Introduction
Computed Tomography (CT) scans account for only 15% of total diagnostic procedures but for over half of the collective dose of radiation. The increasing awareness about the harmful effects of radiation has also created a need for developing techniques that decrease radiation exposure while at the same time providing a reasonably good image quality. The majority of the CT units today use Filtered Back Projection (FBP) as the means of image reconstruction. However, FBP leads to coupling between image noise and radiation exposure and limits the dose reduction possible while providing diagnostic quality images. Second-generation Iterative Reconstruction (IR) techniques have caught the attention of medical researchers because they provide a superior image quality than FBP at the same radiation dose showing potential for dose reduction.
Aim
To compare the image quality and radiation dose in standard dose CT head reconstructed with FBP and low dose CT head reconstructed with Sinogram Affirmed Iterative Reconstruction (SAFIRE) and FBP both.
Materials and Methods
A cross-sectional analytical study was conducted on 100 patients in the emergency department of Vardhman Mahavir Medical College and Safdarjung Hospital in India from November 2018 to April 2020. Patients referred for emergency Non-contrast Computed Tomography (NCCT) head for any indication excluding post-op cases and those with metallic artifacts were included. Fifty patients chosen using systematic random sampling underwent low-dose CT head using the Care Dose 4D Automatic Exposure Control (AEC) system with reconstruction using SAFIRE (Group-A) and FBP (Group-B). Another 50 patients who were within five years of the corresponding Group-A and B patients underwent standard dose head CT reconstruction using FBP (Group-C). CTDI vol, DLP, and effective dose were recorded in all patients. Image quality was assessed objectively using the unpaired t-test for Group-A and C and paired t-test for Group-A and B. Subjective image analysis between the groups was done using a 4-point Likert scale.
Results
Image quality parameters were found to be better in Group-A compared to Group-C (p<0.05). The mean values in low dose SAFIRE group, low dose FBP group, and standard dose FBP group were as follows: Grey Matter (GM) Signal-to-Noise Ratio (SNR) (14±3.29, 8.96±2 and 9.24±1.96), White Matter (WM) SNR (14.6±3.73, 6.9±3.79 and 7.11±1.68), Cerebrospinal Fluid (CSF) SNR (1.65±1.12, 0.86±0.80 and 1.08±0.61) and Contrast-to-Noise Ratio (CNR) (3.06±0.94, 1.81±0.69 and 1.74±0.69), respectively. Group-A had significantly improved image quality parameters than Group-B and Group-C. Radiation dose reduction of 42%, 39.34%, and 42.5% was achieved in CTDIvol, DLP, and effective dose respectively in low dose group.
Conclusion
Low dose CT head reconstructed with SAFIRE were significantly better in image quality compared to standard-dose CT head images reconstructed using FBP, while allowing for up to 42% reduction in dose.
Introduction
The growing use of CT which accounts for only 15% of total diagnostic procedures but for over half of the collective dose of diagnostic radiation has created an increasing concern for radiation exposure. The radiation exposure during an NCCT exam is 2.1 mSv which is nearly twice the recommended dose by Atomic Energy Regulatory Board (AERB) for the general population [1]. Efforts have been made to acquire low-dose CT in the past using tube current modulation and noise reduction filters. However, these methods are limited by simultaneous compromises in image quality. Therefore, other avenues like image reconstruction techniques have been explored to achieve further dose reduction [2,3].
Majority of the current CT units use FBP as the means of image reconstruction. However, FBP leads to coupling between image noise and radiation exposure which limits the dose reduction possible [4]. The IR techniques had limited use when they were initially introduced in the 1970s owing to the long computational process, however with recent technological advancements the use of IR is becoming popular as it provides a superior image quality than FBP at the same radiation dose [5]. It is postulated that IR reconstruction methods like SAFIRE improve contrast, increase SNR, CNR, and noise texture, and show potential for dose reduction [6]. However the extent of dose reduction possible with SAFIRE has not been elucidated in literature.
The purpose of this study was to compare the image quality between FBP and SAFIRE reconstructed images and check the extent of radiation dose reduction possible using SAFIRE in CT head.
Materials and Methods
A cross-sectional analytical study was carried out on 100 patients in the emergency department of Vardhman Mahavir Medical College and Safdarjung Hospital in India from November 2018 to April 2020. Institutional Ethics Committee (IEC) approval (IEC Approval number: 2018-78) was obtained.
Inclusion and Exclusion criteria: Patients who were advised NCCT head for any emergency indication such as loss of consciousness, suspected CVA, severe headache, etc., were included. Patients undergoing NCCT head for postoperative check status, and patients with NCCT images showing motion blur and metallic artifacts were excluded from the study.
Fifty cases were selected by systematic random sampling where the first patient on every Monday underwent low-dose CT with reconstruction using both SAFIRE (Group-A) and FBP (Group-B). The subsequent patient presenting on the same day for emergency NCCT head who fulfilled the inclusion criteria and was within five years of age of the previous patient underwent standard dose CT reconstructed with FBP (Group-C). This patient served as the age-matched control of the previous subject.
Data acquisition and reconstruction: Scanning was performed on Siemens 256-slice Dual-source CT scanner. Image acquisition parameters were as follows: slice thickness 0.6 mm, pitch 0.55, FOV 200 mm, collimation 1×1 mm, rotation time 1s. In controls, kVp was set at 120 for adults and 100 for children whereas mAs was set at 390 for adult and 338 for children. In cases, kVp and mAs were automatically calculated by integrated automatic exposure control device Care Dose 4D and Care kV. For standardisation purposes, SAFIRE strength level of three was used in all cases.
Radiation dose measurements: CTDIvol, DLP and effective dose of all cases and controls were recorded from the dose report available with every scan. The mean effective doses were obtained by multiplying the DLP with tissue factor for head i.e., 0.0021 mSv/(mGy×cm) according to European commissioned published guidelines [7].
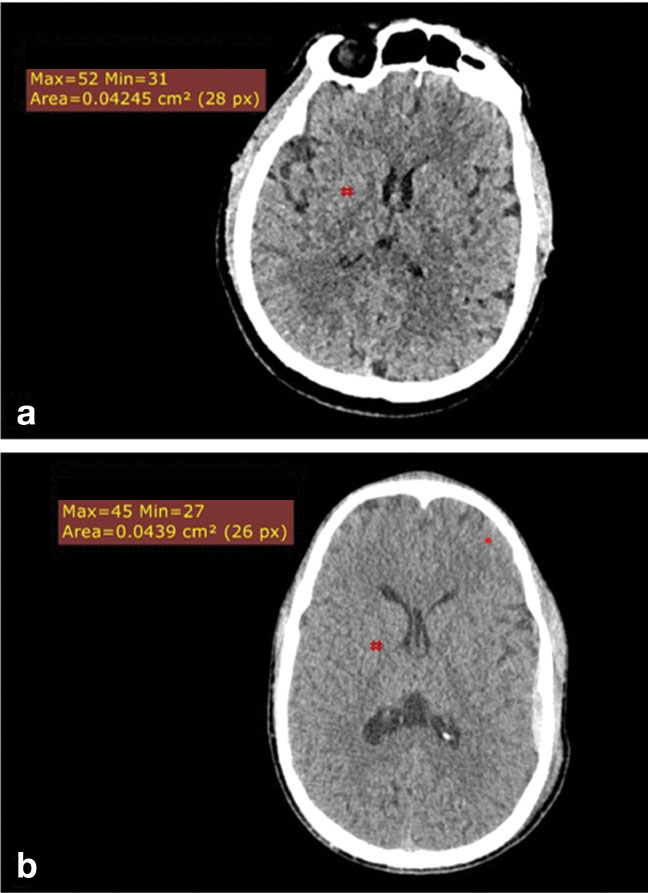
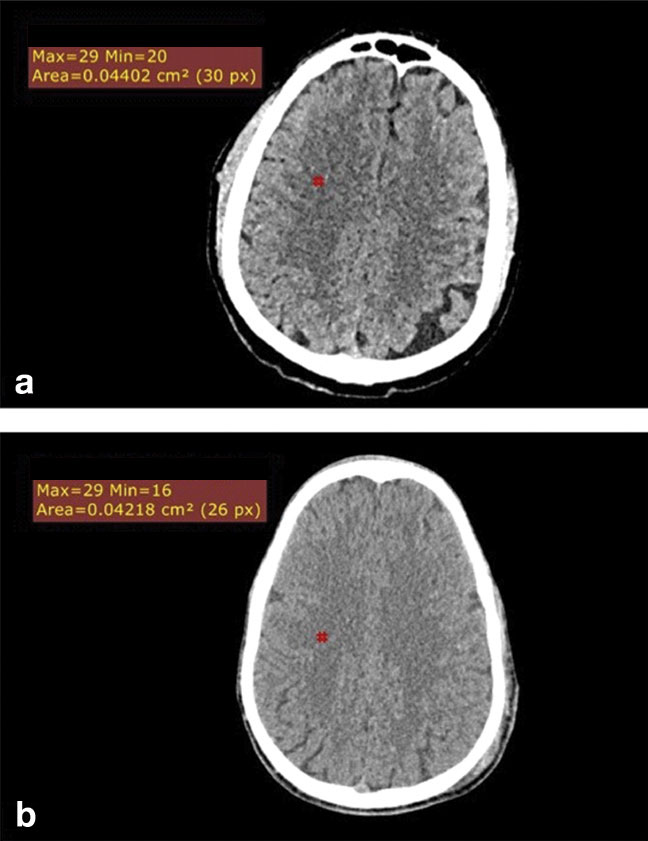
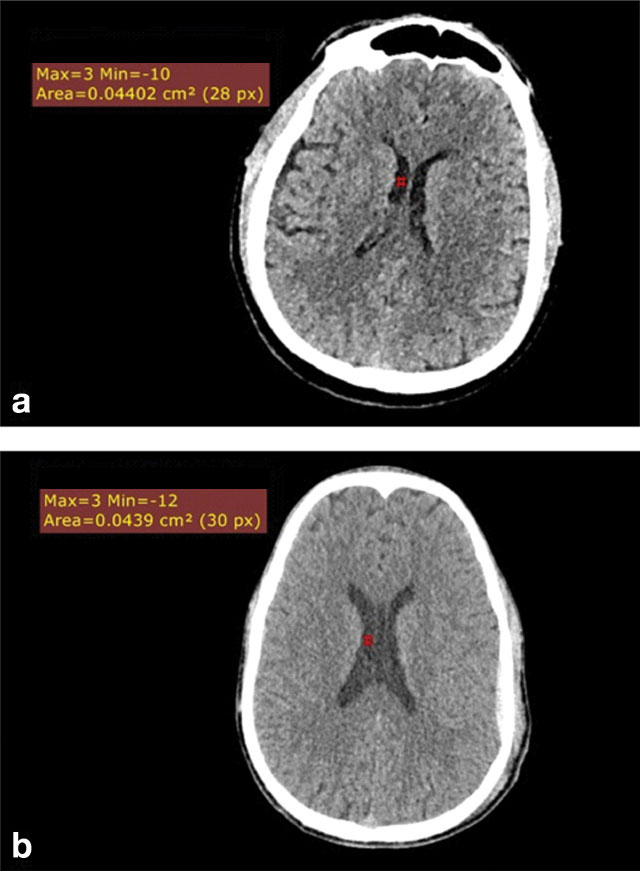
Quantitative image analysis: Quantitative image analysis was performed by a single reader blinded to the image protocol. Images were anonymised for Region of Interest (ROI) placements. A 4 mm sq. Region of Interest ROI was placed in GM in the lentiform nucleus, WM in the centrum semiovale and CSF in the lateral ventricle [Table/Fig-1,2 and 3]. Signal was measured as the CT density in Hounsfield Unit (HU) and noise was measured as the Standard Deviation (SD) of attenuation in the ROI. SNR and CNR was then calculated using following formulas:
Mean image noise was calculated as an average of sums of individual SDs of attenuation values in cases and controls, respectively.
A 4 mm sq ROI placement in right lentiform nucleus in Grey Matter (GM) in low dose SAFIRE subset [Table/Fig-1a]; and in standard dose FBP subset [Table/Fig-1b].
A 4 mm sq ROI placement in right centrum semiovale in White Matter (WM) in low dose SAFIRE subset [Table/Fig-2a]; and standard dose FBP subset [Table/Fig-2b].
4 mm sq ROI placement in right lateral ventricle in low dose SAFIRE subset [Table/Fig-3a]; and standard dose FBP subset [Table/Fig-3b].
Qualitative image analysis: Qualitative image analysis was performed between the cases (low dose CT reconstructed with SAFIRE) and controls (standard dose CT reconstructed with FBP) on a 4-point Likert scale as detailed in [Table/Fig-4]. Images were analysed by two radiologists with 4 and 20 years of experience and any differences were resolved by consensus.
A 4-Point Likert scale for qualitative image analysis.
| Parameters | Score 1 | Score 2 | Score 3 | Score 4 |
|---|
| Noise | Very low | Low | Considerable but diagnostic | High and non-diagnostic |
| GM-WM differentiation | Excellent | Good | Suboptimal but diagnostic | Unacceptable and non-diagnostic |
| Sharpness of Subarachnoid space margins | Excellent | Good | Suboptimal but diagnostic | Unacceptable and non-diagnostic |
| Posterior fossa beam hardening | Excellent | Good | Suboptimal but diagnostic | Unacceptable and non-diagnostic |
| Visibility of small structures like VR spaces, small vessels, cranial nerves | Excellent | Good | Suboptimal but diagnostic | Unacceptable and non-diagnostic |
| Overall diagnostic acceptability | Excellent | Good | Suboptimal but diagnostic | Unacceptable and non-diagnostic |
Statistical Analysis
The data for all patients was entered in MS Excel Spreadsheet and analysed using SPSS version 21.0. Intraobserver variation for the repeated attenuation measurements was assessed with the coefficient of repeatability. Comparison for quantitative image assessment between standard dose-FBP and low dose-SAFIRE images was done by unpaired t-test. Comparison for quantitative image assessment between low dose FBP and low dose SAFIRE images was done by paired t-test. Significance level was taken at p<0.05.
Results
Coefficient of repeatability: No significant difference was found between the three intraobserver readings taken in GM, WM, and CSF in all three subsets. However, significant difference was found in the noise readings of GM and WM in the low dose FBP group [Table/Fig-5].
Coefficient of Repeatability in the three subsets.
| Coefficient of repeatability |
|---|
| Cases | Controls |
|---|
| | Low doseSAFIRE | Low doseFBP | Standard dose FBP |
|---|
| | CoR | p-value | CoR | p-value | CoR | p-value |
|---|
| GM | Signal (HU) | 1.26 | 0.37 | 2.50 | 0.12 | 2.21 | 0.11 |
| Noise (SD) | 1.36 | 0.10 | 5.52 | <0.001 | 0.78 | 0.67 |
| WM | Signal (HU) | 1.15 | 0.35 | 1.88 | 0.11 | 2.01 | 0.59 |
| Noise (SD) | 1.13 | 0.09 | 1.87 | 0.004 | 0.90 | 0.60 |
| CSF | Signal (HU) | 2.19 | 0.28 | 2.27 | 0.13 | 4.18 | 0.09 |
| Noise (SD) | 0.48 | 0.66 | 1.23 | 0.09 | 0.72 | 0.78 |
Quantitative image analysis: The mean GM SNR, WM SNR, CSF SNR, and CNR were found to be significantly higher in low-dose CTs reconstructed with SAFIRE (mean value 14±3.2, 14.6±3.7, 1.65±1.12 and 3.06±0.94, respectively) than with standard dose CTs reconstructed with FBP (mean value 9.24±1.96, 7.11±1.68, 1.08±0.61 and 1.81±0.69, respectively) with p-values <0.001, <0.001, 0.002 and <0.001, respectively [Table/Fig-6]. Image quality parameters of low dose FBP group when compared to low dose SAFIRE group showed significantly lower mean GM SNR, WM SNR, CSF SNR, and CNR values- 8.96±2, 6.9±3.79, 0.86±0.80, and 1.70±0.85, respectively with significant p-values (<0.001, <0.001, 0.002 and <0.001, respectively).
A significant noise reduction was also seen in images reconstructed with SAFIRE compared to FBP [Table/Fig-7]. Image noise was found to be lowest in the case group (low-dose CT reconstructed with SAFIRE) and highest in low-dose CT reconstructed with FBP. Within the low-dose images, noise was lower when reconstruction was done using SAFIRE compared to FBP. Mean noise reduction was 31.2% in GM, 30% in WM, and 26.2% in CSF in low-dose images reconstructed with SAFIRE when compared to standard dose FBP images.
Quantitative image analysis in cases (low dose CT reconstructed with SAFIRE and FBP) and controls (standard dose CT reconstructed with FBP).
| Quantitative image analysis |
|---|
| Low doseSAFIRE | Low doseFBP | Standard doseFBP |
|---|
| Gray matter SNR |
| Mean±SD | 14±3.29 | 8.96±2 | 9.24±1.96 |
| Median | 13.44 | 8.62 | 8.79 |
| Min-Max | 9.08-26 | 5.67-13.75 | 5.29-15.25 |
| Interquartile range | 9.08-15.22 | 7.41-10.30 | 8-10.50 |
| White Matter (WM) SNR |
| Mean±SD | 14.6±3.73 | 6.9±3.79 | 7.11±1.68 |
| Median | 13.67 | 6.88 | 7.0 |
| Min-Max | 9.88-26.33 | 4.63-9.88 | 4.11-12.33 |
| Interquartile range | 12-16.20 | 6.1-7.5 | 4.11-7.85 |
| CSF SNR |
| Mean±SD | 1.65±1.12 | 0.86±0.80 | 1.08±0.61 |
| Median | 1.67 | 0.76 | 1 |
| Min-Max | -1.29-4.6 | -0.63-3.71 | -0.64-2.5 |
| Interquartile range | 1-2.28 | 0.4-1.21 | -0.69-1.56 |
| CNR |
| Mean±SD | 3.06±0.94 | 1.70±0.85 | 1.81±0.69 |
| Median | 2.89 | 1.56 | 1.85 |
| Min-Max | 0.81-4.99 | 0.62-3.62 | 0.32-4.46 |
| Interquartile range | 2.41-3.79 | 1.41-2.29 | 1.29-2.18 |
Image noise analysis in low dose images reconstructed with SAFIRE and FBP with standard dose images reconstructed with FBP.
| Low doseSAFIRE | Low doseFBP | Standard doseFBP |
|---|
| Image noise in gray matter |
| Mean | 2.79 | 4.16 | 4.06 |
| Median | 2.67 | 4 | 4 |
| Min-Max | 1.33-4 | 2.67-7 | 2.66-6 |
| Image noise in White Matter (WM) |
| Mean | 2.61 | 3.85 | 3.73 |
| Median | 2.67 | 3.83 | 3.67 |
| Min-Max | 1.33-4.3 | 2.33-5.3 | 2-6 |
| Image noise in CSF |
| Mean | 2.87 | 4.11 | 3.89 |
| Median | 2.67 | 4 | 3.33 |
| Min-Max | 1.67-6 | 2-7 | 2.67-6.33 |
Qualitative image analysis: The difference in mean readings between readers 1 and 2 was statistically insignificant (p>0.05) in both cases and controls [Table/Fig-8]. Assessment of subjective image quality showed no significant difference between standard dose images reconstructed by FBP and low dose images reconstructed by SAFIRE in all parameters for reader 1 (p>0.05). For reader 2, a significant difference was seen in the posterior fossa beam hardening artifact in the case and control group (p=0.001) implying that the case group had slightly better image quality.
Qualitative image analysis between cases (low dose image reconstructed with SAFIRE) and controls (standard dose images reconstructed with FBP).
| Parameters | Case(n=50) | Control(n=50) | p-value |
|---|
| Noise (Reader 1) | 1.68±0.59 | 1.52±0.58 | 0.162 |
| GM-WM differentiation (Reader 1) | 1.46±0.58 | 1.42±0.54 | 0.785 |
| Sharpness of SAS (Reader 1) | 1.48±0.58 | 1.46±0.58 | 0.852 |
| PF Beam hardening (Reader 1) | 1.74±0.69 | 1.86±0.53 | 0.246 |
| Visibility of small structures (Reader 1) | 1.80±0.64 | 1.72±0.50 | 0.614 |
| Diagnostic acceptability (Reader 1) | 1.86±0.67 | 1.64±0.66 | 0.095 |
| Total (Reader 1) | 10.02±3.18 | 9.62±2.67 | 0.661 |
| Noise (Reader 2) | 1.70±0.61 | 1.52±0.58 | 0.138 |
| GM-WM differentiation (Reader 2) | 1.52±0.65 | 1.44±0.54 | 0.661 |
| Sharpness of SAS (Reader 2) | 1.58±0.57 | 1.48±0.58 | 0.350 |
| PF Beam hardening (Reader 2) | 1.66±0.48 | 1.96±0.40 | 0.001 |
| Visibility of small structures (Reader 2) | 1.86±0.67 | 1.64±0.66 | 0.095 |
| Diagnostic acceptability (Reader 2) | 1.90±0.58 | 1.78±0.62 | 0.301 |
| Total (Reader 2) | 10.22±2.78 | 9.82±2.40 | 0.402 |
Radiation dose comparison: CTDIvol, DLP and effective dose were significantly higher in control group (48.59±6.03, 846.37±125.25 and 1.88±0.44, respectively) than in the case group (29.47±3.53, 486.49±70.11 and 1.09±0.32, respectively) with p-value <0.001 in all [Table/Fig-9]. The total dose reduction was found to be 42%.
Radiation dose comparison between cases and controls.
| Parameters | Case (Low dose group reconstructed with SAFIRE and FBP) | Control (Standard dose group reconstructed with FBP) |
|---|
| CTDIvol |
| Mean | 29.47±3.53 | 48.59±6.03 |
| Median | 29.44 | 49.06 |
| Min-Max | 19.3-38.9 | 29.8-62.26 |
| Interquartile range | 28.79-31.60 | 46.70-71.70 |
| Dose length product |
| Mean | 486.49±70.11 | 846.37±125.25 |
| Median | 480.6 | 843.6 |
| Min-Max | 304.5-670 | 494.2-1138.6 |
| Interquartile range | 438.50-528.20 | 804.60-924.60 |
| Effective dose |
| Mean | 1.09±0.32 | 1.88±0.44 |
| Median | 1.01 | 1.8 |
| Min-Max | 0.64 -2.58 | 1.04-3.79 |
| Interquartile range | 0.94-1.13 | 1.70-1.98 |
Discussion
In the present study used two different groups of subjects as cases and controls for ethical reasons. To perform the same group comparison, many of the previous authors have used the data from a single tube of a dual-source CT scanner for reconstructing half-dose images [8-10]. This is possible with a dual-source CT scanner which allows comparison of full-dose and half-dose CT images in the same patient keeping other parameters similar. The downside to this method is that it only allows an absolute reduction of 50% and does not allow any further exploration into dose reduction. To overcome this factor in the present study, we used automatic exposure control called Care Dose 4D and Care kV to reconstruct low-dose images. Care Dose 4D system performs automatic tube current modulation according to patient size and x-ray attenuation changes together with real-time tube current modulation during each tube rotation. CARE kV is designed to automate kV selection to optimise the CNR for a given diagnostic task. This methodology of low-dose CT acquisition appears slightly superior as it avoids unnecessary over or underexposure in subjects with different body habitus.
Gender and Age Distribution
Majority of the previous authors who did intra-patient dose comparisons like Mitsumori LM et al., and Marin D et al., employed small sample sizes for ethical reasons and limited availability of patients fulfilling inclusion criteria [11,12]. On the other hand, May MS et al., incorporated a larger sample population as they used data from one tube to reconstruct half-dose CT images [8]. The present study employed a large sample size as we utilised vendor-specified pre-set dose reduction protocols and used two different age-matched populations as cases and controls. Most of the previous authors based their study on either adult or pediatric population [11,13-16]. This study included patients from all age groups with age range of subjects varying from 1 to 90 years.
Effect on Image Quality Parameters and Image Noise
The present study showed that images reconstructed with SAFIRE had better subjective and objective image quality parameters compared to images reconstructed with FBP at both standard dose and low dose with a significant amount of noise reduction. Within the low-dose images, improved SNR and CNR values were seen when reconstruction was done using SAFIRE suggesting that improvement in low-dose CT image quality was due to IR.
Korn A et al., conducted a study on head NCCTs and found an increase of 28% in GM SNR, 31% in WM SNR, and 25 % in the CNR between low-dose CT and standard-dose CT [2]. This study found an increase of 34%, 51.3%, and 43.1% in GM SNR, WM SNR and CNR respectively suggesting that IR not only compensates for the degradation in image quality at lower radiation dose but may even provide a better image quality. Other authors such as Rivers-Bowerman MD and Shankar JJS found higher SNR and CNR values compared to the present study (55% in GM SNR, 35% in WM SNR, and 72% in CNR) in SAFIRE reconstructed scans compared to the FBP reconstructed scans [3].
Majority of the previous studies observed that IR-reconstructed images had a blotchy pixelated appearance which was also seen in current study’s SAFIRE-reconstructed images and this appearance increased with higher strength of iteration from S1 to S5 [15,17,18]. According to Kalra MK et al., lower iterative strengths were associated with a low level of image noise reduction while higher iterative strengths were associated with overly smoothened images [19]. A three-phase phantom-based study performed by Harris MA et al., showed that increasing strengths of IR gave a lower pixel noise and increased CNR, concluding that IR has the potential to affect the pixel noise, image texture, and CNR while maintaining image quality [20]. Due to the above reasons, this study design incorporated a single iterative strength level of 3 for all low-dose CT acquisitions for uniformity. We used this strength level based on the recommendations of the vendor and the results of previous studies. The subjective image quality analysis done in this study showed that the quality of low-dose images reconstructed with SAFIRE was at par with the standard dose images reconstructed with FBP. Based on this we propose that the smoothness of the iteratively reconstructed images can be considered as an inherent property of the type of reconstruction and does not hamper the diagnostic accuracy of the scan.
The present study utilised a second-generation IR method which as per Hwang HJ et al., fared better at improving image quality compared to first-generation reconstruction methods [21]. A previous study by Bodelle B et al., also claims that the conspicuity of ischaemic infarcts was improved with IR [22]. We agree with this observation and also propose that low-dose iteratively reconstructed images are equivalent or even better at demonstrating a myriad of pathological findings such as cerebral infarcts, haemorrhagic contusions, extra-axial bleeds, calcified granulomas etc., which were well demonstrated in the case group.
Effect on Radiation Dose
The present study found a reduction of 39.3% in CTDIvol, a 42.5 % reduction in DLP, and 42% reduction in effective dose in the low-dose subset compared to standard dose subset. The results of dose reduction achieved by various researchers has been summarised in [Table/Fig-10] [2,13,20,23-33].
Results of previous research studies on IR [2,13,20,23-33].
| Research authors | Place and year of study | Conclusion |
|---|
| Hara AK et al., [23] | Mayo Clinic Arizona, Scottsdale2009 | Low-dose CT reconstructed with ASIR allowed a 32-65% dose reduction compared to routine dose CT and had lesser noise. |
| Sagara Y et al., [24] | Mayo Clinic, Scottsdale andOita University Faculty of Medicine, Oita, Japan 2010 | The amount of dose reduction was more (66%) with people having BMI ≤20 and less (23%) with people having BMI ≥25. |
| Prakash P et al., [25] | Massachusetts General Hospital and Harvard Medical School, Boston, MA 2009 | Abdominal CTs reconstructed with ASIR allowed 25.1% decrease in CTDIvol compared with standard dose FBP-reconstructed images. |
| Leipsic J et al., [26-28] | University of British Columbia, Vancouver, BC, Canada2010 | They conducted three studies out of which the first study predicted that 17% noise reduction was possible with 40% ASIR-FBP combination; second study demonstrated a 27% dose reduction with ASIR without any significant change in image quality and third study showed that ASIR was associated with a lower noise level and better image quality at a lower radiation dose compared to FBP. |
| Pontana F et al., [29] | University Lille Norde de France, and Hospital Calmette, France2011 and 2013 respectively | They showed that IRIS with three iterations provided the same quality image as standard dose FBP at a 35% reduced radiation dose. |
| Willemink MJ et al., [30] | Utrecht University Medical Center, Utrecht and Gelre Hospital, Apeldoorn, The Netherlands 2013 | They reported dose reduction between 23-76% with IR. |
| Rapalino O et al., [31] | Massachusetts General Hospital, Boston, Massachusetts 2011 | They concluded that at 20-40% dose reduction, the SNR values of ASIR reconstructed images were comparable to routine dose images. |
| Korn A et al., [2] | Eberhard-Karls-University, Tubingen, Germany 2012 | They concluded that SAFIRE allows a dose reduction of 20% with improved image quality. |
| Vorona GA et al., [13] | Allegheny General Hospital, and Children’s Hospital of Pittsburgh of the University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania 2012 | They found that approximately 22% dose reduction was possible with 20% ASIR-FBP combination. |
| Wang R et al., [32] | Beijing Anzhen Hospital, Capital Medical University, Beijing, China; and Medical University of South Carolina, USA 2012Shandong University, Shandong Medical Imaging Research Institute,2013 | They found a 50% dose reduction in IR subset. |
| Harris MA et al., [20] | Mid Yorkshire Hospitals NHS Trust, Pinderfields General Hospital, Wakefield, UK; andSchool of Healthcare, Faculty of Medicine and Health, University of Leeds, Leeds, UK 2017 | They proposed that the maximum dose reduction possible in head CT using SAFIRE was 24%. |
| Pickhardt PJ et al., [33] | University of Wisconsin School of Medicine and Public Health, Clinical Science Centre, Madison 2012 | They found aggressive dose reductions to the extent of 74% in abdominal CT reconstructed with MBIR. |
Korn A et al., studied the potential of IR in NCCT head using SAFIRE. They proposed a 20% radiation dose reduction in NCCT head with mean CTDIvol being 47.8 mGy and mean DLP 829±35 mGy.cm in their low dose dataset [34]. The values in the present study were 29.47±3.53 mGy and 486.49±6.03 mGy.cm, respectively which are significantly less than that obtained by Korn A et al., [34]. This can be explained by the method employed for dose reduction. While Korn A et al., used tube current modulation to obtain low dose dataset, we employed automatic exposure and kV control (Care Dose 4D and Care kV) that amounted to a larger dose reduction. The extent of subjective image quality improvement was also found to be higher in this study [34].
Vorona GA et al., achieved a very low dose reduction of 22% in their study on paediatric head CT. However, their study was conducted on the Alderson-Rando phantom using a different reconstruction algorithm (ASIR) which can explain the variation in results from this study [13].
A few studies such as that by Pickhardt PJ et al., demonstrated aggressive dose reduction to the extent of 74% in abdominal CT [33]. As of today, such aggressive dose reductions are possible only with pure IR methods like MBIR which was used in their study. Hybrid reconstruction techniques like SAFIRE may not be capable of extensive dose reductions but are more suitable for incorporation into routine settings. According to Hara AK et al., a dose reduction of >50% was possible only if image quality in the area outside the ROI was compromised [23].
Feasibility of IR in Routine Setting
Scanning time is an important factor while determining the feasibility of routine use of IR technique. The earlier iterative techniques were associated with longer reconstruction times. According to May MS et al., IRIS (first generation IR algorithm) consumed six times the reconstruction time compared to FBP which proved to be a major limitation [8]. However, use of a second-generation IR algorithm SAFIRE did not lead to any significant computational delay in this study. The mean scan time was eight seconds in the thin slice low dose CT reconstructed with SAFIRE and seven seconds in the standard dose CTs reconstructed with FBP suggesting no significant delay in the scan timings between the two methods. This is compatible with incorporation of IR in routine settings. However, it should be emphasised that this is true for only hybrid IR algorithms and not pure IR methods in which the computational time still runs in hours [17,35].
In the present study fared superior to previous studies in a few areas. Firstly, the sample size was larger compared to previously performed studies and we included patients from all age groups from infants to the elderly population. Secondly, a second-generation IR technique that is routinely available in modern CT scanners was evaluated. Hence, incorporation of these in routine settings would not involve additional capital. Thirdly, size-based automatic exposure and kV control which customised the dose reduction to each patient were used.
Limitation(s)
There were certain limitations of the present study. Due to ethical reasons, the study’s low-dose dataset was obtained on a different set of populations. Hence, the ideal intra-patient comparison was not feasible. The present study did not categorise the extent of dose reduction with respect to the BMI of the individual as dose reduction is expected to be more in people with a lower BMI. The study evaluated dose reduction for only non-contrast CT head whereas the extent of dose reduction varies in different regions of the body as well as in contrast scans.
Conclusion(s)
The IR compensates for image degradation in low-dose CT with improvement in image quality and a radiation dose reduction of 42% is possible in NCCT head without producing any significant delay in scanning, thus allowing incorporation of SAFIRE in routine clinical settings. Even though the study was restricted to only the NCCT head, the results of this study can be extrapolated to other regions of the body as well as to contrast scans. IR has shown dose reduction potential in abdominal scans and CT angiography scans which are associated with high radiation dose. This potential of IR can be applied in CT perfusion studies as well which expose the patients to enormous amount of radiation dose.
[1]. Smith-Bindman R, Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancerArch Intern Med 2009 169:2078 [Google Scholar]
[2]. Korn A, Fenchel M, Bender B, Danz S, Hauser TK, Ketelsen D, Iterative reconstruction in head CT: Image quality of routine and low-dose protocols in comparison with standard filtered back-projectionAm J Neuroradiol 2012 33:218-24. [Google Scholar]
[3]. Rivers-Bowerman MD, Shankar JJS, Iterative reconstruction for head CT: Effects on radiation dose and image qualityCan J Neurol Sci J Can Sci Neurol 2014 41:620-25. [Google Scholar]
[4]. Kalra MK, Maher MM, Toth TL, Hamberg LM, Blake MA, Shepard JA, Strategies for CT radiation dose optimizationRadiology 2004 230:619-28. [Google Scholar]
[5]. Willemink MJ, Noël PB, The evolution of image reconstruction for CT- from filtered back projection to artificial intelligenceEur Radiol 2019 29:2185-95. [Google Scholar]
[6]. Grant K, Raupach R, SAFIRE: Sinogram Affirmed Iterative Reconstruction (White Paper)Siemens Healthcare 2012 Available from: http://imaging.ubmmedica.com/all/editorial/diagnosticimaging/pdfs/SAFIRE.pdf. (Accessed September 15, 2023) [Google Scholar]
[7]. Shrimpton PC, Hillier MC, Lewis MA, Dunn M, National survey of doses from CT in the UK: 2003Br J Radiol 2006 79:968-80. [Google Scholar]
[8]. May MS, Wüst W, Brand M, Stahl C, Allmendinger T, Schmidt B, Dose reduction in abdominal computed tomography: Intraindividual comparison of image quality of full-dose standard and half-dose iterative reconstructions with dual-source computed tomographyInvest Radiol 2011 46:465-70. [Google Scholar]
[9]. Remer EM, Herts BR, Primak A, Obuchowski NA, Greiwe A, Roesel DM, Detection of urolithiasis: Comparison of 100% tube exposure images reconstructed with filtered back projection and 50% tube exposure images reconstructed with sinogram-affirmed iterative reconstructionRadiology 2014 272:749-56. [Google Scholar]
[10]. Schabel C, Fenchel M, Schmidt B, Flohr TG, Wuerslin C, Thomas C, Clinical evaluation and potential radiation dose reduction of the novel Sinogram-affirmed Iterative Reconstruction Technique (SAFIRE) in abdominal computed tomography angiographyAcad Radiol 2013 20(2):165-72. [Google Scholar]
[11]. Mitsumori LM, Shuman WP, Busey JM, Kolokythas O, Koprowicz KM, Adaptive statistical iterative reconstruction versus filtered back projection in the same patient: 64 channel liver CT image quality and patient radiation doseEur Radiol 2012 22:138-43. [Google Scholar]
[12]. Marin D, Nelson RC, Schindera ST, Richard S, Youngblood RS, Yoshizumi TT, Low-tube-voltage, high-tube-current multidetector abdominal ct: Improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm—initial clinical experienceRadiology 2010 254:145-53. [Google Scholar]
[13]. Vorona GA, Zuccoli G, Sutcavage T, Clayton BL, Ceschin RC, Panigrahy A, The use of adaptive statistical iterative reconstruction in pediatric head CT: A feasibility studyAm J Neuroradiol 2013 34:205-11. [Google Scholar]
[14]. Southard RN, Bardo DME, Temkit MH, Thorkelson MA, Augustyn RA, Martinot CA, Comparison of iterative model reconstruction versus filtered back-projection in pediatric emergency head ct: Dose, image quality, and image-reconstruction timesAm J Neuroradiol 2019 40:866-71. [Google Scholar]
[15]. Khawaja RDA, Singh S, Otrakji A, Padole A, Lim R, Nimkin K, Dose reduction in pediatric abdominal CT: Use of iterative reconstruction techniques across different CT platformsPediatr Radiol 2015 45:1046-55. [Google Scholar]
[16]. Baker ME, Dong F, Primak A, Obuchowski NA, Einstein D, Gandhi N, Contrast-to-noise ratio and low-contrast object resolution on full- and low-dose MDCT: SAFIRE versus filtered back projection in a low-contrast object phantom and in the liverAm J Roentgenol 2012 199:08-18. [Google Scholar]
[17]. Katsura M, Sato J, Akahane M, Matsuda I, Ishida M, Yasaka K, Comparison of pure and hybrid iterative reconstruction techniques with conventional filtered back projection: Image quality assessment in the cervicothoracic regionEur J Radiol 2013 82:356-60. [Google Scholar]
[18]. Padole A, Singh S, Ackman JB, Wu C, Do S, Pourjabbar S, Submillisievert chest CT With filtered back projection and iterative reconstruction techniquesAm J Roentgenol 2014 203:772-81. [Google Scholar]
[19]. Kalra MK, Woisetschläger M, Dahlström N, Singh S, Digumarthy S, Do S, Sinogram-affirmed iterative reconstruction of low-dose chest CT: Effect on image quality and radiation doseAm J Roentgenol 2013 201:W235-44. [Google Scholar]
[20]. Harris MA, Huckle J, Anthony D, Charnock P, The acceptability of iterative reconstruction algorithms in head CT: An Assessment of Sinogram Affirmed Iterative Reconstruction (SAFIRE) vs. Filtered Back Projection (FBP) using phantomsJ Med Imaging Radiat Sci 2017 48:259-69. [Google Scholar]
[21]. Hwang HJ, Seo JB, Lee HJ, Lee SM, Kim EY, Oh SY, Low-dose chest computed tomography with sinogram-affirmed iterative reconstruction, iterative reconstruction in image space, and filtered back projection: Studies on image qualityJ Comput Assist Tomogr 2013 37:610-17. [Google Scholar]
[22]. Bodelle B, Wichmann JL, Scholtz JE, Lehnert T, Vogl TJ, Luboldt W, Iterative reconstruction leads to increased subjective and objective image quality in cranial CT in patients with strokeAm J Roentgenol 2015 205:618-22. [Google Scholar]
[23]. Hara AK, Paden RG, Silva AC, Kujak JL, Lawder HJ, Pavlicek W, Iterative Reconstruction technique for reducing body radiation dose at CT: Feasibility studyAm J Roentgenol 2009 193:764-71. [Google Scholar]
[24]. Sagara Y, Hara AK, Pavlicek W, Silva AC, Paden RG, Wu Q, Abdominal CT: Comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patientsAm J Roentgenol 2010 195:713-19. [Google Scholar]
[25]. Prakash P, Kalra MK, Kambadakone AK, Pien H, Hsieh J, Blake MA, Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction techniqueInvest Radiol 2010 45:202-10. [Google Scholar]
[26]. Leipsic J, LaBounty TM, Heilbron B, Min JK, Mancini GBJ, Lin FY, Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: The ERASIR studyAm J Roentgenol 2010 195:655-60. [Google Scholar]
[27]. Leipsic J, LaBounty TM, Heilbron B, Min JK, Mancini GBJ, Lin FY, Adaptive statistical iterative reconstruction: Assessment of image noise and image quality in coronary CT angiographyAm J Roentgenol 2010 195:649-54. [Google Scholar]
[28]. Leipsic J, Nguyen G, Brown J, Sin D, Mayo JR, A prospective evaluation of dose reduction and image quality in chest CT using adaptive statistical iterative reconstructionAm J Roentgenol 2010 195:1095-99. [Google Scholar]
[29]. Pontana F, Duhamel A, Pagniez J, Flohr T, Faivre JB, Hachulla AL, Chest computed tomography using iterative reconstruction vs filtered back projection (Part 2): Image quality of low-dose CT examinations in 80 patientsEur Radiol 2011 21:636-43. [Google Scholar]
[30]. Willemink MJ, de Jong PA, Leiner T, de Heer LM, Nievelstein RAJ, Budde RPJ, Iterative reconstruction techniques for computed tomography Part 1: Technical principlesEur Radiol 2013 23:1623-31. [Google Scholar]
[31]. Rapalino O, Kamalian S, Kamalian S, Payabvash S, Souza LCS, Zhang D, Cranial CT with adaptive statistical iterative reconstruction: Improved image quality with concomitant radiation dose reductionAm J Neuroradiol 2012 33:609-15. [Google Scholar]
[32]. Wang R, Schoepf UJ, Wu R, Reddy RP, Zhang C, Yu W, Image quality and radiation dose of low dose coronary CT angiography in obese patients: Sinogram affirmed iterative reconstruction versus filtered back projectionEur J Radiol 2012 81:3141-45. [Google Scholar]
[33]. Pickhardt PJ, Lubner MG, Kim DH, Tang J, Ruma JA, del Rio AM, Abdominal CT with Model-Based Iterative Reconstruction (MBIR): Initial results of a prospective trial comparing ultralow-dose with standard-dose imagingAm J Roentgenol 2012 199:1266-74. [Google Scholar]
[34]. Korn A, Bender B, Fenchel M, Spira D, Schabel C, Thomas C, Sinogram affirmed iterative reconstruction in head CT: Improvement of objective and subjective image quality with concomitant radiation dose reductionEur J Radiol 2013 82:1431-35. [Google Scholar]
[35]. Patino M, Fuentes JM, Hayano K, Kambadakone AR, Uyeda JW, Sahani DV, A quantitative comparison of noise reduction across five commercial (Hybrid and Model-Based) iterative reconstruction techniques: An anthropomorphic phantom studyAm J Roentgenol 2015 204:W176-83. [Google Scholar]