Haemothorax, characterised by blood in the pleural cavity with a haematocrit greater than 50%, can arise from both traumatic and non traumatic causes. Prompt blood removal is crucial to prevent coagulation and complications like post-traumatic empyema. While tube thoracostomy is the initial management, Intrapleural Fibrinolytic Therapy (IPFT) offers a less invasive alternative when drainage is insufficient. The authors hereby, report the case of a 33-year-old male with congenital heart disease who presented with haemothorax. He exhibited worsening breathlessness, a cough with yellowish sputum and intermittent fever. Examination revealed clubbing, tachycardia, hypotension, tachypnoea and hypoxia. Imaging confirmed a right-sided pleural effusion with septations and severe Pulmonary Arterial Hypertension (PAH). Initial management with a pigtail catheter and antibiotics resulted in minimal drainage. The patient then underwent IPFT, leading to significant fluid drainage and radiological improvement. His clinical condition improved with reduced breathlessness and stabilised vital signs. The present case supports the efficacy of fibrinolytic agents like Streptokinase (STK) in managing clotted haemothorax, particularly in patients with complex medical backgrounds such as congenital heart disease. Early IPFT can enhance pleural drainage and reduce the need for invasive surgery, highlighting its value in similar clinical scenarios.
Case Report
A 33-year-old male office clerk, with a known history of congenital heart disease and a potential recipient for a heart and lung transplant, presented to the Emergency Department with breathlessness since childhood, which had increased over the past eight days (modified Medical Research Council grade III), a cough with yellowish expectoration for 10 days and intermittent, undocumented fever for eight days, which was relieved with medication. A detailed history revealed the use of tablet Bosentan 62.5 mg twice daily and tablet Dabigatran 75 mg twice daily for the past two years.
Physical examination revealed grade 3 clubbing [Table/Fig-1], with a pulse rate of 112 bpm, blood pressure of 110/70 mmHg, respiratory rate of 24 cycles/min and Saturation of peripheral Oxygen (SpO2) of 68% on Fraction of inspired Oxygen (FiO2) 21%. The respiratory examination revealed bilateral vesicular breath sounds with diminished intensity in the right mammary, infrascapular and infra-axillary areas, likely suggestive of pleural effusion. The cardiovascular examination suggested a holosystolic murmur at the left 3rd intercostal space. No abnormal findings were noted in other systems.
Image showing bilateral grade 3 clubbing.

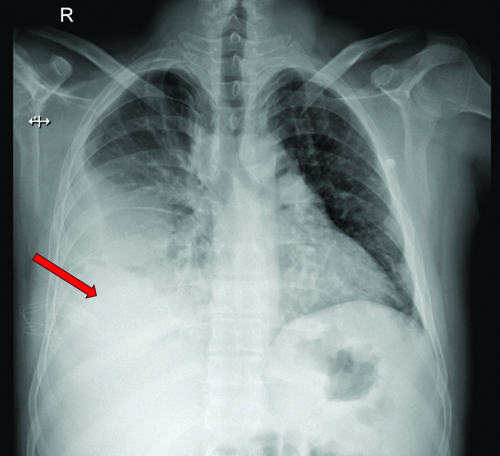
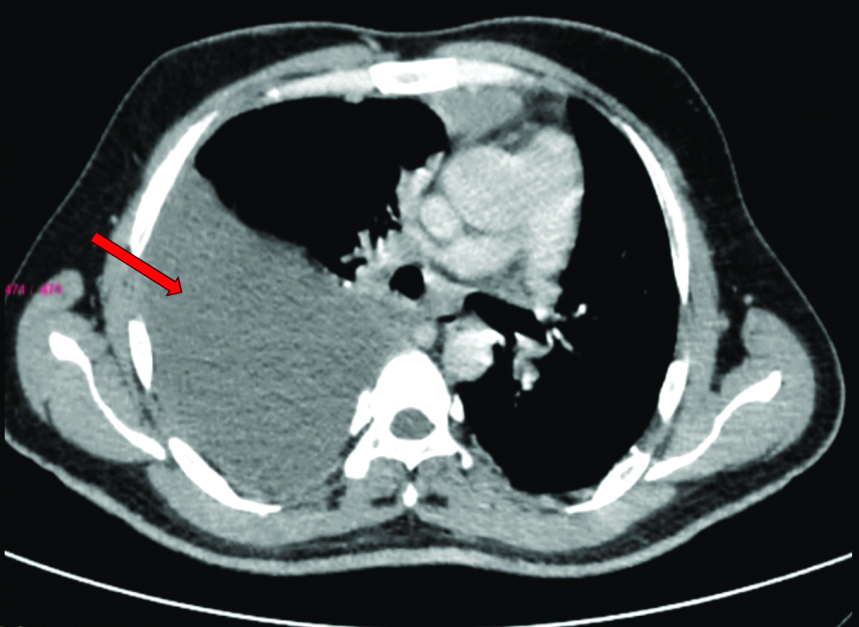
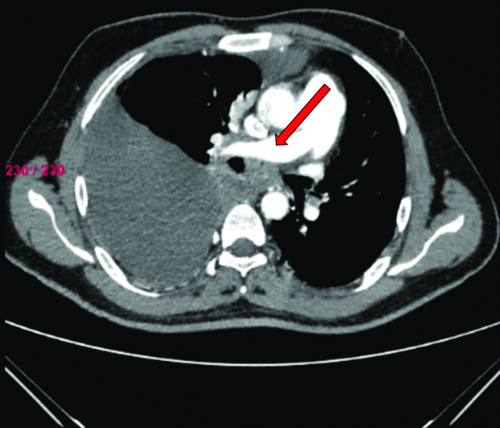
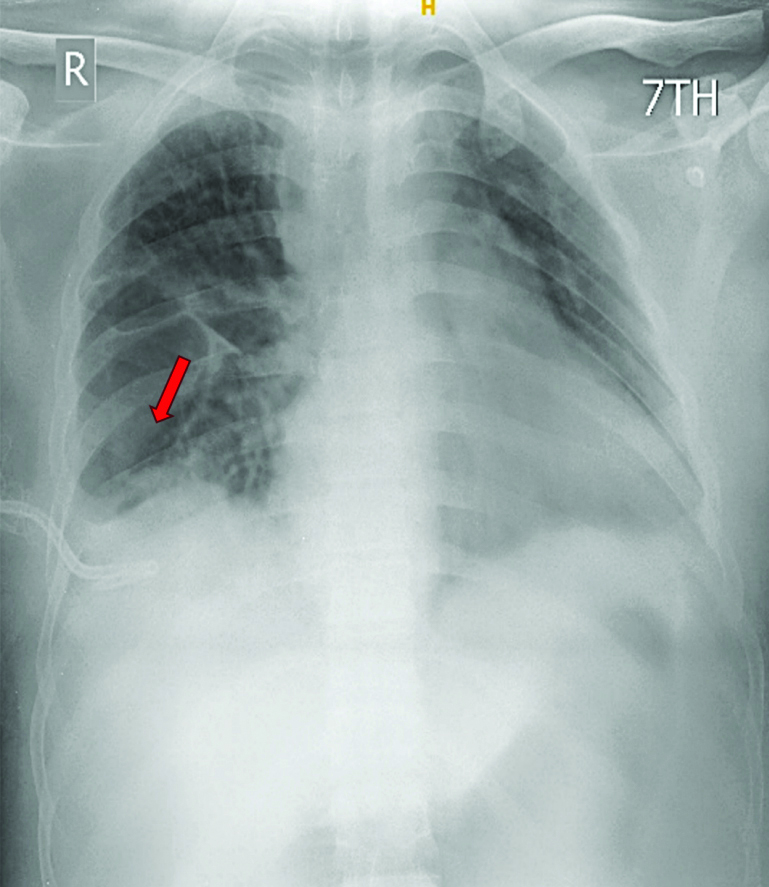
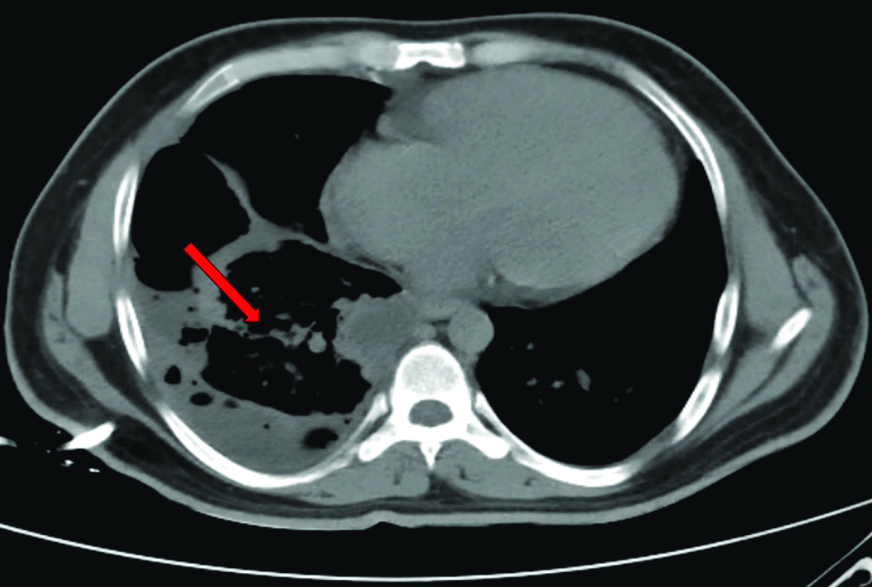
Radiological investigations included a chest X-ray showing right middle and lower zone homogeneous opacity obliterating the right cardiophrenic and costophrenic angles, suggestive of right pleural effusion [Table/Fig-2]. An ultrasound of the thorax indicated a gross right pleural effusion (>1000 cc) with internal septations. High-Resolution Computed Tomography (HRCT) and CT Pulmonary Angiogram (CTPA) confirmed the gross right pleural effusion without evidence of thromboembolism [Table/Fig-3]. It showed a large abnormal communication between the left distal ascending aorta and the right wall of the main pulmonary artery [Table/Fig-4].
Chest X-ray showing right middle and lower zone homogenous opacity (red arrow) with obliteration of the right cardiophrenic and costophrenic angles.
CTPA thorax suggestive of Gross right-sided pleural effusion (red arrow).
CT pulmonary angiography showing a large abnormal communication between the left distal ascending aorta and the right wall of the mail pulmonary artery.
A 2D echocardiogram revealed a Left Ventricular Ejection Fraction (LVEF) of 60%, a dilated Right Atrium (RA) and Right Ventricle (RV), severe Pulmonary Arterial Hypertension (PAH) with Right Ventricular Systolic Pressure (RVSP) of 80 mm Hg and a small Patent Foramen Ovale (PFO) with a right-to-left shunt.
Laboratory investigations showed a haemoglobin level of 13.9 g/dL, Packed Cell Volume (PCV) of 41.2%, Total Leucocyte Count (TLC) of 14,600, platelet count of 1.4 lacs, a normocytic and normochromic Peripheral Blood Smear (PBS), blood urea of 27 mg/dL, serum creatinine of 0.95 mg/dL, serum sodium (Na+) of 138 mEq/L, serum potassium (K+) of 3.8 mEq/L and an International Normalised Ratio (INR) of 1.20. Liver Function Tests (LFT) were Within Normal Limits (WNL). The C-reactive Protein (CRP) levels were borderline elevated (1 mg/dL).
Pleural fluid analysis revealed a reddish appearance, TLC of 1800 cells, Differential Leucocyte Count (DLC) of 15% neutrophils and 75% lymphocytes, Adenosine Deaminase (ADA) of 31.6 IU/L, serum Lactate Dehydrogenase (LDH) of 596 IU/L, Pleural fluid (P/f) LDH of 260 IU/L, serum protein of 7.7 g/dL, P/f protein of 14.5 g/dL, serum glucose of 112 mg/dL, P/f glucose of 48 mg/dL, P/f Red Blood Cell (RBC) of 150-200 and pleural fluid haematocrit of 51.2%. The pleural fluid to serum haematocrit ratio was above 0.5, highly suggestive of haemothorax.
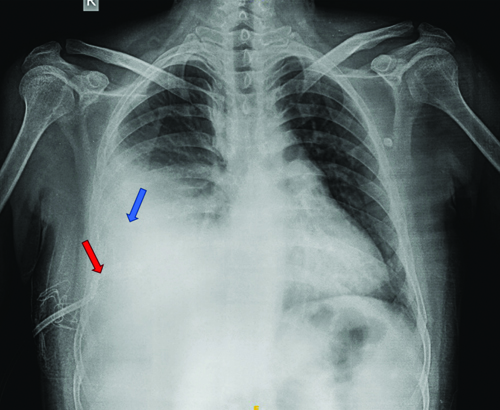
The patient was diagnosed with right loculated pleural effusion-haemothorax and congenital heart disease with Eisenmenger syndrome. Initial management included the insertion of a right-sided 14 F pigtail catheter, intravenous antibiotics, adequate analgesia and oxygen therapy. However, the initial drainage post-pigtail insertion was minimal (100 mL) [Table/Fig-5]. Due to the lack of subsequent drainage, even after reconfirming the tube position and patience, the patient was administered IPFT with 2.5 lac IU STK. The first cycle of IPFT resulted in 1150 mL of drainage, with a cumulative drainage of 2250 mL after three days [Table/Fig-6,7].
Chest X-ray showing right-sided pleural effusion (blue arrow) with pigtail in-situ (red arrow) prior to Intrapleural Fibrinolytic Therapy (IPFT).
Chest X-ray three days post Intrapleural Fibrinolytic Therapy (IPFT) showing resolution of effusion (red arrow).
CT thorax showing resolution of effusion (red arrow) post Intrapleural Fibrinolytic Therapy (IPFT).
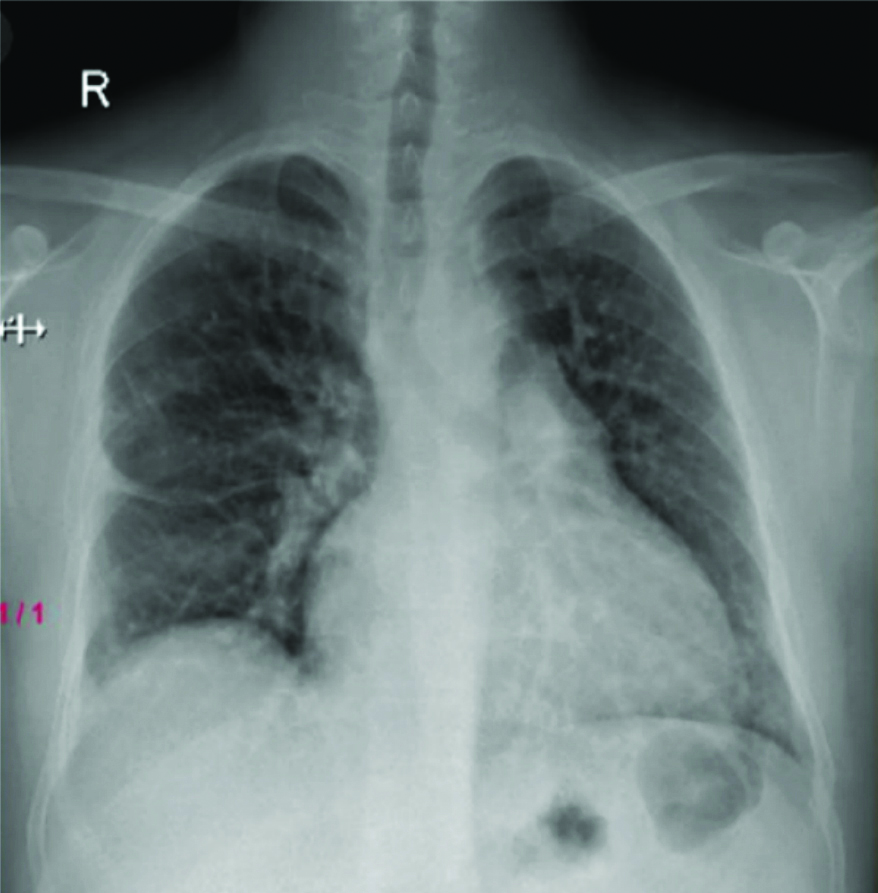
After confirming resolution on serial chest radiography, the intercostal drainage was removed and the patient was followed-up in the outpatient unit. No recurrence of pleural effusion was noted in subsequent chest radiographies [Table/Fig-8].
Follow-up chest X-ray of the patient (after 2 months).
Discussion
The present case report describes a right-sided loculated haemothorax associated with Eisenmenger syndrome and congenital heart disease. Prolonged usage of anticoagulants, including dabigatran, is believed to be the likely cause of the haemothorax.
Haemothorax, defined as the presence of blood in the pleural cavity with a haematocrit of greater than 50%, can result from both traumatic and non traumatic causes [1]. Initial treatment typically involves tube thoracostomy; however, if drainage is insufficient, further interventions are indicated [2]. Several options include saline flushes, the insertion of one or more catheters into the loculi under image guidance, standard thoracotomy, Video-assisted Thoracoscopic Surgery (VATS), empyema drainage and decortication [3]. IPFT is a less invasive and cost-effective alternative for treating clotted haemothorax compared to surgical procedures [4].
Adults receiving fibrinolytic therapy are usually administered 100,000 IU of Urokinase (UK) or 250,000 IU of STK every eight hours [4]. The medication is first reconstituted in 50 cc of normal saline before being introduced via the intercostal drain and flushed with 20 cc of normal saline [4]. The patient is instructed to alternate positions often and the chest tube is clamped for two hours following the administration of each dose [5]. Three doses of UK or STK constitute the therapy cycle [5]. The amount of pleural fluid drained and the radiological improvement indicate whether the fibrinolysis cycle was successful [5]. Responders who show little to moderate radiological improvement within 48 hours and cumulative drainage of more than 100 mL are considered for another cycle of therapy [5]. Individuals who fall short of these standards are labelled as non responders [5].
In the present case, the patient had a significant haemothorax on the right-side that did not drain after the insertion of a pigtail catheter. The clearance of the loculated haemothorax was aided by the IPFT with STK injection, as evidenced by the significant drainage volumes and notable radiological improvement. In line with earlier studies, a 91.7% success rate in dissolving fibrinous septations was achieved by Inci I et al., in their investigation of 24 patients undergoing treatment for haemothorax using fibrinolytic medications such as STK and UK [2]. A 5-year observational study by Barthwal MS et al., found that patients with haemothorax had a 91.6% success rate [4].
Kimbrell BJ et al., conducted a prospective investigation on patients who had suffered a traumatic haemothorax, showing a 92% success rate [5]. Other recent studies by Kumar S et al., and Caylor M et al., in accordance with earlier studies like Jerjes-Scanchez C et al., found that patients with haemothorax had similar outcomes, with a significant resolution of 70% or more [Table/Fig-9] [4-8].
Comparative analysis of various studies, where Intrapleural Fibrinolytic Therapy (IPFT) was used in haemothorax cases [2,4-8,12].
| Authors | Type of study | Sample size | Type of effusion | Key results |
|---|
| Jerjes-Sánchez C et al., [8]1993-1995 | Prospective study | 48 patients | Loculated haemothorax | Success rate- 92% |
| Inci I et al., [2]1995-1997 | Prospective study | 24 patients | Traumatic clotted haemothorax | Success rate- 91.7% |
| Skeete DA et al., [12]1999-2003 | Retrospective study | 41 patients | Complicated pleural effusions | Success rate- 78% |
| Kimbrell BJ et al., [5]2003-2005 | Prospective study | 25 patients | Traumatic haemothorax | Success rate- 92%2 required surgical intervention |
| Barthwal MS et al., [4]2008-2013 | 5 years observational study | 12 patients | Haemothorax | Success rate- 91.6% |
| Caylor M et al.,2010-2013 [7] | Retrospective observational analysis | 24 patients | Traumatic haemothorax | Success rate- 83.4% |
| Kumar S et al., [6]2011-2013 | Randomised Control Trial (RCT) | 146 patients (17 haemothorax) | Retained haemothorax | Success rate- 70.6% |
The STK and other fibrinolytics work by dissolving various proteins, including fibrin, blood clots and pleural loculations [9]. The plasminogen-STK complex is enzymatically activated by STK to produce plasmin, which initiates the fibrinolytic response [9]. Furthermore, as demonstrated in the present case, plasmin has the ability to lyse the septa of multiloculated pleural space collections, permitting unhindered pleural fluid flow and final resolution [9].
Since IPFT is a widely accessible, safe and efficient substitute for VATS, it should be incorporated into the management strategy for clotted haemorrhage within the seven to ten-day window [10]. An investigation by Bouros D et al., shows that optimal pleural drainage occurs when fibrinolytic therapy is started early, before to the development of pleural adhesions [11].
Conclusion(s)
The IPFT with STK is an effective and less invasive treatment for clotted haemothorax in patients with complex medical backgrounds. Early initiation of fibrinolytic therapy enhances pleural drainage and prevents the complications associated with invasive surgical procedures. The authors noted significant radiological and clinical improvement in the present patient with congenital heart disease and Eisenmenger syndrome following IPFT, highlighting it as a valuable treatment option in similar clinical scenarios, particularly for patients at high-risk for surgery.
[1]. Zeiler J, Idell S, Norwood S, Cook A, Hemothorax: A review of the literatureClin Pulm Med [Internet] 2020 27(1):01-12.Available from: https://journals.lww.com/clinpulm/fulltext/2020/01000/hemothorax__a_review_of_the_literature.1.aspx10.1097/CPM.000000000000034333437141 [Google Scholar] [CrossRef] [PubMed]
[2]. Inci I, Özçelik C, Ülkü R, Tuna A, Eren N, Intrapleural fibrinolytic treatment of traumatic clotted hemothoraxChest [Internet] 1998 114(1):160-65.Available from: https://journal.chestnet.org/article/S0012369215476330/fulltext10.1378/chest.114.1.1609674464 [Google Scholar] [CrossRef] [PubMed]
[3]. Boersma WG, Stigt JA, Smit HJM, Treatment of haemothoraxRespir Med [Internet] 2010 104(11):1583-87.Available from: https://www.resmedjournal.com/article/S0954611110003513/fulltext10.1016/j.rmed.2010.08.00620817498 [Google Scholar] [CrossRef] [PubMed]
[4]. Barthwal MS, Marwah V, Chopra M, Garg Y, Tyagi R, Kishore K, A five-year study of intrapleural fibrinolytic therapy in loculated pleural collectionsIndian J Chest Dis Allied Sci 2016 58:1710.5005/ijcdas-58-1-17 [Google Scholar] [CrossRef]
[5]. Kimbrell BJ, Yamzon J, Petrone P, Asensio JA, Velmahos GC, Intrapleural thrombolysis for the management of undrained traumatic hemothorax: A prospective observational studyJ Trauma 2007 62(5):1175-78.Available from: https://journals.lww.com/jtrauma/fulltext/2007/05000/intrapleural_thrombolysis_for_the_management_of.18.aspx10.1097/TA.0b013e318050065417495721 [Google Scholar] [CrossRef] [PubMed]
[6]. Kumar S, Rathi V, Rattan A, Chaudhary S, Agarwal N, VATS versus intrapleural streptokinase: A prospective, randomized, controlled clinical trial for optimum treatment of post-traumatic Residual HemothoraxInjury 2015 46(9):1749-52.10.1016/j.injury.2015.02.02825813733 [Google Scholar] [CrossRef] [PubMed]
[7]. Caylor M, Hamblin S, Guillamondegui O, Johnson D, Dennis B, 1056: Efficacy of intrapleural TPA for retained hemothorax in trauma patientsCrit Care Med [Internet] 2014 42:A1614Available from: https://journals.lww.com/ccmjournal/fulltext/2014/12001/1056__efficacy_of_intrapleural_tpa_for_retained.1023.aspx10.1097/01.ccm.0000458553.78740.64 [Google Scholar] [CrossRef]
[8]. Jerjes-Sánchez C, Ramirez-Rivera A, Elizalde JJ, Delgado R, Cicero R, Ibarra-Perez C, Intrapleural fibrinolysis with streptokinase as an adjunctive treatment in hemothorax and empyema: A multicenter trialChest 1996 109(6):1514-19.10.1378/chest.109.6.15148769503 [Google Scholar] [CrossRef] [PubMed]
[9]. Foo CT, Herre J, Intrapleural fibrinolysis in acute non-traumatic retained haemothoraxRespirol Case Rep [Internet] 2021 9(6):e00760Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/rcr2.76010.1002/rcr2.76033976889 [Google Scholar] [CrossRef] [PubMed]
[10]. Agarwal R, Aggarwal AN, Gupta D, Intrapleural fibrinolysis in clotted haemothoraxSingapore Med J 2006 47(11):984-86.Available from: https://pubmed.ncbi.nlm.nih.gov/17075670/ [Google Scholar]
[11]. Bouros D, Schiza S, Tzanakis N, Chalkiadakis G, Drositis J, Siafakas N, Intrapleural urokinase versus normal saline in the treatment of complicated parapneumonic effusions and empyema. A randomized, double-blind studyAm J Respir Crit Care Med 1999 159(1):37-42.Available from: www.atsjournals.org10.1164/ajrccm.159.1.98030949872815 [Google Scholar] [CrossRef] [PubMed]
[12]. Skeete DA, Rutherford EJ, Schlidt SA, Abrams JE, Parker LA, Rich PB, Intrapleural tissue plasminogen activator for complicated pleural effusionsJ Trauma 2004 57(6):1178-83.Available from: https://journals.lww.com/jtrauma/fulltext/2004/12000/intrapleural_tissue_plasminogen_activator_for.6.aspx10.1097/01.TA.0000141879.67441.5215625447 [Google Scholar] [CrossRef] [PubMed]