who was unaware of the assigned induction agent. Monitoring of the parameters was also conducted by the performing anaesthesiologist. This was a double-blind study, as both the patient and the anaesthesiologist performing the insertion were unaware of the group assignments.
A thorough preanaesthetic assessment, comprising medical history, physical examination, airway evaluation and routine investigations, was conducted a day before the surgery. The patients were kept nil by mouth for eight hours for solids and two hours for clear liquids prior to the surgery. On the day of the surgery, the patients were transferred to the preoperative area, where a preoperative check-up was performed. The procedure was then thoroughly explained to the patients in their native language and written informed consent was obtained. The patients were subsequently moved to the operating theatre, where a multipara monitor was attached and baseline vital signs were recorded.
The patient received premedication consisting of intravenous injections of glycopyrrolate (0.2 mg), ondansetron (4 mg) and midazolam (0.5 mg). Following preoxygenation with 100% oxygen via face mask for three minutes, anaesthesia was induced using one of three induction agents: Group-1 (propofol 2 mg/kg) [5], Group-2 (ketofol, a combination of ketamine 1 mg/kg and propofol 1 mg/kg), or Group-3 (thiopental 4 mg/kg) [18]. Jaw mobility was then assessed using a scoring system: 1 (fully relaxed), 2 (mild resistance), 3 (tight but opens), or 4 (closed) [10,11]. If inadequate jaw mobility or movement was observed, additional doses of the induction agent (up to 0.5 mg/kg, a maximum of three times) were administered. If all attempts failed, endotracheal intubation was performed. Otherwise, an appropriately sized I-gel was inserted.
Several parameters were evaluated, including ease of insertion, which was assessed as easy or difficult, insertion duration and any adverse reactions such as coughing, gagging, or laryngospasm. Easy insertion means there was no adverse response, such as gagging, coughing, or movement noted and no additional boluses of drugs were needed. Any adverse response requiring additional boluses of drugs or more than two attempts were considered difficult insertion [4].
The duration of I-gel insertion was measured from the cessation of mask ventilation to the appearance of the carbon dioxide square wave on capnography [19]. An appropriately sized nasogastric tube was passed through the gastric tube channel in all cases.
Following confirmation of bilateral air entry, anaesthesia was maintained using a circle system with a mixture of oxygen, nitrous oxide (1:1 ratio) and isoflurane. Muscle relaxation was achieved with an initial dose of 0.5 mg/kg of atracurium i.v., followed by a maintenance dose of 0.1 mg/kg i.v.. Patients were mechanically ventilated in volume control mode to maintain normocapnia. Baseline parameters, including Heart Rate (HR), Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP), Mean Arterial Pressure (MAP), oxygen saturation and end-tidal carbon dioxide, were monitored and recorded at preinduction, after induction, after I-gel insertion and at 1, 3, 5 and 10 minutes after I-gel insertion.
Statistical Analysis
The data was coded and entered into a Microsoft Excel spreadsheet. Analysis was conducted using IBM Statistical Package for the Social Sciences (SPSS) Statistics version 25.0 for Windows software. Descriptive statistics included the computation of percentages, means and standard deviations. The data were checked for normality before statistical analysis using the Kolmogorov-Smirnov test. The Kruskal-Wallis test was applied for quantitative data to compare two or more observations. The Chi-square test was used for the comparison of qualitative data regarding all clinical indicators. The level of significance was set at p≤0.05.
Results
A total of 36 patients of either gender, aged between 18 and 60 years and belonging to ASA grades I and II, scheduled for elective surgeries and undergoing general anaesthesia, were included in this study. They were randomised into three groups, each receiving a different induction agent: Group-1 received Propofol, Group-2 received Ketofol and Group-3 received Thiopentone. The patients showed demographically comparable data in terms of age, gender and ASA grading [Table/Fig-2].
Comparison of demographic parameters.
| No | Demographic factors | Group-1 | Group-2 | Group-3 | p-value |
|---|
| 1 | Age (in years) | Mean±SD | 34.67±5.97 | 33.25±8.70 | 36±8.48 | 0.89 (NS) |
| 2 | Gender | Female | 7 | 6 | 5 | 0.71 (NS) |
| Male | 5 | 6 | 7 |
| 3 | ASA Grade | I | 5 | 5 | 6 | 0.89 (NS) |
| II | 7 | 7 | 6 |
(Significant: S; Not significant: NS)
The number of patients with an excellent jaw opening score, meaning that their jaws were completely relaxed, was significantly higher in Group-2 than in Groups 1 and 3. The maximum number of attempts of I-gel insertion was observed in Group-3, whereas most patients in Group-2 had the I-gel placed in a single attempt. More than one attempt was required for 10 patients (83%) in Group-3, which was significantly higher than in Group-2, 4 patients (33%) and Group-1, 6 patients (50%). The ease of I-gel insertion was comparable across all three groups. It was slightly more difficult in the Thiopentone group (Group-3), but the difference was not statistically significant. The average duration of insertion was shortest in the Ketofol group at 10.25±0.96 seconds, whereas it was longest in the Thiopentone group at 19.75±2.00 seconds. The difference in duration was statistically highly significant (p<0.0001) [Table/Fig-3].
Comparison of different parameters for ease of insertion.
| No | Parameters (For ease of insertion) | Group-1n (%) | Group-2n (%) | Group-3n (%) | p-value |
|---|
| 1. | Jaw mobility score | 1 | 6 (50%) | 8 (66.7%) | 1 (8.3%) | 0.003 (S) |
| 2 | 6 (50%) | 4 (33.3%) | 6 (50%) |
| 3 | - | - | 5 (41.7%) |
| 4 | - | - | - |
| 2. | Number of attempts | 1 | 6 (50%) | 8 (66.7%) | 2 (16.7%) | 0.04 (S) |
| 2 | 6 (50%) | 4 (33.3%) | 8 (66.7%) |
| 3 | - | - | 2 (16.7%) |
| 3. | Ease of insertion | Easy | 8 (66.7%) | 8 (66.7%) | 6 (50%) | 0.62 (NS) |
| Difficult | 4 (33.3%) | 4 (33.3%) | 6 (50%) |
| 4. | Duration of I-gel insertion in seconds | Mean±SD | 14.92±1.16 | 10.25±0.96 | 19.75±2.00 | 0.0001 (HS) |
(Significant: S; Not significant: NS; Highly significant: HS)
Immediate complications during the insertion of the I-gel, such as coughing and gagging, were observed in eight patients in Group-3 and five patients in Group-1. In contrast, only one patient in Group-2 experienced these complications. However, this difference was not statistically significant. No cases of laryngospasm were reported in any of the three groups [Table/Fig-4].
Comparison of complications post insertion of I-GEL.
| No. | Adverse effects | Group-1n (%) | Group-2n (%) | Group-3n (%) | p-value |
|---|
| 1 | Coughing | 2 (16.7%) | - | 4 (33.3%) | 0.09 (NS) |
| 2 | Gagging | 3 (25%) | 1 (8.3%) | 4 (33.3%) | 0.32 (NS) |
| 3 | Laryngospasm | - | - | - | - |
(Not significant: NS)
The baseline and pre-induction heart rates were comparable across the groups (p-value >0.05). Following induction, the Propofol group exhibited a significant decrease in heart rate (p-value 0.02), while the Ketofol group showed a non significant decline. In contrast, the Thiopentone group experienced a slight increase in heart rate. At the I-gel insertion, all groups showed a significant increase in heart rate (p-value 0.01). Post I-gel insertion, all groups experienced a statistically significant decline in heart rate at 1, 3 and 5 minutes, with Group-1 showing the most significant decrease in heart rate post I-gel insertion (p-value 0.036) [Table/Fig-5].
Comparison of heart rate.
| HR (Beats/min) | Group-1Mean±SD | Group-2Mean±SD | Group-3Mean±SD | p-value |
|---|
| Baseline | 75.67±8.17 | 81.67±7.28 | 76.83±6.24 | 0.11 (NS) |
| Before Induction | 78.33±8.4 | 82.33±6.76 | 78.83±5.75 | 0.07 (NS) |
| After Induction | 75.67±8.48 | 83.33±6.68 | 81.67±5.10 | 0.02 (S) |
| After I-gel insertion | 85.33±8.19 | 92.67±6.95 | 84.83±4.93 | 0.014 (S) |
| 1 min | 83.00±7.98 | 90.67±5.74 | 85.83±4.63 | 0.015 (S) |
| 3 min | 80.50±8.83 | 88.67±6.46 | 82.50±5.98 | 0.015 (S) |
| 5 min | 78.83±7.84 | 84.17±6.46 | 77.33±6.95 | 0.036 (S) |
| 10 min | 76.33±6.81 | 81.67±5.96 | 77.33±6.57 | 0.10 (NS) |
(Significant: S; Not significant: NS)
There was a significant fall in SBP after induction in the propofol and thiopentone groups, while in the ketofol group, a slight increase was observed, followed by a decreasing trend in SBP after I-gel insertion, at 1, 3, 5 and 10 minutes (p<0.05) [Table/Fig-6].
Comparison of Systolic Blood Pressure (SBP).
| Systolic Blood Pressure (SBP) mmHg | Group-1Mean±SD | Group-2Mean±SD | Group-3Mean±SD | p-value |
|---|
| Baseline | 116.67±7.785 | 117.33±8.542 | 116.67±7.152 | 0.097 (NS) |
| Before induction | 118.17±5.006 | 119.17±5.357 | 115.33±5.280 | 0.19 (NS) |
| After induction | 108.67±5.483 | 122.00±5.592 | 113.33±4.849 | 0.001 (HS) |
| After I-gel insertion | 120.83±5.149 | 121.67±5.516 | 110.33±6.485 | 0.001 (HS) |
| 1 min | 117.33±4.924 | 120.33±4.735 | 109.83±7.209 | 0.001 (HS) |
| 3 min | 115.33±4.697 | 117.67±5.245 | 107.50±6.216 | 0.001 (HS) |
| 5 min | 114.00±4.348 | 116.50±4.982 | 108.17±5.219 | 0.001 (HS) |
| 10 min | 111.83±3.243 | 114.00±4.264 | 109.00±4.221 | 0.01 (S) |
(Significant: S; Not significant: NS, Highly significant: HS)
The DBP showed an elevation after induction and after I-gel insertion, which gradually returned to baseline values. This change was highly significant (p<0.001) [Table/Fig-7].
Comparison of Diastolic Blood Pressure (DBP).
| Diastolic Blood Pressure (DBP) mmHg | Group-1Mean±SD | Group-2Mean±SD | Group-3Mean±SD | p-value |
|---|
| Baseline | 71.67±6.02 | 74.83±6.74 | 76.83±6.40 | 0.15 (NS) |
| Before induction | 72.17±6.29 | 76.67±5.14 | 77.33±5.21 | 0.06 (NS) |
| After induction | 74.67±5.93 | 79.83±4.63 | 75.17±5.15 | 0.001 (HS) |
| After I-gel insertion | 73.67±4.81 | 81.67±4.33 | 79.33±4.54 | 0.001 (HS) |
| 1 min | 71.50±4.60 | 80.33±4.65 | 78.17±4.70 | 0.001 (HS) |
| 3 min | 70.00±4.90 | 79.33±5.14 | 77.67±3.90 | 0.001 (HS) |
| 5 min | 70.17±5.69 | 79.17±5.42 | 78.00±2.83 | 0.001 (HS) |
| 10 min | 70.50±5.05 | 78.17±4.13 | 77.33±3.85 | 0.001 (HS) |
(Significant: S; Not significant: NS, Highly significant: HS)
The baseline and pre-induction MAP values were comparable across the groups (p-value >0.05). However, at I-gel insertion and at subsequent time points (1, 3, 5 and 10 minutes post-I-gel), all three groups experienced a decline in MAP, while the ketofol group showed an initial rise followed by a fall in MAP [Table/Fig-8]. Notably, the decrease in MAP was highly significant in Group-1 (p-value=0.0004), significant in Group-3 (p-value=0.02) and non-significant in Group-2 (p-value=0.62).
Comparison of Mean Arterial Pressure (MAP).
| Mean Arterial Pressure (MAP) mmHg | Group-1Mean±SD | Group-2Mean±SD | Group-3Mean±SD | p-value |
|---|
| Baseline | 86.67±5.94 | 89.00±6.21 | 90.11±5.73 | 0.36 (NS) |
| Before induction | 87.50±5.26 | 90.83±4.10 | 90.00±4.32 | 0.19 (NS) |
| After induction | 82.00±5.05 | 93.88±3.27 | 87.88±4.59 | 0.001 (HS) |
| After I-gel insertion | 89.38±4.09 | 95.00±3.84 | 89.66±3.84 | 0.002 (HS) |
| 1 min | 86.77±4.19 | 93.66±4.09 | 88.72±4.24 | 0.001 (HS) |
| 3 min | 85.11±4.08 | 92.11±3.81 | 87.61±4.17 | 0.001 (HS) |
| 5 min | 84.77±4.21 | 91.61±4.29 | 88.05±2.50 | 0.001 (HS) |
| 10 min | 84.27±4.24 | 90.11±3.42 | 87.88±2.69 | 0.001 (HS) |
(Significant: S; Not significant: NS; Highly significant: HS)
From the results shown above, it can be seen that haemodynamic stability was better maintained in the Ketofol group compared to the Propofol and Thiopentone groups as induction agents.
Discussion
In this study, haemodynamic stability was better maintained in the Ketofol group compared to the Propofol and Thiopentone induction agents. All three groups were comparable in terms of age, gender and ASA physical status. These findings are consistent with various other studies [8,10,12,13].
In the present study, the number of patients achieving full jaw opening was significantly higher in the groups receiving Ketofol (66.67%) and Propofol (50%) compared to Thiopentone (8.3%). These results align with previous studies comparing these induction agents. Yousef GT and Elsayed KM, reported better jaw relaxation and full mouth opening in the Ketofol group (90%) compared to the Propofol group (76%) [8]. Excellent LMA insertion conditions were observed in 45 patients in the KP (ketamine-propofol) group and 38 patients in the P (propofol) group. The KP group demonstrated better haemodynamic stability (mean blood pressure, heart rate), which is similar to the findings of this study. Additionally, Saloi DK et al., and Driver I et al., compared Propofol and Thiopentone for ease of LMA insertion and concluded that there was a higher rate of complete jaw opening with Propofol compared to Thiopentone [12,13].
The I-gel was inserted and positioned accurately on the first attempt in 66.7% of patients receiving Ketofol, compared with 50% in patients receiving Propofol and 16.7% in patients receiving Thiopentone. The number of attempts was comparable in Group-1 (Propofol) and Group-2 (Ketofol). However, it was significantly higher in Group-3 (Thiopentone). These findings coincide with the study conducted by Aberra B et al., which compared Ketofol and Propofol for LMA insertion [4].
The total duration of insertion was significantly different among the groups, with Group-2 having the shortest mean time for insertion, at 10.25±0.96 seconds, while Group-3 had the longest mean time (19.75±2.06 seconds) for insertion. These results align with previous studies conducted by Saloi DK et al., and Sengupta J et al., who found a significantly longer insertion time with Thiopentone compared to Propofol and Yousef GT and Elsayed KM, who reported faster induction times with Ketofol compared to Propofol [8,12,14].
Adverse reactions such as coughing and gagging were more frequently observed in Group-3, while they were least common in Group-2. This aligns with the results of earlier studies by Saloi DK et al., Yazdi B et al., and Basunia SR et al., [12,15,16]. While no patients suffered laryngospasm in the current study, this is consistent with the study conducted by Saloi DK et al., [12]. However, the authors believe that a larger sample size could have yielded more meaningful data regarding adverse reactions associated with these induction agents.
There was a fall in heart rate soon after the administration of propofol. However, due to a stress response, there was a modest rise in heart rate at the time of I-gel insertion in all groups. Subsequently, there was a decrease in heart rate at 1, 3, 5 and 10 minutes after propofol and thiopentone were administered. Heart rate variation was not significant in the groups receiving ketofol. Baseline SBP, DBP and MAP were comparable in all three groups in the study. After administering the induction agent and at 1, 3, 5 and 10 minutes after I-gel insertion, there was a statistically significant decrease in SBP, DBP and MAP in the groups receiving propofol and thiopentone. Propofol exhibited a more marked reduction in MAP, as it causes a notable reduction in SBP, potentially due to severe vasodilatation [17,20]. On the other hand, thiopentone (a barbiturate) lowered SBP comparatively less than propofol. Ketofol showed a statistically insignificant rise in MAP compared to the baseline, which eventually approached the baseline, as the presence of ketamine in ketofol counterbalances the hypotensive effect of propofol because of its sympathomimetic effects. Therefore, a higher statistically significant fall in MAP was observed post-induction and further during the study in the propofol and thiopentone groups (p-value <0.002), while haemodynamic stability was maintained by ketofol, which is consistent with many studies [10,21-23]. Additionally, ketamine may activate NMDA receptors either in the vascular endothelium or in the central nervous system. It seems likely that ketamine reduces propofol injection pain due to its local anaesthetic property [24].
Consistent with the results of the present study, Talwar V et al., also observed a decrease in heart rate and arterial blood pressure after the insertion of I-gel in both groups, with a more pronounced drop in the propofol group compared to the thiopentone group [25]. Recently, Ramoliya RV et al., also compared thiopentone and propofol for the insertion of I-gel and proved that propofol provides good insertion conditions and fewer side-effects with a fall in blood pressure compared to thiopentone [26].
A study reported by Yousef GT et al., showed that at every measurement point, mean blood pressure was considerably lower in the propofol group than in the ketofol group (p<0.05) [8]. There was a significant decrease in heart rate (p<0.05) in the propofol group, but the ketofol group experienced heart rate variations similar to the baseline level. Hailu S et al., also found a significant decrease in mean SBP in the propofol group immediately after induction, at 5, 10 and 15 minutes compared to the baseline value; conversely, the ketofol group exhibited no significant changes in mean SBP at any time point compared to baseline [27].
The present study suggests that using ketofol as an induction agent is definitely beneficial in comparison to propofol alone or thiopentone for ease of insertion, relaxation of the jaw, fewer attempts required and faster intubation. Ketofol brings together the features of ketamine and propofol, making it a preferable choice as an induction agent.
Limitation(s)
The limitations of the present study are that it covered a very small group of the population from a single centre, which may limit its generalisability. Secondly, the duration of the study was short, lasting only until 10 minutes post-induction. Thirdly, since only normotensive patients were included, the results might not accurately represent the efficacy and safety in hypertensive patients, for whom attenuation of the intubation response is more important.
Conclusion(s)
Ketofol offers a swift onset of induction and exceptional jaw relaxation, facilitating easier I-gel insertion with fewer attempts compared to propofol and thiopentone. Ketofol can be used as an alternative to propofol and thiopentone induction agents, as it provides superior haemodynamic stability, ease of insertion and a decreased frequency of side-effects such as gagging and coughing.
(Significant: S; Not significant: NS)
(Significant: S; Not significant: NS; Highly significant: HS)
(Not significant: NS)
(Significant: S; Not significant: NS)
(Significant: S; Not significant: NS, Highly significant: HS)
(Significant: S; Not significant: NS, Highly significant: HS)
(Significant: S; Not significant: NS; Highly significant: HS)