Moebius Syndrome Misdiagnosed as Duane Retraction Syndrome: A Case Report
Harnoor Kaur1, Neha K Sethi2, Harsimarpreet Singh3
1 Junior Resident, Department of Ophthalmology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India.
2 Associate Professor, Department of Ophthalmology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India.
3 Junior Resident, Department of Ophthalmology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Neha K Sethi, Department of Ophthalmology, Guru Gobind Singh Medical College and Hospital, Faridkot-151204, Punjab, India.
E-mail: neha.knew@gmail.com
Moebius syndrome and Duane Retraction Syndrome (DRS) are Congenital Cranial Dysinnervation Disorders (CCDDs) characterised as congenital, non progressive groups of diseases caused by abnormal development of cranial nerve nuclei or their axonal connections. Due to their overlapping features, distinguishing between these disorders can be challenging, leading to potential diagnostic oversights. This is a case report of a 10-year-old female with Moebius syndrome misdiagnosed as DRS. She had 6th and 7th nerve palsies with exposure keratopathy. Probably the cause for misdiagnosis was the presence of an abduction deficit-a characteristic shared by both disorders. Additionally, it is crucial to examine the facial nerve, as it is exclusively affected in Moebius syndrome. DRS is significantly more common than Moebius syndrome; the rarity of Moebius syndrome might contribute to the misdiagnosis. Conducting a thorough examination is essential for differentiating between these conditions, thereby facilitating comprehensive management.
Congenital cranial dysinnervation disorders, Congenital facial palsy, Exposure keratopathy, Strabismus
Case Report
The 10-year-old female, diagnosed with left-eye (OS) DRS since five years, presented to the ophthalmology OPD for the first time with OS diminution of vision, watering, redness, and long-standing inability to close her left eye. The patient was systemically stable. There was no significant family or past history. Her Best Corrected Visual Acuity (BCVA) was 6/9 and 6/36 in the right eye (OD) and left eye (OS) respectively. OS had uncorrected hypermetropia of +2.75D with anisometropic amblyopia. The anterior segment examination was normal except in OS, showing Superficial Punctate Keratopathy (SPK). Intraocular pressure and fundus examination were normal in both eyes (OU).
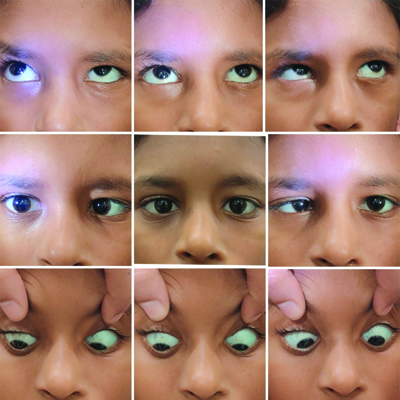
OU abduction was restricted and suggestive of abducens nerve palsy; the visual axis was parallel in the primary gaze. Palpebral fissure height was the same in both abduction and adduction in both eyes; and importantly there was no globe retraction on adduction or abduction as shown in [Table/Fig-1]. OS had lagophthalmos, poor Bell’s phenomenon, mild corneal exposure keratopathy, and SPK on the cornea inferiorly in the left eye. She had a mask-like facial appearance. Examination of the seventh nerve revealed left facial palsy- no forehead furrows, no forehead wrinkling on the left-side, inability to close the left eye against resistance, deviation of the angle of the mouth to the right-side as shown in [Table/Fig-2]. The rest of the central nervous system, cranial nerve, and systemic examination were normal. The Magnetic Resonance Imaging (MRI) of her brain was also normal.
Nine cardinal positions of gaze showing restriction in abduction and normal palpebral fissure height with no globe retraction.
Tests of facial nerve were suggestive of left facial palsy: (a) Deviation of angle of mouth towards right-side with absence of the nasolabial fold on left-side of face while smiling; (b) Incomplete closure of left eye.

The diagnosis of the patient was revised as Moebius Syndrome as she had bilateral sixth and left seventh nerve palsy. She improved with medical treatment for exposure keratopathy including lubricants (eyedrop carboxymethylcellulose 0.5%- QID), antibiotics (eyedrop moxifloxacin 0.5%-TDS), and night eye-taping. After one week of treatment, she had no SPK, decreased congestion, and vision improved to 6/24.
Discussion
Authors report a case of Moebius syndrome (with OS facial and bilateral abducens palsy) misdiagnosed as OS DRS. Moebius syndrome is a congenital condition characterised by unilateral or bilateral facial and abducens nerve palsy with an incidence of 1 in 250,000; most often sporadic [1,2]. Patients suffering from this rare disease present with mask-like faces, deviation of the angle of the mouth, especially during smiling, lagophthalmos with or without exposure keratopathy, horizontal gaze palsies with intact vertical gaze, and normal palpebral fissure height with horizontal eye movements. It may also involve other cranial nerves, neurodevelopmental abnormalities of the limb and pectoral region, and autism [2].
On the other hand, DRS is a congenital complex strabismus with an incidence of 1 in 10,000; 10% of cases are familial [1]. It is characterised by a limitation of abduction or adduction of the eye (most commonly type 1 DRS with abduction limitation), retraction of the eyeball, and shortening of the palpebral fissure on attempted adduction due to co-contraction of horizontal recti [1,3].
A major difference between Moebius syndrome and DRS is the presence of facial palsy in Moebius syndrome while the 7th nerve is unaffected in DRS. It is postulated that the cause of misdiagnosis was the abduction deficit in both eyes, which is a common feature of Moebius syndrome and type 1 DRS (the most common type). Additionally, the failure to determine the patient’s facial nerve function, DRS being much more common than Moebius syndrome, and the probable ignorance of Moebius syndrome (which is rare) on the part of the previous treating ophthalmologist may have contributed to the misdiagnosis [4]. Also, although the vertical palpebral fissure height was constant in horizontal gazes, OS lagophthalmos was mistakenly interpreted as OD retraction in present case patient.
The management of both Moebius syndrome and DRS depends on the severity of squint. Strabismus surgery can help provide a parallel visual axis in at least the primary position with the surplus goal of improvement of visual motility in horizontal gazes. For Moebius syndrome, ocular management should additionally include prevention and treatment of exposure keratopathy due to associated 7th nerve palsy. Furthermore, support from a neurologist, paediatrician, plastic surgeon, counsellor, and physiotherapist is also required for managing the non ocular manifestations of the disease [5-7]. This latter aspect of management is likely to be neglected if such a misdiagnosis is made. [Table/Fig-3] summarises the differences between Moebius syndrome and DRS [1-4,6,8].
Summarises the differences between Moebius syndrome and Duane Retraction Syndrome (DRS) [1-4,6,8].
| Feature | Moebius syndrome | Duane retraction syndrome |
|---|
| Frequency | 1 in 250,000; most often sporadic [1,2] | 1 in 10,000; 10% cases familial [1] |
| Age at diagnosis | Often earlier (2-11 years) maybe due to mask like facies | Often in teens [6] |
| Overlapping symptoms and signs | Esotropia in primary gaze | Esotropia more in adduction but in severe cases in primary gaze also (in DRS Type-1) |
| Saliant feature | Facial palsy due to 7th nerve involvement; mask like facies, lateral rectus palsy | In 80% cases, abduction is limited (type 1), in 20% cases adduction or both adduction and abduction may be limited; globe retraction |
| Palpebral fissure height | No change in horizontal gazes | Narrowing on attempted horizontal eye movements |
| Cranial nerve involvement | 6th and 7th nerve most commonly involvedRarely-3rd, 4th, 9th and 12th | Aplasia of 6th nerve nucleus and aberrant lateral rectus innervation by 3rd nerve |
| Bilaterality | Facial nerve involvement- 97% bilateral [4] | Unilateral in upto 80% cases, often left-sided [3] |
| Abduction | Limited | Limited (in 80% cases) |
| Additional features | Developmental delay, musculoskeletal malformations, neurological disorders, mental retardation, problems with endocrine and respiratory system [8] | Other ocular findings- nystagmus, anisocoria, ptosis, congenital cataract, optic nerve hypoplasiaGustatory lacrimal reflex or crocodile tears |
Conclusion(s)
Moebius syndrome (being a rare disorder) and DRS (relatively more common) may have overlapping clinical features, like abduction deficit. Therefore, a thorough examination, especially of facial nerve function, can help clinch the diagnosis and form the basis for comprehensive management of Moebius syndrome. The statement above reports a case of Moebius syndrome misdiagnosed as DRS.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jul 04, 2024
Manual Googling: Jul 26, 2024
iThenticate Software: Sep 09, 2024 (10%)
[1]. Gutowski NJ, Chilton JK, The congenital cranial dysinnervation disordersArch Dis Child 2015 100:678-81.10.1136/archdischild-2014-30703525633065 [Google Scholar] [CrossRef] [PubMed]
[2]. Zaidi SMH, Syed IN, Tahir U, Noor T, Choudhry MS, Moebius syndrome: What we know so farCureus 2023 15(2):e3518710.7759/cureus.35187 [Google Scholar] [CrossRef]
[3]. Gaballah KA, Shawky D, Treatment modalities in Duane’s Retraction SyndromeInt J Ophthalmol 2020 13(1):278-83.10.18240/ijo.2020.02.1232090038 [Google Scholar] [CrossRef] [PubMed]
[4]. Assaf AA, Congenital innervation dysgenesis syndrome (CID)/congenital cranial dysinnervation disorders (CCDDs)Eye (Lond) 2011 25(10):1251-61.10.1038/eye.2011.3821720410 [Google Scholar] [CrossRef] [PubMed]
[5]. Ali MH, Jamal S, Rashid MA, Javaid U, Butt NH, Moebius syndrome with hypoglossal palsy, syndactyly, brachydactyly, and anisometropic amblyopiaCureus 2018 10(3):e233410.7759/cureus.2334 [Google Scholar] [CrossRef]
[6]. Kekunnaya R, Gupta A, Sachdeva V, Krishnaiah S, Venkateshwar Rao B, Vashist U, Duane retraction syndrome: series of 441 casesJ Pediatr Ophthalmol Strabismus 2012 49:164-69.10.3928/01913913-20111101-0122074356 [Google Scholar] [CrossRef] [PubMed]
[7]. Souni G, Ayad G, Elouali A, Babakhouya A, Rkain M, Moebius syndrome: A case report on an uncommon congenital syndromeCureus 2023 15(6):e4074610.7759/cureus.40746 [Google Scholar] [CrossRef]
[8]. Chowdhury S, Sarkar S, Guha D, Dasgupta MK, Moebius syndrome: A rare entity or a missed diagnosis?J Pediatr Neurosci 2020 15(2):128-31.10.4103/jpn.JPN_72_1933042246 [Google Scholar] [CrossRef] [PubMed]