EZ-Blocker™ is a specially designed semi-rigid Y-shaped Bronchial Blocker (BB) containing two inflatable cuffs. The difficulties and challenges encountered while inserting the Rusch EZ-Blocker™ (Teleflex Life Sciences Ltd., Athlone, Ireland) for isolating the left lung in Minimally Invasive Coronary Artery Bypass Graft (MICS CABG) surgery are numerous and varied. The present case series describes 28 different patients (out of 102 patients with attempted EZ-Blocker™) who faced various difficulties and technical problems while introducing the EZ-Blocker™ and how troubleshooting was performed in those cases with different manoeuvres. The difficulties in inserting the EZ-Blocker™ were due to a variety of reasons such as inadequate space between the carina and bronchus, a prominent right main bronchus at an acute angle compared to the obtuse angle of the left main bronchus, a compressed left main bronchus, deviation of the airway and a deep posterior bronchus. The manoeuvres used to overcome these challenges included controlled pulling of the endotracheal tube upwards, rotation of the head to the right-side with or without direct tracheal manual compression to the right-side, manual widening of the distal Y end of the EZ-Blocker™ and extension of the head in selected cases. Out of 102 attempted cases of EZ-Blocker™, difficulty (insertion time >90 seconds) was noted in 28 cases, which were managed with the different clinical manoeuvres mentioned above. However, in four other cases, the EZ-Blocker™ could not be introduced and the attempts failed. Although the EZ-Blocker™ is a safe and easy alternative to the Double Lumen Tube (DLT), it has not been widely used in India to date. The proposed manoeuvres will surely help clinicians use it more efficiently in cases where they encounter difficulty during insertion.
Coronary artery bypass graft, Clinical manoeuvres, Difficult insertion, Lung isolation
Introduction
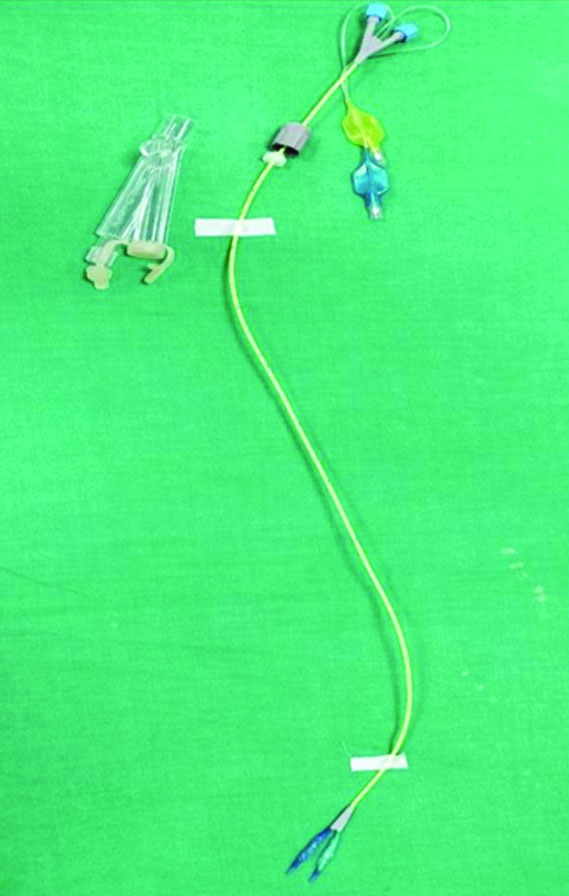
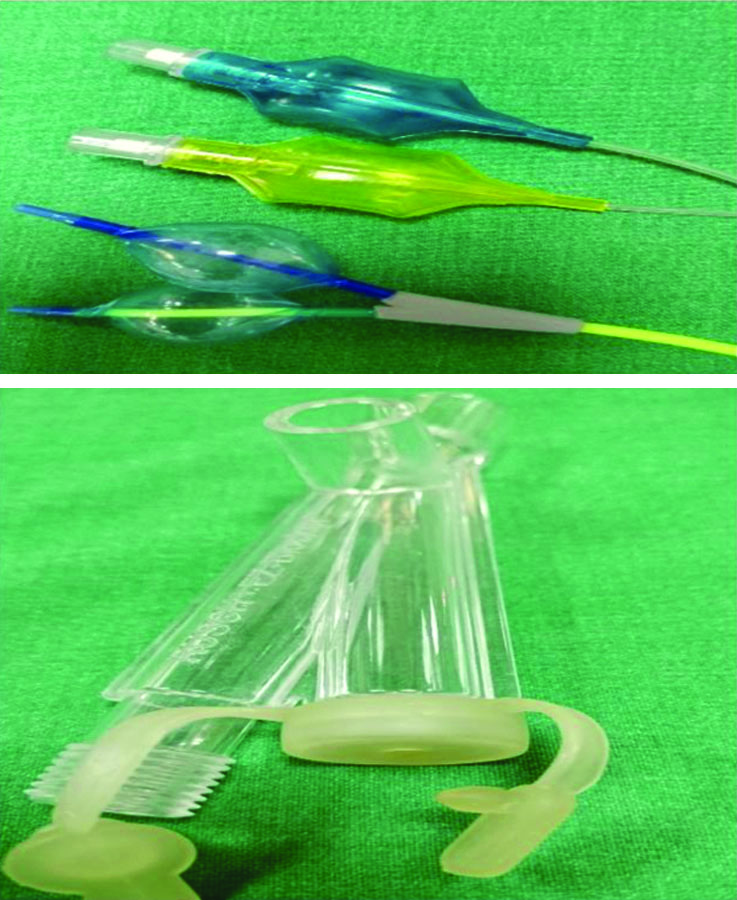
In MICS CABG surgery, it’s mandatory to isolate the left lung for a left anterior thoracotomy. This can be achieved by using either a left DLT or a BB. Both DLT and BB have different pros and cons [1,2]. Sometimes, correct placement of a DLT may be technically difficult and bear additional risk of trauma to the trachea and the bronchi [3,4]. EZ-Blocker™ are relatively new in India and only a few centres use them. Apart from this, other blockers available are single-cuff endobronchial blockers (for example, COOPDECH™, Diaken Medical Company Ltd., Japan and the Arndt™ blocker, Cook Medical Inc., Bloomington, IN, USA, etc.). All BBs are placed under direct vision using a Fibreoptic Bronchoscope (FOB). The EZ-Blocker is a semi-rigid endobronchial blocker made of polyurethane. It is 7-French in outer diameter and 75 cm long. It has four lumens and is Y-shaped [Table/Fig-1]. This blocker has two different coloured (blue and yellow) 4 cm long symmetrical distal extensions [Table/Fig-2,3]. Both have an inflatable cuff and a small central lumen and a pressure line connected to the external blue and yellow-coloured balloons. Two proximal colour-coded balloons of the blocker serve to inflate or deflate the cuffs. Two additional lumens at the distal end are used for suction or oxygen insufflation into the non dependent lung. The EZ-Blocker™ is supplied with a multiport adaptor. This adaptor connects to the ventilator end of a single lumen tube (minimum diameter 7 mm) and also allows the introduction of a FOB or a suction catheter. The right deployment of the Y-shaped distal part usually needs a minimum of 4 cm distance from the distal end of the single lumen tube and the carina. The Y-shape helps the device to anchor onto the carina. Therefore, the EZ-Blocker™ poses less chance of secondary malposition compared to other blockers [5,6]. Usually, the EZ-Blocker™ is considered a user-friendly blocker for easy one-lung ventilation [7-9]. Although the average time taken for a BB insertion was reported to be as high as 4-6 minutes [8], Vegh T et al., in a study concluded that the mean time for the placement of the EZ-Blocker™ was 76±15 seconds [10]. Based on this study by Vegh T et al., in this reported case series, difficult insertion has been taken as >90 seconds as the mean time of placement was 76±15 seconds in their study [10]. The EZ-Blocker™ is a relatively new blocker available in India. The manoeuvres described below come from our wide clinical practice as it has been used in a large number of cases. It has not been described in the literature before, but these are really effective ways to manage difficult cases.
Full assembly of EZ-Blocker™.
Balloons and cuffs and the multiport adaptor of EZ-Blocker™.
Left-sided yellow cuff inflated.
Case Series
In a one and a half-year time duration, 102 EZ-Blocker™ placements were attempted for MICS CABG surgery. An 8-8.5 size endotracheal tube for male patients and a 7-7.5 size endotracheal tube for females were used. After the insertion of a single-lumen tube, a check with fibreoptic bronchoscopy was done to approximately get an idea about the distance between the tube end and the carina. This distance should ideally be more than 4 cm for easy opening of EZ distal cuffs. The length of fixation of the single tube was changed if necessary by bronchoscopy. As preparation for EZ-Blocker™ insertion, two pilot balloon cuffs were inflated and checked for air leaks before insertion. A silicone gel spray was applied to the distal ends for smooth insertion. After the induction of general anaesthesia and endotracheal intubation with a single-lumen tube, the EZ-Blocker™ was introduced through the multiport adaptor until it reached and straddled at the carina. For adequate cuff seal, the authors used 8-10 mL of air under FOB (3.8 mm, Pentax EB-1170K, Breda, The Netherlands) guidance. The time from insertion of the EZ-Blocker™ through the multiport adaptor to the final check of its proper position by fibreoptic bronchoscopy was recorded. In most cases, the EZ-Blocker™ reached the correct position smoothly in less than 90 seconds. The term ‘difficult’ was used when the operator failed to place the EZ-Blocker™ correctly in less than 90 seconds. This is based on the study conducted by Veg T et al., who showed that the mean time to insert the EZ-Blocker™ was 76±15 seconds. Different clinical manoeuvres were applied when it was found to be difficult (unable to place in less than 90 seconds). All the blockades were performed by the same anaesthetist with more than 10 years of experience in cardiac anaesthesia.
Out of the 102 attempted cases of EZ-Blocker™, 28 cases were found to be difficult (insertion time more than 90 seconds) and challenging and different manoeuvres were applied to facilitate quick and successful positioning of the EZ-Blocker™ to isolate the left lung.
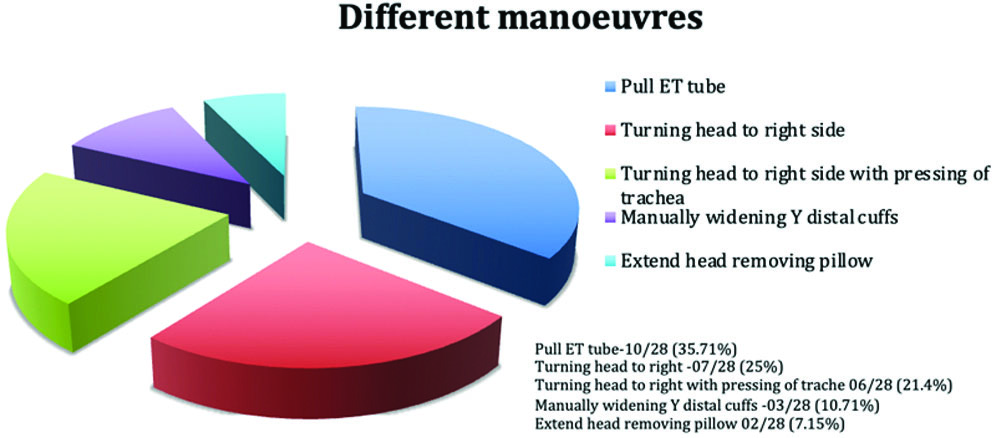
Out of 28 difficult insertions, in 10 patients, there was inadequate length and space between the distal end of the endotracheal tube and the carina (although being checked by fibreoptic bronchoscopy beforehand). So, the cuff of the single-lumen tube was deflated and it was cautiously pulled further up [Table/Fig-4] to create more length while ensuring that the tube is not coming out too far and out of the vocal cords. This extra length made the manipulation of the EZ-Blocker™ easy and facilitated successful placement, as atleast 4 cm of length should be available from the distal end of the endotracheal tube to the carina [11].
Pulling the single lumen tube up.

In seven cases, the right main bronchus originated at a more acute angle, while the left main bronchus originated at a more obtuse angle. This led to the passage of the EZ-Blocker™ with both cuffs to the right-side repeatedly. In these cases, the head was turned completely to the right-side, which made the left bronchus more prominent and centered, facilitating successful EZ insertion with the cuff on the left-side.
In six patients, the above situation became more extreme with a more compressed left main stem bronchus, causing the two balloons of the EZ-Blocker™ to enter the right main bronchus. Along with turning the head to the right-side, manual compression of the trachea towards the right-side was performed to make the left main bronchus more prominent and centered, enabling correct placement [Table/Fig-5].
Head turning to right with manual tracheal compression to right.

In three patients, the trachea was relatively small and the two distal cuffs of the EZ-Blocker™ were adhered to each other due to mucus and thick secretions. The EZ-Blocker™ was removed from the multiport adaptor, cleaned and the Y distal end was manually spread before reinsertion. This maneuver resolved the above problem and enabled successful EZ placement.
In a couple of patients, the airway carina was quite posterior, causing the EZ-Blocker™ to slide towards the anterior part and hit above the carina instead of entering the lumens. Removing the pillow and extending the neck improved the situation by slightly anteriorly positioning the airway, allowing the EZ distal balloons to enter each main bronchus.
In four cases, despite all manoeuvres and spending more than 10 minutes with repeated attempts, EZ-Blocker™ insertion failed. In three of those patients, single-lumen COOPDECH™ blockers were used, while in another patient, blocker placement was abandoned due to significant hypoxemia followed by bradycardia and asystole. Immediate open sternotomy and cardiopulmonary bypass were performed, eventually saving the patient.
The incidence of postoperative hoarseness and sore throat among a total of 102 patients was approximately 5 (4.9%) patients and 14 (13.72%) patients, respectively. A summary of all the patients and the manoeuvres has been presented in [Table/Fig-6,7].
Characteristics of patients, types of difficulty faced, used manoeuvres and outcome of difficult EZ-Blocker™.
| Number of difficult EZ insertion (left) | Patient characteristics | Procedure | Challenges and difficulties | Manoevre and outcome |
|---|
| 10 patients | 7 male and 3 female patients | MICS CABG | Inadequate space between carina and main stem bronchus. | Controlled traction of the ETT.All successfulNo episode of desaturation. |
| 07 patients | 05 male and 02 female patients | MICS CABG | Prominent right main bronchus, more acute angle and obtuse origin left main bronchus. | Turning head to right-side.All successful01 case of desaturation upto SpO2 90%. |
| 06 patients | All male patients | MICS CABG | Prominent right main bronchus, more acute angle and compressed left main bronchus. More deviated and prominent right main bronchus. | Turning head to right-side+press the trachea towards right-side manually.All successful 02 patients with desaturation upto mid 90%. |
| 03 patients | 02 female and 01 male patient | MICS CABG | Small carina and EZ-Blocker™ two balloons are stuck/adhered with secretions. | Removing EZ-Blocker™ and manually widening the cuffs to create wide space between balloons.All successful. |
| 02 patients | 02 male patients | MICS CABG | Airway deep, posterior. | Remove pillow to extend head and make airway anterior, all successful 01 desaturation upto 92%. |
Different manoeuvres to troubleshoot difficult EZ-Blocker™ insertion.
Discussion
The present case series has described the different types of technical difficulties and challenges during the insertion of the EZ-Blocker™, as well as the different manoeuvres to overcome them. To date, not too many problems and factors for difficult EZ-Blocker™ insertion have been reported in the literature. Rispoli M et al., proposed the inflated positioning technique when both cuffs go into the right main bronchus [11]. Goto M et al., reported almost the same technique with the inflation of both balloons [12]. Entrapment of the EZ-blocker in the Murphy eye has also been reported [13].
The present case series reports 28 cases (out of a total of 102 attempted EZ-Blocker™ insertions) where the EZ-Blocker™ insertion was “difficult.” In the present case series, 05 different manoeuvres (used alone or in combination) to troubleshoot the obstacles for successful placement have been described. Ultimately, by applying these manoeuvres, there was success in most of the difficult cases. The practiced manoeuvres in the present case series came from the vast experience of using EZ-Blocker™ in large numbers by the authors. By using them, it can be confirmed that the EZ-Blocker™ are a safe, easy and reliable blocker and the quality of lung isolation is comparable to DLT, as reported by Mourisse J et al., and Végh T et al., in studies [9,10]. Compared to the systematic review conducted by Palacznski P et al., the incidence of hoarseness and sore throat is less in this study [14]. The recent study by Palacznski P et al., reported the incidence of hoarseness and sore throat as 13% and 23.3%, respectively. The experience and knowledge of the operator about the anatomy and the device are key factors to potentially deal with difficult EZ-Blocker™ successfully. This is a new study on EZ-Blocker™ and no similar study has been published in the literature to date. The present case series will raise awareness among anaesthesiologists and clinicians to know the range of difficulties and their probable solutions associated with EZ-Blocker™. It can be concluded that the EZ-Blocker™ is a safe, easy and reliable device for lung isolation in the hands of clinicians with good clinical expertise.
Conclusion(s)
The present case series highlighted the wide range of difficulties related to real-time insertion of the EZ-Blocker™ and how we managed them with different simple but efficient manoeuvres. The EZ-Blocker™ is a safe, user-friendly and reliable endobronchial blocker with a great success rate in the hands of experienced operators. The authors are not promoting any device brand and this device is mentioned only for research purposes.
Author Declaration:
Financial or Other Competing Interests: None
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 08, 2024
Manual Googling: Sep 10, 2024
iThenticate Software: Oct 10, 2024 (07%)
[1]. Clayton-Smith A, Bennett K, Alston RP, Adams G, Brown G, Hawthorne T, A comparison of the efficacy and adverse effects of double-lumen endobronchial tubes and bronchial blockers in thoracic surgery: A systematic review and meta-analysis of randomized controlled trialsJ Cardiothorac Vasc Anesth 2015 29(4):955-66.10.1053/j.jvca.2014.11.01725753765 [Google Scholar] [CrossRef] [PubMed]
[2]. Neustein SM, The use of bronchial blockers for providing one-lung ventilationJournal of Cardiothoracic and Vascular Anesthesia 2009 23(6):860-68.10.1053/j.jvca.2009.05.01419632864 [Google Scholar] [CrossRef] [PubMed]
[3]. Knoll H, Ziegeler S, Schreiber JU, Buchinger H, Bialas P, Semyonov K, Airway injuries after one-lung ventilation. a comparison between double-lumen tube and endobronchial blocker: A randomized, prospective, controlled trialAnesthesiology 2006 105(3):471-77.10.1097/00000542-200609000-0000916931978 [Google Scholar] [CrossRef] [PubMed]
[4]. Fitzmaurice BG, Brodsky JB, Airway rupture from double-lumen tubesJ Cardiothorac Vasc Anesth 1999 13(3):322-29.10.1016/S1053-0770(99)90273-210392687 [Google Scholar] [CrossRef] [PubMed]
[5]. Narayanaswamy M, McRae K, Slinger P, Dugas G, Kanellakos GW, Roscoe A, Choosing a lung isolation device for thoracic surgery: A randomized trial of three bronchial blockers versus double-lumen tubesAnesth Analg 2009 108(4):1097-101.10.1213/ane.0b013e318199933919299767 [Google Scholar] [CrossRef] [PubMed]
[6]. Kus A, Hosten T, Gurkan Y, Gul Akgul A, Solak M, Toker A, A comparison of the EZ-Blocker with a Cohen Flex-Tip blocker for one-lung ventilationJ Cardiothorac Vasc Anesth 2014 28(4):896-99.10.1053/j.jvca.2013.02.00623958073 [Google Scholar] [CrossRef] [PubMed]
[7]. Van de Pas JM, van der Woude MC, Belgers HJ, Hulsewe KW, de Loos ER, Bronchus perforation by EZ-blocker TM endobronchial blocker during esophagial resection after neoadjuvant chemoradiation- a case reportKorean J Anesthesiol 2019 72(2):184-87.10.4097/kja.d.18.0023730553237 [Google Scholar] [CrossRef] [PubMed]
[8]. Ruetzler K, Grubhofer G, Schmid W, Papp D, Nabecker S, Hutschala D, Randomized clinical trial comparing double-lumen tube with EZ-blocker for single-lung ventilationBr J of Anaesth 2011 106(6):896-902.10.1093/bja/aer08621493621 [Google Scholar] [CrossRef] [PubMed]
[9]. Mourisse J, Liesveld J, Verhagen A, van Rooji G, van der Heide S, Schuurbiers-Siebers O, Efficiency, efficacy and safety of EZ-blocker compared with left-sided double-lumen tube for one-lung ventilationAnesthesiology 2013 118(3):550-61.10.1097/ALN.0b013e3182834f2d23299364 [Google Scholar] [CrossRef] [PubMed]
[10]. Vegh T, Juhasz M, Enyedi A, Takacs I, Kollar J, Fulesdi B, Clinical experience with a new endobronchial blocker: The EZ-blockerJ Anesthesiol 2012 26(3):375-80.10.1007/s00540-011-1315-022278374 [Google Scholar] [CrossRef] [PubMed]
[11]. Rispoli M, Nespoli MR, Ferrara M, Rosboch GL, Templeton LB, Templeton TW, A practical guide for using the EZ-blocker endobronchial blocker: Tips and tricks after 10 years of experienceJ Cardiothorac Vasc Anesth 2023 37(10):1884-93.10.1053/j.jvca.2023.06.01537481398 [Google Scholar] [CrossRef] [PubMed]
[12]. Goto M, Aoyama K, Nishimura M, Takeda T, Simultaneous inflation of both cuffs of an EZ-blocker device facilitates selective endobronchial isolationJ Cardiothorac Vasc Anesth 2022 36(8 Pt B):3429-30.10.1053/j.jvca.2022.03.03935537975 [Google Scholar] [CrossRef] [PubMed]
[13]. Tang J, Merritt RE, Essandoh M, Entrapment of an EZ-Blocker in the murphy eye of an endotracheal tubeJ Cardiothorac Vasc Anesth 2019 33(10):2873-74.10.1053/j.jvca.2019.04.00631078375 [Google Scholar] [CrossRef] [PubMed]
[14]. Palaczynski P, Misiolek H, Szarpak L, Smereka J, Pruc M, Rydel M, Systematic review and meta-analysis of efficiency and safety of double -lumen tube and bronchial blocker for one-lung ventilationJ Clin Med 2023 12(5):187710.3390/jcm1205187736902663 [Google Scholar] [CrossRef] [PubMed]