Dental caries is one of the most common chronic diseases of modern times. For the majority of the 20th century, Dr. G.V. Black had a significant impact on operative dentistry. His concept of “Extension for Prevention” was widely accepted. He believed that once caries developed, they would progress until the tooth was lost. This resulted in a mechanistic or surgical approach rather than a biological or therapeutic one [1]. These conventional standards led to the elimination of healthy tooth structure and significant loss of sound enamel and dentin [2].
Over the last few decades, extensive research in cariology has introduced minimally invasive treatments as an alternative therapy. There has been a shift from the philosophy of “drill and fill” to a minimally invasive approach [2].
This study aims to reduce the mechanistic approach to caries removal, especially for primary teeth and to bridge the gap in the literature. It will allow practitioners to adopt a more conservative treatment approach.
The carious dentin exhibits two layers, which have been well reported in the literature [3]. The superficial first layer is characterised by extensive decalcification, degenerated collagen fibers and is physiologically not remineralisable. In the underlying second layer, total decalcification is not present; only a slight difference is observed in collagen cross-linkage [3]. The main focus of minimally invasive restorative dentistry is to remove only the outer layer of denatured, caries-infected dentin while preserving the inner layer, which is intact, bacteria-free and remineralisable. This inner layer is also known as the caries-affected dentin layer [2].
Traditionally, caries removal was performed using hand instruments, which was laborious and time-consuming. Over time, rotary tools such as diamond burs, carbide burs and stainless-steel burs replaced manual instruments for the removal of caries. However, the drawback of these burs is that they are non selective, resulting in excessive preparation that compromises the remaining tooth structure and increases the risk of iatrogenic injury to primary teeth due to thinner dentin. Additionally, these burs cause more pain and discomfort [4].
Recently, Boston introduced new polymer burs to replace conventional ones. The Smart Bur (SS White, Lakewood, NJ, USA) is made from a polymer and features reinforced blades designed for the selective removal of carious dentin [4]. The blades are paddle-shaped and have a unique flute design, utilising low speeds (500-800 rpm). The polymer used in the bur is medical-grade Polyether-Ketone-Ketone (PEKK), which has specific hardness and wear resistance. The soft infected dentin has a Knoop Hardness Number (KHN) of 0-30, while affected dentin has a KHN of 70-90. The burs have a KHN of 50, enabling them to remove only the soft dentin without affecting the sound tooth structure. As they encounter the more highly calcified caries-affected dentin, the bur quickly dull and vibrate [5].
The traditional method of removing dental caries involves using a high-speed handpiece to access carious lesions and a low-speed handpiece to remove infected dentin. Many patients find this uncomfortable and painful, often necessitating the administration of local anaesthesia [5]. However, local anaesthesia is not required when using polymer burs [6].
The current study focuses primarily on the preservation of affected dentin, maintaining remaining dentin thickness and avoiding unnecessary pulp exposure. Additionally, due to certain disadvantages and the time required for their use, the benefits of polymer bur are often overlooked, leading to frequent neglect of their potential advantages. Therefore, the aim of the present study was to compare and evaluate the efficacy of smart burs and conventional burs in removing infected dentin while preserving affected dentin in deep carious lesions in primary teeth.
Materials and Methods
The present study was a double-blinded randomised controlled trial conducted in the Department of Paediatric and Preventive Dentistry at Swargiya Dadasaheb Kalmegh Smruti Dental College and Hospital, Nagpur, Maharashtra, India over a period of three months, from August 2023 to October 2023. Ethical approval was obtained from the institutional review board (number PG/043/2023). An information sheet was provided to the parents and informed consent was obtained. The primary outcome was the preservation of affected dentin and the removal of soft carious dentin.
Sample size calculation: The sample size was calculated using a Z value of 1.96, an error margin of 15% and a power of 80%. The formula used was: n=z2×P(1-P)÷e2
(n=no. sample, z=z statistic for level of confidence, e=allowable error, P=expected prevalence)
of 40.13=(1.96)2×0.642(1-0.642)÷(0.15)2
(p=64% according to report by Reddy S et al., in 2017 [7])
In total, 40 children were included in the study.
Inclusion criteria: Healthy children aged 6-12 years of both sexes who were willing to participate in the study were selected. Children exhibiting positive or definitely positive behaviour according to Frankel’s behaviour rating scale and having right or left maxillary and mandibular primary carious molars, were included. Asymptomatic occlusal dentine carious lesions without any clinical or radiographic symptoms of furcation involvement were also included.
Exclusion criteria: Non cooperative children with grossly decayed teeth, any clinical or radiographic signs and symptoms, or developmental defects in primary molars were excluded. Children with any underlying systemic diseases were also excluded.
Study Procedure
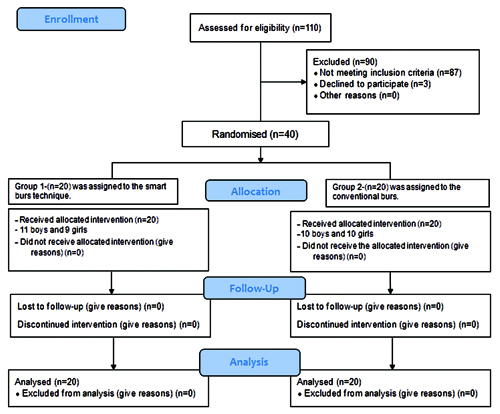
The children were randomised using a computer-generated block randomisation technique. The investigator generated and allocated the participants to specific interventions. It was a double-blinded study, where both the participants and the assessor were blinded. A total sample size of 40 children aged 6-12 years was calculated and they were equally randomised and divided into two groups of 20 samples each. Group 1 served as the control group using diamond point burs, while Group 2 served as the intervention group using polymer burs, as shown in the Consolidated Standards of Reporting Trials (CONSORT) flow chart [Table/Fig-1].
Group 1: 20 children were selected for caries excavation with smart burs (SS White RA-4) [Table/Fig-2].
Group 2: 20 children were selected for caries excavation with diamond point bur [Table/Fig-3].
Diamond point bur and SS White RA-4 polymer bur.


The clinical procedure involved a total of 40 healthy children aged 6-12 years, selected according to block randomisation. Each child assigned to a specific procedure was introduced to the process using the tell-show-do technique.
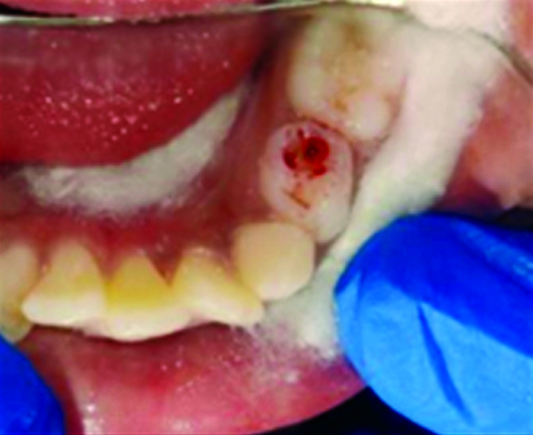
For the smart burs, the soft carious dentin was initially exposed [Table/Fig-4] by removing the unsupported enamel using a high-speed handpiece with water coolant. The exposed carious dentin was then removed with the smart bur (Group-1). Light, discrete strokes were directed from the center of the lesion outward and were used selectively over the soft caries under water coolant [Table/Fig-5]. The bur becomes abraded and smooth when it comes into contact with sound tooth structure, providing a minimally invasive approach [Table/Fig-3].

Light, discrete strokes with Smart bur under water coolant selectively over the soft caries.

Further, the removal of soft caries was verified using both visual and tactile methods. The tactile criterion was defined as the smooth passage of an explorer over the surface of the affected dentin, without any catch or a “tug back” sensation. The visual criterion was based on the removal of the infected dentin, which was further confirmed by caries indicator dye. Isolation was maintained with cotton rolls. The caries detector dye was dispensed onto an applicator tip and then applied into the cavity. After 10 seconds, the dye was rinsed-off with water and the cavity was evaluated for the presence of infected dentin [Table/Fig-6]. If the presence of infected dentin was noted, a new bur was used and the dye was reapplied to check until complete caries removal was observed. After complete removal of the infected dentin, a glass ionomer cement restoration was performed [Table/Fig-7].
Application of caries indicator dye.

Similarly, for deep carious lesions [Table/Fig-8], a diamond point (Group-2) was used, applying discrete strokes [Table/Fig-9] and caries indicator dye was utilised to confirm the complete removal of infected dentin [Table/Fig-10]. The tooth was then restored with glass ionomer cement [Table/Fig-11].

Discrete strokes with Diamond burs with water coolant were used to remove carious dentine.

Application of caries indicator dye.
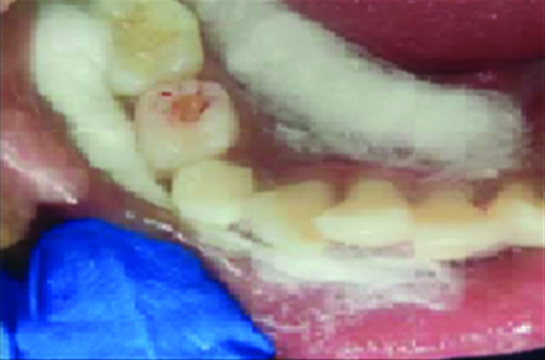

Carious tooth [Table/Fig-4], light, discrete strokes with the smart bur under water coolant selectively over the soft caries [Table/Fig-5], application of caries indicator dye [Table/Fig-6], restoration with Glass Ionomer Cement (GIC) [Table/Fig-7].
Carious tooth [Table/Fig-8], discrete strokes with diamond burs with water coolant were used to remove carious dentin [Table/Fig-9], application of caries indicator dye [Table/Fig-10], restoration with GIC [Table/Fig-11].
After the first application of caries indicator dye, scoring was done using the standard suggested by Munshi A et al., [Table/Fig-12] [8].
Scoring criteria for the assessment of the efficacy of caries removal [8].
| Score | Criteria |
|---|
| 0 | Caries completely removed |
| 1 | Caries present in the base of the cavity preparation |
| 2 | Caries present in the base and/or in one wall of the cavity preparation |
| 3 | Caries present in the base and/or two walls of the cavity preparation |
| 4 | Caries present in the base and/or more than two walls of the cavity preparation |
| 5 | Caries present in the base, walls and margins of the cavity preparation |
Statistical Analysis
Statistical analysis was performed using descriptive and inferential statistics, including the Chi-square test. The software used for the analysis was Statistical Package for the Social Sciences (SPSS) version 27.0 and GraphPad Prism version 7.0. A p-value of less than 0.05 was considered statistically significant.
Results
According to [Table/Fig-13], Group-1 consisted of 11 boys and 9 girls, while Group-2 included 10 boys and 10 girls. As shown in [Table/Fig-14], the table illustrates the efficacy of caries removal by polymer burs and conventional burs based on the scoring criteria established by Munshi A et al., It was found that 60% of cases exhibited complete caries removal after the first application of dye when using both types of burs [Table/Fig-12] [8]. In contrast, 20% of cases showed some amount of caries remaining when smart burs were used and 30% showed caries retention with diamond points at the base of the cavity preparation. Furthermore, [Table/Fig-14] indicates that 20% of cases had caries present at the base and/or in one wall of the cavity preparation when smart burs were used, compared to 10% when conventional burs were employed.
Age-wise and gender-wise distribution of subjects.
| Group | Boys (6-12 years) | Girls (6-12 years) |
|---|
| Group-1 | 11 | 9 |
| Group-2 | 10 | 10 |
Efficacy of caries removal by polymer burs and conventional burs.
| Efficacy | Smart burs | Conventional burs | χ2-value |
|---|
| Caries completely removed | 12 (60%) | 12 (60%) | 1.06p=0.58, NS |
| Caries present in the base of the cavity preparation | 4 (20%) | 6 (30%) |
| Caries present in the base and/or in one wall of the cavity preparation | 4 (20%) | 2 (10%) |
| Caries present in the base and/or two walls of the cavity preparation | 0 (0%) | 0 (0%) |
| Caries present in the base and/or more than two walls of the cavity preparation | 0 (0%) | 0 (0%) |
| Caries present in the base, walls and margins of the cavity preparation | 0 (0%) | 0 (0%) |
| Total | 20 (100%) | 20 (100%) |
Chi-square test
Comparison of the findings of similar studies with present study [4,18,19].
| S. No. | Author’s name and year (Reference no.) | Place of study | Groups studied | Population studied | Conclusion |
|---|
| 1. | Goyal A et al., 2022 [4] | India | Group-1: Smart bur IIGroup-2: Diamond point | Age 3-9 years | Non-significant p-value was obtained on comparison between groups |
| 2. | Khoury N et al., 2022 [18] | Syria | Group-1: Caries removal using Smart burs.Group-2: Caries removal with carbide conventional rotary drill | Age 6-8 years | Smart bur had significantly lower caries removal efficiency when compared to conventional carbide bur |
| 3. | Asal M et al., 2021 [19] | Mansoura | Group-1: (Polymer bur group)Group-3: (Conventional group) | Age 4-8 years | The mean total viable bacterial count after caries removal was significantly higher in polymer bur. While, there was no significant difference |
| 4. | Present study | India | Group-1: Smart bursGroup-2: Diamond point bur | Age 6-12 years | Statistically insignificant results were obtained on comparison between the group |
Discussion
Minimally Invasive Treatment (MIT) is an approach that utilises conservative techniques to manage large carious lesions while preserving maximum tooth structure [9]. The aim of the present study was to preserve affected dentin and maintain the vitality of the teeth. According to Rajnekar R et al., the affected dentin exhibits a loss of minerals but retains an intact collagen framework. This layer has the ability to remineralise, allowing the stressed pulp to heal and repair, potentially eliminating the need for invasive procedures such as pulp therapy [10].
The authors selected an age group of 6-12 years because, according to Schindova M et al., children in this age range tend to exhibit little or no dental fear [11]. Furthermore, Jindal L et al., reported that the prevalence of caries in six-year-old children is 63.6% and in 12-year-old children, it is 56.3%. Therefore, the current study focused on the 6-12 year age group with a sample size of 40 children [12].
The Tell-Show-Do behaviour management technique was used to introduce the children to the procedure, as it is considered to be highly effective. According to Lekhwani P et al., this technique is the most widely accepted and has been modified for better results [13]. An in-vivo randomised controlled trial design was followed in this study. Goyal A et al., conducted a similar in-vivo randomised controlled trial comparing smart burs, ceramic burs and diamond points [4]. Meanwhile, Shakya V et al., conducted an in-vitro study and concluded that the Smartprep bur exhibits a more conservative approach to selectively removing dentin caries compared to conventional burs [2].
During the clinical procedure, dye was applied to all the teeth to confirm the removal of soft caries, in addition to other clinical evaluation parameters. While polymer burs are selective in caries removal and do not require dye application-since the bur abrades upon contact with affected dentin, indicating safe cutting. But during the course of the study, it was appreciated that the samples showed extensive variation in extent of caries thus to standardise, a single application of the caries detector dye was considered. Nevertheless, Carounanidy U and Ranjani R concluded that histopathologic examination of sections is the ideal method for observing carious alterations in dentin [14].
In the present study, score 1 was found in four subjects of the smart bur group (carious dentin on the floor) and score 2 was also found in four subjects (caries present in the base and/or in one wall of the cavity preparation), indicating that the polymer bur tends to leave behind infected dentin. Similarly, Wahba W et al., concluded that when using Smart Bur II, they observed complete caries removal in only 36.6% of cases, while incomplete removal occurred in 63.4% of cases [15]. Prabhakar A and Kiran NK found that the polymer bur was self-limiting, resulting in decreased cutting ability when the bur came into contact with healthy dentin [16]. According to Soni H et al., the greatest efficacy of caries removal was observed with a diamond abrasive round point compared to the polymer bur [17]. In 2012, Shakya V et al., conducted an in-vitro study comparing smart prep, diamond and carbide burs. The results showed that the difference in the grading of remaining carious dentin between smart prep and conventional burs (diamond and carbide) after total excavation of samples was statistically insignificant [2].
In the current study, a non significant result was observed and an approximately equal number of cases showed complete removal of caries in both groups. Goyal A et al., also reported similar results when comparing the two, as shown in [Table/Fig-15] [4,18,19].
The polymer burs were found to be more selective and conservative in cutting due to their special properties and blade design, whereas the diamond points were inefficient in differentiating between carious and healthy dentin [4]. Additionally, Divya G et al., found that when comparing these burs to traditional burs, polymer burs were more conservative and caused the least amount of dentinal tubule damage [20]. Shakya V et al., concluded that the Smartprep bur is more conservative than carbide and diamond points, but noted that these burs have a high probability of over-preparation [2]. In contrast, Nagham K et al., concluded that the smart bur was less efficient in caries removal compared to conventional carbide burs [21].
Strassler H stated that the polymer bur can be utilised to selectively remove carious tooth structure without causing unnecessary damage to healthy tooth structure [22]. Both Shakya V et al., and Goyal A et al., reported that polymer burs require more time for caries removal than conventional burs. The longer duration associated with the smart bur can be attributed to its rapid abrasion and loss of cutting efficiency upon contact with sound dentin, necessitating the frequent replacement of the bur [2,4]. Similarly, in the current study, it was observed that the burs became abraded quickly, making it necessary to replace them repeatedly until complete caries removal was achieved. This makes them technique-sensitive, expensive and more time-consuming than conventional burs.
According to Somani R et al., polymer burs can be considered equally successful as traditional burs in terms of reducing microbial presence following caries removal. However, they require more time to use compared to conventional burs [23]. Inamdar M et al., compared BRIX3000, Carie Care and Smart bur, concluding that all three effectively reduced bacterial counts, but in terms of working time, BRIX3000 is the best choice, followed by Carie Care and Smart bur, which abrades frequently [24].
The selective, judicious and smart use of these polymer burs will facilitate a more precise practice of minimally invasive dentistry, reduce a child’s anxiety during initial visits and make subsequent appointments easier and more comfortable for the child.
Limitation(s)
The present study lacks an assessment of microbial counts, a brief analysis of the longevity of restorations and an evaluation of the occurrence of secondary caries. Additionally, further research should be conducted to examine the remaining dentin thickness. A larger sample size and more comprehensive analysis are necessary to achieve more reliable results. Furthermore, since each carious tooth in the included sample had a different extent of caries and management approach, standardisation is a matter of concern.
Conclusion(s)
It can be concluded that smart burs are equally effective in removing soft caries compared to conventional methods. Although the results were statistically insignificant, polymer burs can be considered a viable alternative to conventional caries removal techniques. The polymer burs were found to be more convenient, as their abrasion upon contact with sound tooth structure aids in the easy identification of affected carious dentine. Thus, the major goals of conservative cavity preparation were achieved.
Chi-square test