Maintaining oral hygiene is important to prevent the deposition of food debris on the tooth surface, which leads to the formation of invisible plaque, acting as a promoting factor for calculus deposition. Ultimately, all these factors lead to the initial stage of inflammation of the periodontium, i.e., gingivitis, and if left untreated, this can progress to periodontitis [1-4]. Therefore, maintaining oral hygiene with proper brushing techniques is essential for improving the oral health status of children.
Vision is one of the most important senses for interpreting the world around us. If, vision is impaired during childhood, it can have detrimental effects on the physical, cognitive, neurological, and emotional development of the child. Over 1.4 million children worldwide are estimated to be living with visual impairment [5]. Visually impaired children may have poor oral hygiene due to several factors, such as diet, eating patterns, lack of cleaning habits, poor eye-hand co-ordination, or physical dexterity [6]. Thus, awareness of dental health is essential, as it can promote both oral health and general health maintenance [7].
In visually impaired children, oral illnesses may be difficult to diagnose, and adherence to care may be low. The most common method for maintaining oral hygiene in visually impaired children is by using the Braille system (1827, Louis Braille). As visually impaired children face challenges in learning daily skills, a specific form of health education known as ATP was developed. This is a powerful communication tool for teaching these children the correct technique for brushing to maintain good oral hygiene [8].
Effective tooth brushing with proper technique using dentifrice can significantly impact a child’s daily routine activities, such as eating habits, speaking, mouth cleaning, relaxing, maintaining emotional well-being, smiling, schoolwork, and social interactions, which ultimately improves overall outcomes [9-12]. Several tooth brushing techniques are widely accepted and used, such as the Modified Bass and Fones techniques; however, no study has been conducted to date that depicts the effect of the ATP technique with different brushing techniques on children’s oral health and hygiene with a large sample size.
Hence, the present study aimed to evaluate the oral hygiene status by comparing the Braille and ATP techniques with the Fones method and the ATP technique with the Modified Bass technique of tooth brushing, using conventional dentifrice in visually impaired children aged 6-12 years, to determine which method is best suited to maintain acceptable levels of oral hygiene.
Materials and Methods
The prospective interventional study was conducted by the Department of Paediatric and Preventive Dentistry at SGT University, Gurugram, Haryana, India involving 300 blind school children aged 6-12 years from New Delhi-NCR. The study took place over a period of one year and six months, starting in November 2018 and ending in February 2020, after obtaining ethical clearance with Institutional Ethical Committee (IEC) number SGTU/FDS/MDS/24/1/519.
Inclusion criteria: The inclusion criteria included visually impaired children aged 6-12 years without any associated disabilities or systemic diseases, classified as H-54.0- Biocular blind according to the International Statistical Classification of Diseases by the World Health Organisation (WHO) [13]. Participants were recruited from two different schools: the Blind Relief Association in New Delhi and Captain Chandan Lal Special Middle School for the Blind in Gurugram. Permission was obtained from the school management.
Exclusion criteria: The exclusion criteria involved children with uniocular blindness, biocular blindness with any other systemic disease, physical or mental disabilities, and parents/caretakers/visually impaired children who were unwilling to participate in this study.
Sample size: A sample size of 300 was selected based on a convenient sampling method and the children were divided into three groups, each containing 100 children, using the chit method for randomisation.
Study Procedure
The study was conducted in four stages:
First stage: Engaging session.
Second stage: Noting down the Oral Hygiene Index-simplified (OHI-S) [8] scores during the baseline examination.
Third stage: Demonstrating the brushing methods.
In group 1, oral health education was delivered using Braille, a traditional approach to educate the visually impaired. A Braille slate was prepared with a set of instructions engraved as follows: a) brush twice a day with a soft toothbrush (morning and night); b) rinse the mouth after every meal; c) limit sugar consumption; d) consume more fibrous diets; e) have consistent dental check-ups every six months with the help of school staff to maintain good oral hygiene.
In group 2 and group 3, children were trained using the ATP technique with the Fones brushing method and the ATP technique with the Modified Bass brushing method, respectively [8]. The ATP technique includes three components: audio, tactile, and performance [15]. Children were first verbally informed about the importance of teeth and the method of brushing (Audio). They were then allowed to feel the teeth on a large-sized model (Tactile) and were taught to brush on the model with support. They were encouraged to feel their own teeth with their tongues, and any deposits present were marked by the feeling of roughness.
Finally, the children were taught to brush their own teeth with assistance (Performance). They practiced the Fones and Modified Bass Techniques first on a model and then on their own teeth. This process was repeated until the children could perform it independently.
Postoperatively, OHI-S scores were recorded for all groups during follow-up visits at 1, 3, 6, 9, and 12 months. Based on the mean OHI-S scoring of (≤0.9)-Good, (1.0-1.9)-Fair, and (≥2)-Poor oral hygiene, the results were analysed [8].
Statistical Analysis
Statistical analysis was conducted using SPSS version 21.0. Intergroup comparisons of oral hygiene status were performed for the three different brushing techniques, and the data were analysed statistically using the Post-hoc test with Bonferroni correction. A p-value less than 0.05 were considered significant.
Results
The study sample comprised 300 visually impaired children. Among these children, 283 were males and 17 were females, all within the age group of 6 to 12 years. The mean age was 8.58±1.297 years.
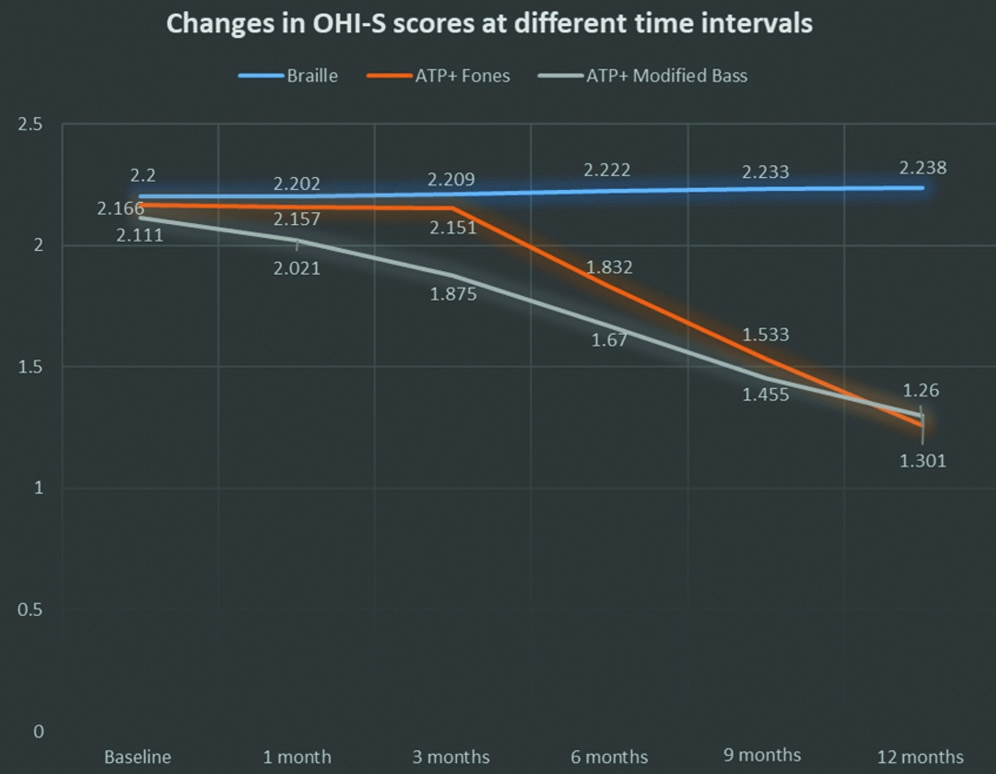
The mean OHI-S scores in three groups at baseline examination and at 1, 3, 6, 9, and 12 months follow-up visits after intraoral examination are shown in [Table/Fig-1,2]. The graphical representation of the mean OHI-S scores at different time intervals has been depicted in [Table/Fig-2].
Mean OHI-S scores (Mean±SD) in three groups at baseline examination and at 1, 3, 6, 9 and 12 months follow-up visits after intraoral examination.
| Study groups | Mean OHI-S scoring (Mean±SD) |
|---|
| Baseline examination | 1 month | 3 months | 6 months | 9 months | 12 months |
|---|
| Group 1 (Braille) | 2.200±0.668 | 2.202±0.633 | 2.209±0.474 | 2.222±0.481 | 2.233±0.889 | 2.238±0.765 |
| Group 2 (ATP+Fones) | 2.166±0.664 | 2.157±0.612 | 2.151±0.485 | 1.832±0.420 | 1.533±0.843 | 1.260±0.752 |
| Group 3 (ATP+Modified Bass) | 2.111±0.649 | 2.021±0.601 | 1.875±0.487 | 1.670±0.367 | 1.455±0.796 | 1.301±0.725 |
The graph depicts changes in the mean OHI-S scores at 1, 3, 6, 9 and 12 months.
At baseline and at one month, the mean differences between the groups were statistically insignificant [Table/Fig-3]. However, at three months, the mean differences between group 1 (Braille) and group 3 (ATP + Modified Bass), as well as between group 2 (ATP + Fones) and group 3 (ATP + Modified Bass), were statistically significant. Similarly, at 6, 9, and 12 months, the mean differences between group 1 (Braille) and group 3 (ATP + Modified Bass), as well as between group 2 (ATP + Fones) and group 1 (Braille), were statistically significant [Table/Fig-3].
Pair-wise comparison of mean OHI-S scores at baseline examination and at 1, 3, 6, 9 and 12 months follow-up visits after intraoral examination between the 3 groups.
| Dependent variable | Mean difference (I-J) | Sig. |
|---|
| Baseline examination | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.034 | 1.000 |
| Group 3 (ATP+Modified Bass) | 0.089 | 1.000 |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.055 | 1.000 |
| 1 month | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.045 | 1.000 |
| Group 3 (ATP+Modified Bass) | 0.181 | 0.182 |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.136 | 0.475 |
| 3 months | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.058 | 1.000 |
| Group 3 (ATP+Modified Bass) | 0.334 | 0.001* |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.276 | 0.010* |
| 6 months | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.390 | <0.001* |
| Group 3 (ATP+Modified Bass) | 0.552 | <0.001* |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.162 | 0.220 |
| 9 months | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.700 | <0.001* |
| Group 3 (ATP+Modified Bass) | 0.778 | <0.001* |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.078 | 1.000 |
| 12 months | Group 1 (Braille) | Group 2 (ATP+Fones) | 0.978 | <0.001* |
| Group 3 (ATP+Modified Bass) | 0.937 | <0.001* |
| Group 2 (ATP+Fones) | Group 3 (ATP+Modified Bass) | 0.041 | 1.000 |
*Denotes statistically significant using Post-hoc test-Bonferroni correction
Discussion
Braille is an important tool for visually impaired children to learn various activities. In this context, Khurana C et al., conducted a non randomised controlled trial stating that children with visual impairments could maintain an acceptable level of oral hygiene when instructed using the Braille system for education [16]. Conversely, in a non randomised controlled study by Tiwari BS et al., it was concluded that the Braille method was the least effective in maintaining good oral health, as it showed the smallest reduction in mean plaque scores compared to other control groups [17].
The ATP technique, combined with different brushing methods, is used to teach and maintain oral hygiene in these children, including methods such as Horizontal Scrub, Fones, Roll Method, Modified Bass, Stillman, and Charter’s Method.
In the present study, the intergroup comparison of the mean OHI-S score at baseline examination across all three groups did not reveal a statistically significant difference. Braille, being the standard method for teaching visually impaired children, was used to provide oral hygiene instructions in group 1, aiming to help the children maintain their oral hygiene. However, there were no signs of improvement in the mean OHI-S values. Therefore, the Braille method used in group 1 was found to be insufficient for improving the oral hygiene status.
This was in contrast to a study conducted by Gautam K et al., in which a notable decrease in the plaque index (p<0.01) was observed when visually impaired children were educated using Braille slates [18].
At six months and 12 months, the mean OHI-S difference between group 1 (Braille) and group 2 (ATP+Fones) was statistically significant, with mean OHI-S differences of 0.390 and 0.978, respectively (p-value <0.001).
Deshpande S et al., conducted a study in 2017, which yielded similar significant results, with a p-value <0.001 for the Fones brushing method compared to the Braille method, thus demonstrating the superior efficacy of the Fones method over Braille instructions [19].
At 6 months and 12 months, intergroup comparisons revealed that the mean OHI-S difference between group 1 (Braille) and group 3 (ATP + Modified Bass) was statistically significant, with mean OHI-S differences of 0.552 and 0.937, respectively (p-value <0.001). There is no supporting literature that compares Braille instructions and the Modified Bass method in reducing plaque scores. In group 2 (ATP + Fones) and group 3 (ATP + Modified Bass), the difference between mean OHI-S scores did not show a statistically significant difference. This is consistent with a study by Harnacke D et al., which concluded that during the follow-up visits, the Fones method is superior to the Modified Bass approach and is more easily understood, recalled, and enjoyable for visually impaired children [20]. Similar results were seen in studies conducted by Joybell C et al., Sreedevi S and Shivaprakash PK and Tiwari BS [8,13,17].
In present study, as observed from the results, ATP with Fones and the Modified Bass method are the best guided brushing techniques in comparison to the conventional brushing method (Braille) for these children. These techniques can be documented in school dental health programs and should be practiced, easily guided by their parents/caretakers, and accepted by visually impaired children for better maintenance of oral hygiene in the Indian context. This aligns with a study conducted by Chowdary PB et al., which found that a combination of verbal Braille and tactile instructions resulted in a greater reduction in mean plaque scores at the six-month follow-up compared to the first and third month follow-up visits [21]. Studies with larger sample sizes are required to further validate the techniques used. More research needs to be conducted to evaluate and compare the observations further.
Limitation(s)
The present study had a few limitations. Children between the ages of 6 to 12 years differ in their cognitive abilities and manual dexterity, which are necessary for performing tooth brushing methods. Since tooth brushing is a fine motor activity, children with visual impairments may perform it completely without assistance. Additionally, the time taken by each child to brush their teeth every day varies and can also be considered a limitation of the present study. Studies with a larger sample size are required to further validate the techniques used. More research needs to be conducted to evaluate and compare these methods.
Conclusion(s)
Group 2 (ATP with the Fones method) and group 3 (ATP with the Modified Bass method) demonstrated superior results in reducing mean plaque scores from baseline to the 12-month follow-up visit compared to group 1 (Braille method), reflecting the higher efficacy of the ATP technique in comparison to Braille instructions. Additionally, group 3 showed slightly better results than group 2, although the differences were statistically insignificant.
*Denotes statistically significant using Post-hoc test-Bonferroni correction