Notorious Foreign Body in the Cricopharynx with Impending Internal Carotid Artery Penetration: A Case Report
K Gowthame1, Raghvi Anand2, RB Namasivaya Navin3, S Prabakaran4, B Sarath Kumar5
1 Assistant Professor, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
2 Senior Resident, Department of Ear, Nose and Throat, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
3 Assistant Professor, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
4 Associate Professor, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
5 Senior Resident, Department of Ear, Nose and Throat, Chettinad Hospital and Research Institute, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. B Sarath Kumar, Chettinad Hospital, OMR, Kelambakkam, Chennai-603103, Tamil Nadu, India.
E-mail: sarathkumarbalan@gmail.com
The presence of foreign bodies in the throat is a relatively frequent occurrence in otolaryngology practice. Adults experience foreign bodies in their throats more frequently, with food impaction being the main reason. A 60-year-old female presented with a history of fish ingestion and complaints of Foreign Body (FB) sensation in the throat and painful swallowing. Computed Tomography (CT) of the neck showed the presence of a FB in the hypopharynx, with a possibility of penetration into the parapharyngeal space and the left Internal Carotid Artery (ICA). The patient underwent FB removal under flexible fibreoptic endoscopy with intravenous sedation. Any delay in diagnosis and treatment could lead to the migration of the FB into the carotid artery, resulting in catastrophic bleeding. Hence, every patient who visits the otolaryngology Outpatient Department (OPD) with complaints of FB sensation in their throat needs to be evaluated promptly. Physicians should be particularly concerned if the patient has prolonged clinical symptoms, positive neck radiography, and negative direct laryngoscopy and rigid esophagoscopy. These cases have a high index of suspicion for a migrating FB. Whether to consider segmental resection and end-to-end anastomosis, angioplasty with a saphenous vein or prosthetic patch, insertion of an allograft, Polytetrafluoroethylene (PTFE) interposition graft, or replacement of the injured ICA will depend on the type and extent of the arterial injury.
Polytetrafluoroethylene graft, Prosthetic patch, Proton pump inhibitors, Segmental resection
Case Report
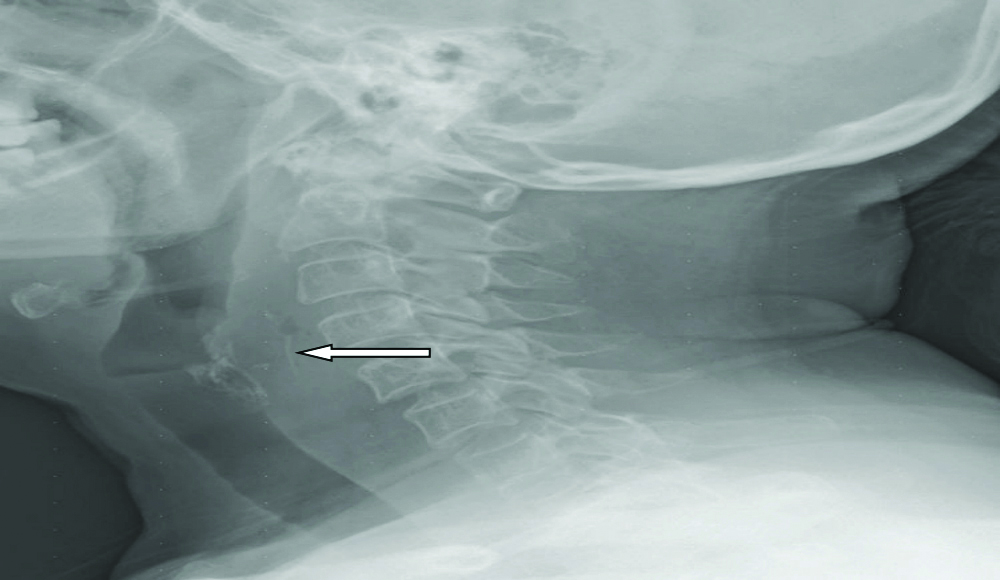
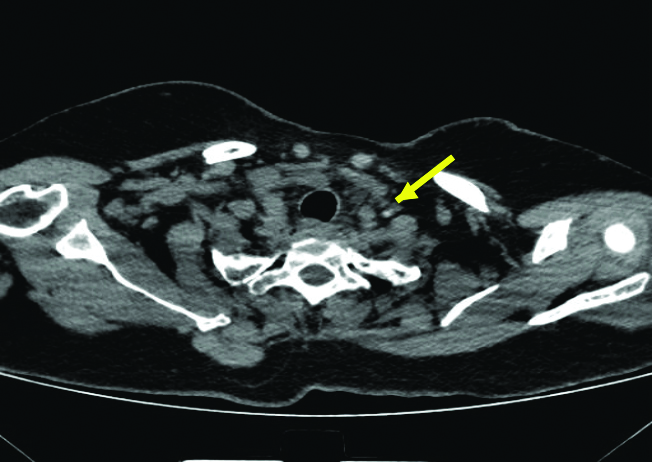
A 60-year-old female presented to the Ear, Nose and Throat (ENT) Outpatient Department (OPD) with a history of tilapia fish ingestion two days prior and complaints of a FB sensation in her throat and painful swallowing for the same duration. She did not report any haemoptysis or difficulty in breathing. Her blood pressure was 120/80 mmHg, respiratory rate was 16 breaths per minute, and SpO2 was 100% on room air. Video laryngoscopy was normal. No FB was visualised. The mobility of both vocal cords was normal. An X-ray of the soft-tissue in the neck (lateral view) showed a soft-tissue opacity in the postcricoid region, along with widening of the prevertebral space [Table/Fig-1]. A CT scan of the neck revealed the presence of a FB (fishbone) in the hypopharynx, with a possibility of penetration into the parapharyngeal space and the left ICA [Table/Fig-2].
Radiograph showing a lateral view of the neck’s soft-tissue depicting the hypopharynx’s prevertebral space widening (arrow).
CT neck with fish bone (white dot) in hypopharynx with impending Internal Carotid Artery (ICA) penetration. The ICA is present in the region, pointed out by the arrow.
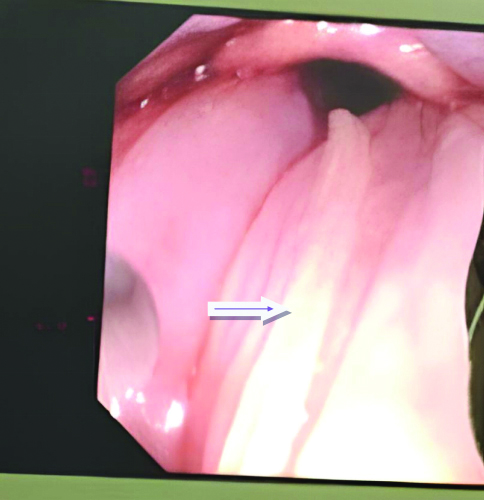
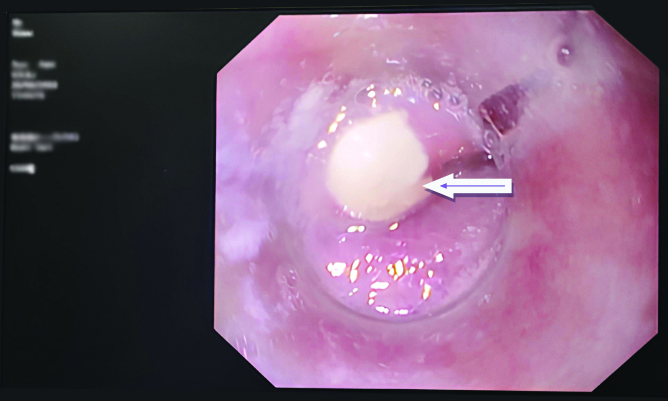
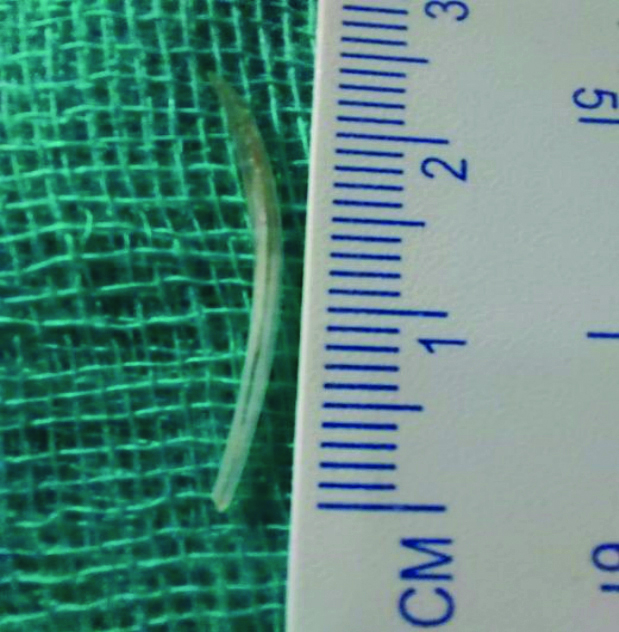
The patient was taken for surgery after receiving fitness clearance for anaesthesia. She underwent FB removal under flexible fibreoptic endoscopy with intravenous sedation. The fishbone was visualised in the postcricoid region and was removed using rat-tooth forceps [Table/Fig-3]. An ulcer was observed in the region where the FB had been lodged [Table/Fig-4]. [Table/Fig-5] shows the removed fishbone, which measured approximately 2.4 cm. Haemostasis was maintained throughout the procedure.
Fishbone (arrow) in postcricoid region being grasped by rat toothed forceps.
Ulcer in the region where the fishbone was lodged.
Fish bone after removal measuring around 2.4 cm.
The patient was initially kept NPO (nothing by mouth) and was on nasogastric tube feeds on the day of surgery to prevent infection of the ulcer. Postoperatively, the patient was treated with intravenous steroids, fluids, antibiotics, analgesics, and Proton Pump Inhibitors (PPIs) to prevent gastric ulcers. She was gradually started on oral liquids the following day and a soft solid diet after two hours of oral liquids. She improved symptomatically, and there was no evidence of fever or tachycardia. The patient was discharged the next day and reviewed after one week, with weekly follow-ups for a month. She had no complaints postprocedure and was now symptomatically better and stable.
Discussion
In adults, FB in the throat are more common, with most cases occurring because of food impaction. Fish bones, mutton bones, and fragments of meat are among the most prevalent types of foreign bodies found in adults [1]. Sometimes, the FB can migrate extraluminally and affect significant structures in the neck and other neighbouring structures [2,3]. Present case was a rare presentation of the FB (fish bone) getting stuck in the hypopharynx, with radiological findings suggestive of possible penetration ICA. Foreign bodies are a frequent cause of morbidity and mortality in the aerodigestive tract at both extremes of the lifespan. Particularly during the first six years of life, children are more prone to eating and aspirating FBs [4]. However, in adults, FB ingestion generally occurs while eating, which causes either bone impaction or meat impaction because of weak dentition, artificial dentures, and insufficient chewing [5].
Adults with psychiatric disorders, mental retardation, alcohol-induced inebriation, trauma-related decreased awareness levels, and impaired airway reflexes are more likely to encounter FB aspiration. Dentures, coins, fish bones, and even tiny pieces of glass have been discovered in the digestive tract [6]. FB impaction usually occurs at the cricopharyngeal junction, while other frequent locations for FB impaction include the oropharynx, hypopharynx, and thoracic oesophagus. Accidental foreign object ingestion, such as a fish bone or chicken bone, can result in an FB getting lodged in the cervical oesophagus or hypopharynx. On a lateral X-ray of the neck, the bones are often under-calcified and difficult to see. It must be remembered that bone impaction-related soft-tissue oedema takes 3-12 hours to appear and might not be apparent if the patient is X-rayed right away. According to Street I these individuals exhibit neck swelling, odynophagia, prevertebral soft-tissue swelling on X-ray, symptoms of septicaemia, and retropharyngeal abscess if an early diagnosis is not obtained [7]. To avoid morbidity, prompt detection and removal of FBs is essential.
The FBs can migrate extraluminally and affect significant structures in the neck, gastrointestinal tract, and other neighbouring structures. Chee LW and Sethi DS showed that a delay in detecting fish bone impaction is typically caused by negative laryngoscopy and visual examination, resulting in a low rate of radiolucent fish bone being detected on the lateral radiograph of the neck [8]. Due to their low sensitivity, X-rays of the neck are prone to overlooking thin fish bones. According to Hussain SZ et al., a CT scan performed before endoscopy would help to precisely define the position (both intraluminal and extraluminal) and level of impaction or perforation, assisting us during the endoscopy [9].
The migration of fish bones extraluminally can result in deep neck abscesses (retropharyngeal, parapharyngeal abscesses), vascular complications such as oesophageal fistulas (aorta-oesophageal, innominate artery-oesophageal fistulas), puncture of the carotid artery, thromboembolism, brachial plexus injury, and retention of the FB in the thyroid gland [10]. Several mechanisms are implicated in the migration of the FB to the extraluminal region, including the fish bone’s thin orientation and pointed shape, the contraction of the cricopharyngeus muscle during swallowing or the movement of muscles in the neck, localised inflammation of the oesophagus and pharyngeal wall, and direct pressure necrosis. It is necessary to locate and surgically remove the migrating fish bone [11]. If there is an abscess, it must be drained. The management of a migrating fish bone can be difficult and frequently calls for multidisciplinary teamwork. A neck exploration surgery under general anaesthesia by a transverse cervical incision may be necessary in cases of migration of fish bone [11].
Present case was a rare instance of the FB getting stuck in the hypopharynx, with radiology suggesting possible ICA penetration. A quick evaluation was done, and the FB was removed using flexible fibreoptic endoscopy under intravenous sedation. The impending ICA penetration posed a significant threat to index patient, which was managed efficiently. Fortunately, there was no major bleeding. To avoid complications, a quick blood panel was conducted, reserved adequate blood, and promptly removed the fish bone. The backup of the vascular surgeon team and materials for vascular repair and grafting was also there in case it became necessary.
Conclusion(s)
This case report, involving a fishbone that was impeding the ICA, was efficiently managed early, thus preventing catastrophic bleeding and other complications mentioned. Therefore, every patient who visits the ENT-OPD with complaints of FB sensation in the throat needs to be thoroughly evaluated. The FB may not always be visible in all scenarios on video laryngoscopy or soft-tissue neck X-ray, which can present a challenge. Depending on the patient’s age, health, nature of the FB, and other factors, the FB should be quickly detected, located, and removed either under local or general anaesthesia.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 28, 2024
Manual Googling: Jul 15, 2024
iThenticate Software: Aug 26, 2024 (9%)
[1]. O’Flynn P, Simo R, Fish bones and other foreign bodiesClin Otolaryngol Allied Sci 1993 18(3):231-33.10.1111/j.1365-2273.1993.tb00837.x8365016 [Google Scholar] [CrossRef] [PubMed]
[2]. Jamal S, Irfan M, Nazim N, Spontaneous extrusion of migrated fish bone in the neck after 48 hours of ingestionBangladesh J Med Sci 2011 10(2):12910.3329/bjms.v10i2.7809 [Google Scholar] [CrossRef]
[3]. Goh YH, Tan NG, Penetrating esophageal foreign bodies in the thyroid glandJ Laryngol Otol 1999 113:769-71.10.1017/S002221510014516510748860 [Google Scholar] [CrossRef] [PubMed]
[4]. Bane A, Bekele A, Management of gastrointestinal foreign bodies using flexible endoscopy: An experience from Addis Ababa, EthiopiaEast and Central African J Surg 2012 17(3):32-38. [Google Scholar]
[5]. Triadafilopoulos G, Roorda A, Akiyama J, Update on foreign bodies in the esophagus: Diagnosis and managementCurr Gastroenterol Rep 2013 15:01-06.10.1007/s11894-013-0317-523435762 [Google Scholar] [CrossRef] [PubMed]
[6]. Parajuli R, Foreign bodies in the ear, nose and throat: An experience in a tertiary care hospital in central NepalInt Arch Otorhinolaryngol 2015 19(2):121-23.10.1055/s-0034-139733625992166 [Google Scholar] [CrossRef] [PubMed]
[7]. Street I, Infections and foreign bodies in the ear, nose and throatSurgery (Oxford) 2009 27(12):518-22.10.1016/j.mpsur.2009.09.013 [Google Scholar] [CrossRef]
[8]. Chee LW, Sethi DS, Diagnostic and therapeutic approach to migrating foreign bodiesAnn Otol Rhinol Laryngol 1999 108(2):177-80.10.1177/00034894991080021310030237 [Google Scholar] [CrossRef] [PubMed]
[9]. Hussain SZ, Kk A, Mohammad AW, Khan M, Migratory foreign bodies in the aerodigestive tract: The importance of CT imagingCureus 2022 14(1):e2159510.7759/cureus.21595 [Google Scholar] [CrossRef]
[10]. Castan Senar A, Dinu LE, Artigas JM, Larrosa R, Navarro Y, Angulo E, Foreign bodies on lateral neck radiographs in adults: Imaging findings and common pitfallsRadiographics 2017 37(1):323-45.10.1148/rg.201716007328076010 [Google Scholar] [CrossRef] [PubMed]
[11]. Johari HH, Khaw BL, Yusof Z, Mohamad I, Migrating fish bone piercing the common carotid artery, thyroid gland and causing deep neck abscessWorld J Clin Cases 2016 4(11):37510.12998/wjcc.v4.i11.37527900327 [Google Scholar] [CrossRef] [PubMed]