Plantar fasciitis, or Vatakantaka, is a common cause of heel pain characterised by inflammation and swelling in the plantar fascia, leading to discomfort. Standard treatments often yield poor results, which has motivated research into new therapies. The present case series includes 10 patients (five males and five females) with plantar fasciitis who were treated with a topical application of Nirgundi Lepa twice a day for four weeks. Pain levels were assessed using the Visual Analogue Scale (VAS), and foot function was evaluated with the Foot Function Index (FFI) at baseline, two weeks after treatment, and at the conclusion of the study. Nirgundi Lepa was applied to the feet of both limbs, resulting in a reduction in pain and an improvement in foot function. VAS scores decreased by an average of 65%, and the FFI-related symptom improvement rate increased to 55%. The therapeutic effects observed during the follow-up period were sustained, with minimal recurrence of symptoms. The present case series illustrates the utility of Nirgundi Lepa in patients with plantar fasciitis, positioning it as an effective non surgical modality for managing heel pain. Further research is needed to confirm these results and assess their value in clinical practice.
Introduction
Plantar fasciitis, known as Vatakantaka in Ayurvedic terminology, is a common cause of heel pain that significantly impacts daily activities and quality of life [1]. It involves degenerative irritation and microtears of the plantar fascia at the medial calcaneal tuberosity, often due to overuse or biomechanical factors such as flat feet, high arches, limited ankle dorsiflexion, prolonged standing and excessive foot pronation or supination [2]. Although the condition is marked by inflammation, it predominantly features degenerative changes, including granulation tissue and collagen disarray.
Conventional treatments, including Non Steroidal Anti-Inflammatory Drugs (NSAIDS), physical therapy and orthotics, provide varying degrees of relief but may have limitations and side effects [3]. Diagnostic imaging, such as ultrasound and Magnetic Resonance Imaging (MRI), often shows thickening, tears and calcifications in the fascia, indicating a non inflammatory, degenerative process. Ayurveda offers alternative remedies, such as Nirgundi (Vitex negundo) Lepa, known for its anti-inflammatory and analgesic properties [4,5].
Plantar fasciitis is prevalent among runners, older adults and individuals with a high body mass index, significantly affecting their quality of life and daily functions [6]. It accounts for 10% of injuries in runners and 11-15% of foot symptoms in adults [7].
Case Series
Total of 10 patients presented with complaints of severe heel pain, especially in the morning, with an average duration of 4.5 months. This pain was aggravated by prolonged standing [Table/Fig-1]. It caused difficulty in walking and performing daily tasks. None of the patients had significant medical histories or family histories of similar conditions. They led active lifestyles, regularly walking and standing due to occupational requirements (farmer, housewife, businessperson, teacher). All patients had tried over-the-counter pain medications like NSAIDs, with limited relief, and used orthotic insoles, which provided temporary relief from the symptoms of Vatakantaka (plantar fasciitis).
Summary of the findings of the cases.
| Case no. | Age/sex | Chief complaint/Symptoms | Duration of chief complaint | Examinationfindings |
|---|
| 1 | 45/M | Heel pain, worse in the morning | 3 months | Tenderness at the plantar fascia |
| 2 | 52/F | Sharp pain in the heel | 6 months | Swelling and redness at heel |
| 3 | 48/M | Pain after prolonged standing at heal | 4 months | Tight Achilles tendon |
| 4 | 55/F | Stiffness and pain in the foot | 5 months | Pain on dorsiflexion |
| 5 | 40/M | Burning sensation and pain in the heel | 2 months | Pain with palpation of heel |
| 6 | 59/F | Heel pain after exercise | 7 months | Limited ankle range of motion |
| 7 | 47/M | Pain at heal radiating to the arch | 4 months | Thickened and tenderness at plantar fascia |
| 8 | 53/F | Heel pain, mainly in morning with first step | 3 months | Flatfoot deformity, Tenderness at the plantar fascia |
| 9 | 42/M | Sharp heel pain in the morning | 3 months | Tenderness on heel |
| 10 | 58/F | Chronic heel pain | 8 months | Swelling, pain, and redness at heel |
Physical examinations revealed tenderness at the medial calcaneal tuberosity in all patients, a positive Windlass test [8], and limited ankle dorsiflexion due to pain. The diagnostic assessment included a physical examination, noting tenderness and a positive Windlass test, while imaging was not performed due to the clear clinical presentation.
The therapeutic intervention involved the topical application of Nirgundi Lepa. Fresh Nirgundi leaves were collected from the study Institute’s Herbal Garden. The leaves were washed with water, then blended with one-fourth of the water to create a thick paste-like consistency [Table/Fig-2]. Approximately 50 milliliters of water was added to 200 grams of Nirgundi leaves. This standard preparation leverages the anti-inflammatory and analgesic properties of Vitex negundo.
Preparation of Nirgundi Lepa. a) Collection of fresh leaves; b) Thorough wash in clean water; c) Paste made by blending one fourth amount of water.
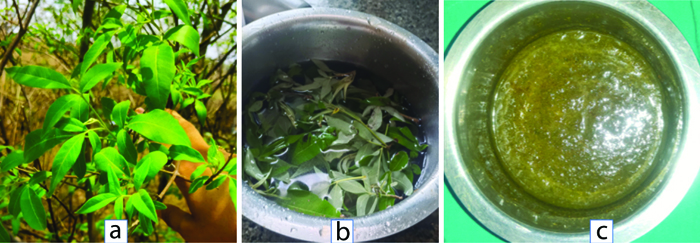
The patient was asked to first clean their legs with clean water. In a comfortable sitting position, Nirgundi Lepa was applied to the affected area to a thickness of approximately 0.5-1 mm, as shown in [Table/Fig-3]. This dosage was intended to ensure that the entire inflamed region of the plantar fascia was adequately covered, maximising the contact between the Lepa and the skin to facilitate absorption and therapeutic action. The Nirgundi Lepa was kept on until it dried, after which the patient was asked to wash their legs with lukewarm water. The same treatment was continued twice daily for four weeks. Applying the Lepa in the morning and evening ensured that the active compounds remained in contact with the affected area throughout the day and night, promoting continuous anti-inflammatory action and pain relief.
Application of Nirgundi Lepa.

Observations were recorded using the VAS pain score [Table/Fig-4] and the FFI [Table/Fig-5] of patients with Vatakantaka (plantar fasciitis) during the interventional period on day 0 (before intervention), day 14, day 28 and follow-up was conducted after 28 days on the 8th week (Day 56).
Observation of the VAS scale of the patients on various time scales.
| Case no. | VAS score |
|---|
| Baseline/at time of enrollment | Day 14 | Day 28 | Day 56 |
|---|
| 1 | 9 | 5 | 3 | 4 |
| 2 | 8 | 6 | 3 | 3 |
| 3 | 8 | 5 | 3 | 4 |
| 4 | 10 | 5 | 2 | 3 |
| 5 | 9 | 5 | 3 | 3 |
| 6 | 9 | 6 | 3 | 3 |
| 7 | 9 | 6 | 2 | 3 |
| 8 | 10 | 6 | 3 | 3 |
| 9 | 8 | 5 | 3 | 3 |
| 10 | 9 | 5 | 3 | 3 |
| Mean score | 8.5 | 5.5 | 3.0 | 3.2 |
Observation of FFI score of the patients on various time scale.
| Case no. | Foot Function Index (FFI) score |
|---|
| Baseline/at time of enrollment | Day 14 | Day 28 | Day 56 |
|---|
| 1 | 75 | 55 | 45 | 44 |
| 2 | 89 | 64 | 29 | 41 |
| 3 | 86 | 58 | 30 | 35 |
| 4 | 72 | 63 | 41 | 44 |
| 5 | 93 | 59 | 30 | 37 |
| 6 | 96 | 61 | 46 | 40 |
| 7 | 91 | 57 | 34 | 41 |
| 8 | 82 | 68 | 32 | 38 |
| 9 | 76 | 58 | 46 | 40 |
| 10 | 90 | 59 | 43 | 41 |
| Mean score | 85 | 60 | 38 | 40 |
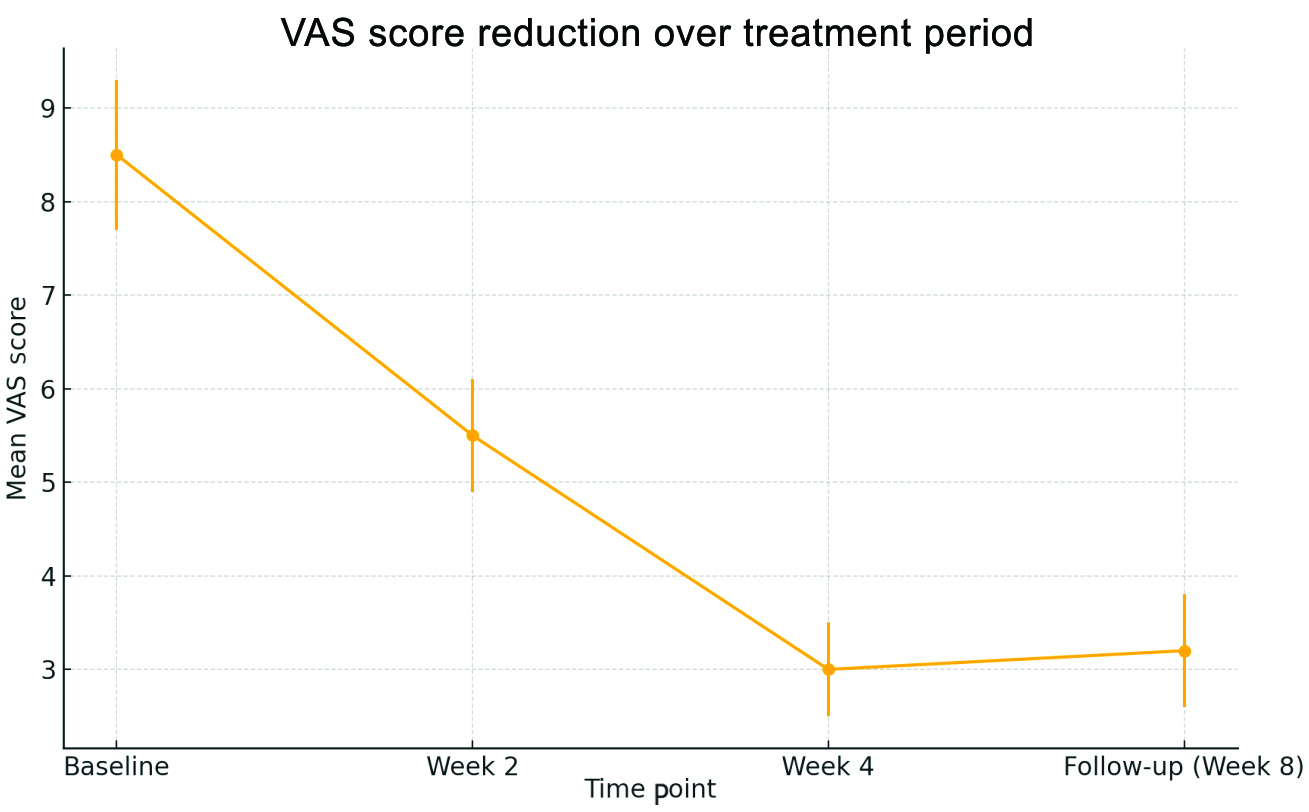
At the start of the treatment, the mean VAS score [9] for pain among the patients was 8.5. By the end of the four-week treatment period, the mean VAS score had decreased to 3.0, representing a 65% reduction in pain [Table/Fig-6]. In addition to the VAS scores, physical examinations conducted showed a marked decrease in tenderness at the calcaneal tuberosity, a common site of pain in plantar fasciitis.
Graphical representation of VAS score.
From the patient’s perspective, there was a notable improvement in both pain and functionality, as measured by the Foot Function Index (FFI) [10,11]. The FFI assesses foot impairment associated with pain, disability and activity limitation. It is a self-administered index composed of 23 items divided into three subscales: pain (9 items), disability (9 items) and activity limitation (5 items), all scored on a Likert scale from 0 to 10. The total score is then calculated as a percentage using the formula: (total score/230) × 100 =_%.
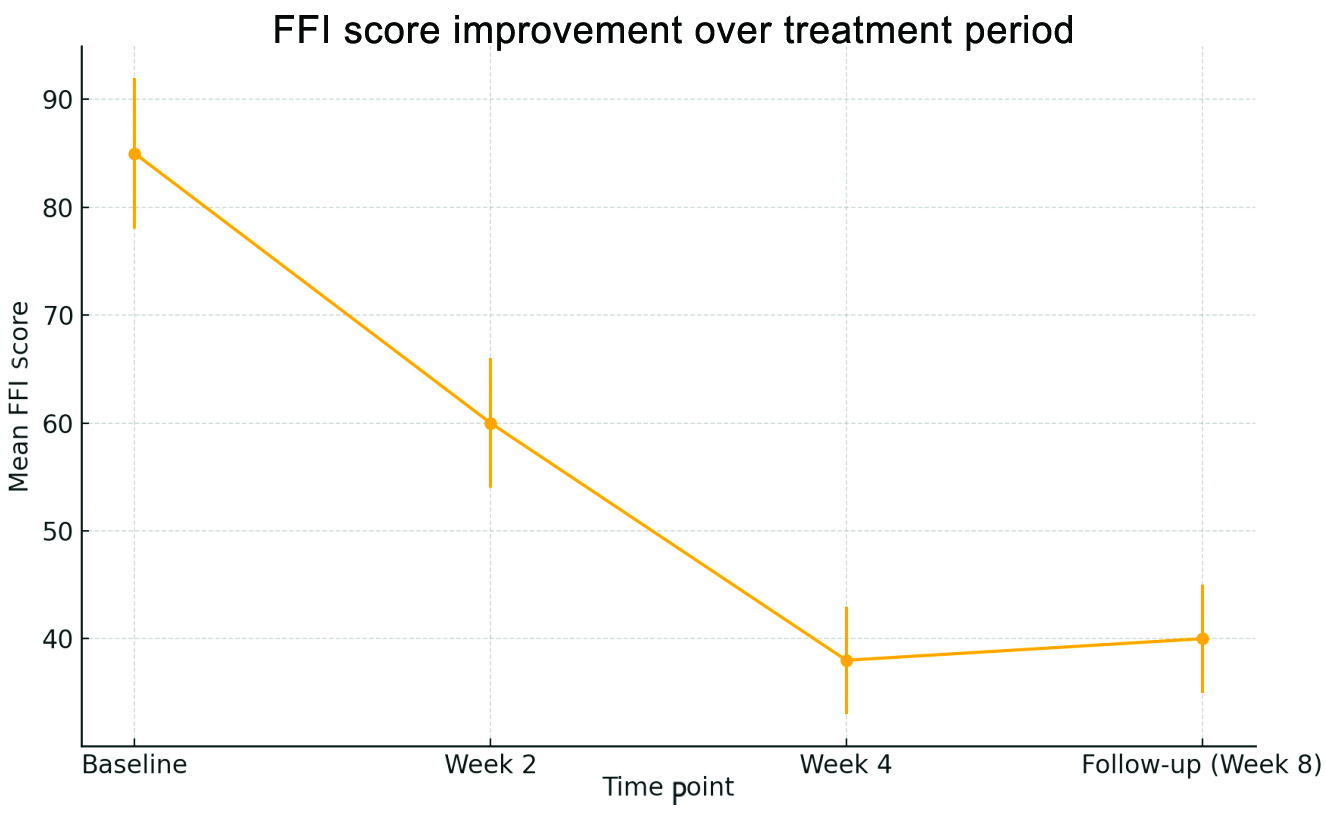
Initially, the mean FFI score was 85. After four weeks of treatment, the mean FFI score improved to 38, reflecting a 55% improvement in foot function [Table/Fig-7]. Patients reported an enhanced ability to perform daily activities, reduced pain during walking and standing, and an overall improved quality of life.
Graphical representation of FFI score.
Follow-up was conducted on the 8th week (day 56), and reassessment was performed using VAS and FFI scores. Intervention adherence was assessed through patient self-reporting, showing high tolerability with no adverse events reported.
Discussion
Plantar fasciitis typically resolves with non surgical methods, yielding a high resolution rate. However, individual responses vary due to differences in pathology, body types and lifestyles. Traditional treatments focus on reducing inflammation through methods such as NSAIDs, rest, corticosteroids and orthotic interventions. Alternatively, some therapies aim to address the underlying degeneration, often by inducing acute inflammation to initiate healing. These may include autologous blood or platelet-rich plasma injections, shock-wave therapy, or surgical options [12].
Agnikarma (thermo-cauterisation) is considered the gold standard Ayurvedic management for Vatkantak, showing significant results in patients [13]. Agnikarma performed with Panchdhatu Shalaka is more effective compared to the use of Madhuchista (beeswax) [14]. Raktamokshan, either through Siravedh [15] or Jalaukavcharan (leech therapy), is also recommended. Jalaukavcharan is particularly effective, as it acts locally and its saliva contains various enzymes with anti-inflammatory properties [16]. Eranda Tail Nitya Virechan combined with Kolakulathadi Upanaha has shown relief in heel pain in a case series involving 20 patients [17].
Pinda Thaila Abyanga, Rasnadi Sweda, followed by the application of Hingwadi Lepa, resulted in a 75% resolution of symptoms in 40% of patients [18]. Similarly, the present study found that a Lepa made from Nirgundi reduced VAS scores and improved the FFI in patients with plantar fasciitis.
The active compounds in Nirgundi, such as flavonoids, alkaloids and terpenoids, exhibit significant anti-inflammatory effects by inhibiting proinflammatory cytokines and enzymes [19]. Additionally, Nirgundi’s analgesic properties complement its anti-inflammatory actions, providing relief from pain associated with musculoskeletal disorders. This dual action makes it a promising natural remedy for various forms of musculoskeletal discomfort.
Limitations of the present case series include the small sample size and the need for larger randomised controlled trials to confirm these findings.
Conclusion(s)
The findings of the present case series suggest that Nirgundi Lepa is a promising non invasive treatment for plantar fasciitis, providing significant pain relief and improved functionality. These results imply that Nirgundi Lepa could be integrated into clinical practice as an effective alternative to conventional treatments. Future research should focus on larger, randomised controlled trials to confirm these findings and explore the long-term benefits and potential mechanisms of action of Nirgundi Lepa.
[1]. Vaidya U, Dholakiya H, Clinical aspect of effect of agnikarma with mrittikashalaka in vatakantaka w.s.r. to calcaneal spurXCV-III 2024 69-81. [Google Scholar]
[2]. Sharma M, Kumar S, To evaluate the effects of plantar fascia and tendo Achilles stretch in chronic plantar fasciitisPhysiother Occup Ther J 2020 13(3):115-22. [Google Scholar]
[3]. Schuitema D, Greve C, Postema K, Dekker R, Hijmans JM, Effectiveness of mechanical treatment for plantar fasciitis: A systematic reviewJ Sport Rehabil 2019 29(5):657-74.10.1123/jsr.2019-003631629333 [Google Scholar] [CrossRef] [PubMed]
[4]. Kumar D, Kumar R, Sharda K, Medicinal property of nirgundiJ Pharmacogn Phytochem 2018 7(1S):2147-51. [Google Scholar]
[5]. Jajra SD, Panwar N, Adlakha MK, Purvia RP, Vinod G, Chandan S, Role of (Vitex nigundo) nirgundi in pain managementWorld J Pharm Res 2019 8(7):2083-89. [Google Scholar]
[6]. Buchanan BK, Sina RE, Kushner D, Plantar fasciitis. [Updated 2024 Jan 7]In: StatPearls [Internet] 2024 Jan Treasure Island (FL)StatPearls PublishingAvailable from: https://www.ncbi.nlm.nih.gov/books/NBK431073/ [Google Scholar]
[7]. Nahin RL, Prevalence and pharmaceutical treatment of plantar fasciitis in United States adultsJ Pain 2018 19(8):885-96.10.1016/j.jpain.2018.03.00329597082 [Google Scholar] [CrossRef] [PubMed]
[8]. Bolgla LA, Malone TR, Plantar fasciitis and the windlass mechanism: A biomechanical link to clinical practiceJ Athl Train 2004 39(1):77-82. [Google Scholar]
[9]. Katz J, Melzack R, Measurement of painSurg Clin North Am 1999 79(2):231-52.10.1016/S0039-6109(05)70381-910352653 [Google Scholar] [CrossRef] [PubMed]
[10]. Budiman-Mak E, Conrad KJ, Roach KE, The foot function index: A measure of foot pain and disabilityJ Clin Epidemiol 1991 44(6):561-70.10.1016/0895-4356(91)90220-42037861 [Google Scholar] [CrossRef] [PubMed]
[11]. Foot Function Index (FFI) [Internet]PhysiopediaAvailable from: https://www.physio-pedia.com/Foot_Function_Index_(FFI) [Google Scholar]
[12]. Pandey S, Kumar N, Kumar A, Biswas A, Sinha U, Pandey J, Extracorporeal shockwave therapy versus platelet rich plasma injection in patients of chronic plantar fasciitis: A randomized controlled trial from a tertiary center of Eastern IndiaCureus 2023 15(1):e34430eCollection 2023 Jan10.7759/cureus.34430 [Google Scholar] [CrossRef]
[13]. Ghodela NK, Singh N, Khobbanna B, Heel pain and agnikarma: An ayurved approachWorld J Pharm Res 2017 6(3):342-50. [Google Scholar]
[14]. Hiremata V, Balaraddi SL, A randomized controlled trial to evaluate the effect on pain by agnikarma with madhuchista (bee wax) and panchaloha shalaka in vatakantakaJ Ayurveda Integr Med Sci 2020 5(05):78-88.10.21760/jaims.5.5.10 [Google Scholar] [CrossRef]
[15]. Solanki B, Meher A, Bhatted SK, Dharmarajan P, Management of plantar fasciitis with raktamokshana and shamana chikitsa in Ayurveda: A case studyJ Indian Syst Med 2021 9(1):59-63.10.4103/JISM.JISM_111_20 [Google Scholar] [CrossRef]
[16]. Nambiar VK, George MJ, Jalaukā vacaraṇa in plantar fasciitisInt Ayurvedic Med J 2020 8:4724-31.10.46607/iamj2308102020 [Google Scholar] [CrossRef]
[17]. Rao VG, Nischitha MS, Ayurvedic management of vatakantaka (plantar fasciitis)Int J Ayurvedic Med 2013 4(1):43-49.10.47552/ijam.v4i1.243 [Google Scholar] [CrossRef]
[18]. Pramodani MPN, Wickramarachchi WJ, A clinical study to evaluate the efficacy of selected treatment modality in the management of vatakantakaInt J Res Granthaalayah 2017 5(1):282-90.10.5281/zenodo.264253 [Google Scholar] [CrossRef]
[19]. Banik B, Das S, Das MK, Medicinal plants with potent anti-inflammatory and anti-arthritic properties found in eastern parts of the Himalaya: An ethnomedicinal reviewPharmacogn Rev 2020 14(28):121-37.10.5530/phrev.2020.14.16 [Google Scholar] [CrossRef]