Introduction
Mechanical Low Back Pain (MLBP) is a prevalent condition that significantly impacts individuals’ quality of life and healthcare systems worldwide. The management of MLBP has explored various manual therapy techniques, including Maitland mobilisation; however, the immediate effects and comparative efficacy of these techniques remain subjects of ongoing investigation.
Aim
To evaluate the immediate effects of Maitland mobilisation compared to other manual therapy techniques on flexion and extension Range of Motion (ROM) in patients with MLBP.
Materials and Methods
The present systematic review involved a comprehensive search of electronic databases, including PubMed, Cochrane Library, and Google Scholar, from January 2017 to March 2024. The search utilised the keywords “Randomised Controlled Trials (RCTs)”, “Maitland mobilisation”, and “mechanical low back pain”. Studies comparing the immediate effects of Maitland mobilisation with other manual therapy techniques on flexion and extension ROM in patients with MLBP were included. Data extraction and quality assessment were performed using established protocols.
Results
Nine studies met the inclusion criteria and were included in the review. The findings revealed that Maitland mobilisation demonstrated significant immediate effects on both flexion and extension ROM in patients with MLBP. Improvements were particularly noted in lumbar flexion following Maitland mobilisation, while lumbar extension showed greater enhancement after specific techniques such as Posteroanterior (PA) mobilisation. Additionally, combination therapies, such as core stability exercises coupled with Maitland manual therapy, showed promising results in reducing disability associated with MLBP.
Conclusion
This review investigated the immediate effects of Maitland mobilisation on ROM in MLBP. While some studies indicated improvements in ROM, the evidence for its effectiveness compared to other interventions and its long-term impact on pain and function remains unclear. Future well-designed studies are needed to definitively assess the role of Maitland mobilisation in the management of MLBP.
Introduction
The MLBP stands as one of the most prevalent musculoskeletal disorders worldwide, affecting individuals across various age groups and occupations [1]. The burden of MLBP is not limited to physical discomfort; it also encompasses psychological distress, economic costs, and reduced quality of life [2]. Given its multifaceted impact, effective management strategies for MLBP are of paramount importance. In recent years, manual therapy techniques have gained increasing attention as viable interventions for MLBP management. Among these techniques, Maitland mobilisation has emerged as a prominent approach, characterised by its emphasis on assessment-driven treatment tailored to individual patient presentations. Developed by Geoffrey Maitland, this method employs skilled passive movements applied at varying speeds, amplitudes, and directions to specific joints with the aim of restoring optimal function [3].
Epidemiological data indicate that low back pain is a leading cause of disability worldwide, with a lifetime prevalence of up to 84% [4]. In the United States, approximately 23% of adults suffer from Chronic Low Back Pain (CLBP), with many experiencing recurrent episodes [5]. The economic burden of CLBP is significant, with direct healthcare costs and indirect costs related to lost productivity and disability reaching substantial levels. These statistics highlight the urgent need for effective therapeutic interventions like Maitland mobilisation to mitigate the pervasive impact of MLBP on individuals and society [6].
Maitland mobilisation is thought to be effective in managing MLBP due to its complex effects on proprioception, joint mobility, tissue repair, and pain modulation [7]. The approach aims to address the underlying dysfunctions of MLBP by combining neurophysiological and biomechanical principles, thereby reducing symptoms and enhancing functional outcomes [8]. Although Maitland mobilisation has a theoretical foundation and is frequently used in clinical settings, the actual data demonstrating its effectiveness in managing MLBP remains inconsistent and open to discussion. While some studies show favourable results, others are unable to demonstrate a discernible improvement over alternative interventions or control circumstances [9].
To shed light on this issue, the goal of this review was to thoroughly assess the available data regarding Maitland mobilisation’s effectiveness in addressing MLBP. This review aims to provide insight into the immediate, intermediate, and long-term impacts of Maitland mobilisation on important outcomes such as pain severity, functional impairment, and ROM. An extensive exploration of various electronic databases, including PubMed, EMBASE, Web of Science, and Scopus, was conducted to identify pertinent research. A thorough evaluation was performed on studies that met predetermined inclusion criteria, with special emphasis on methodological quality and risk of bias [10].
MLBP is a leading cause of disability worldwide, resulting in significant healthcare costs and a substantial impact on individual wellbeing. Through this review, non invasive interventions are explored that have the potential to improve patient outcomes for this prevalent condition. This ongoing research investigates the effectiveness of Maitland mobilisation for MLBP, focusing on its impact on pain and function. This systematic review will serve as a companion piece to my investigation, aiming to provide a comprehensive understanding of the broader effects of Maitland mobilisation on MLBP.
Through a rigorous analysis of recent research, particularly focusing on high-quality RCTs, this review will critically evaluate the immediate effects of Maitland mobilisation on flexion and extension ROM in individuals with MLBP. This particular emphasis on ROM is consistent with current research trends that highlight the role of joint mobility in the treatment of MLBP. In addition to summarising the available data on the effectiveness of Maitland mobilisation in improving ROM, this review will identify areas where additional research is required by evaluating the methodological strengths and weaknesses of the included studies. Determining these gaps in knowledge is essential for charting future paths in this field of study.
Furthermore, the review will explore studies investigating the combined effects of Maitland mobilisation with other interventions, potentially informing future research on optimising treatment strategies for MLBP, including those focused on pain and function. Ultimately, this review seeks to provide evidence-based guidance for clinicians managing MLBP, empowering them to make informed treatment decisions based on the latest research.
This review aims to assess the immediate impact of Maitland mobilisation compared to other manual therapy techniques on flexion and extension ROM in individuals with MLBP. By synthesising evidence from RCTs, the review seeks to determine the effectiveness of these interventions in enhancing ROM. This analysis intends to provide valuable insights for clinicians and researchers in the field of manual therapy.
Materials and Methods
PICO Framework
Population: This review focuses on patients diagnosed with MLBP.
Intervention: The intervention of interest is Maitland mobilisation.
Comparison: Comparisons are made with other manual therapy techniques.
Outcome: The primary outcomes are the immediate effects on movements (flexion/extension/range of motion).
A systematic search was conducted across several electronic databases-PubMed, Cochrane Library, and Google Scholar-to locate studies published between January 2017 and March 2024. The primary keywords used were “Maitland mobilisation,” “mechanical low back pain,” and “RCTs.” Boolean operators (AND, OR) were employed, and the search was strategically expanded to capture a comprehensive range of studies without compromising relevance.
The study selection process is depicted in [Table/Fig-1]. The initial database search identified 71 studies. Titles and abstracts were screened for alignment with our review’s objectives, and duplicates were promptly removed. This screening phase ensured that studies not related to the objectives were excluded early. In the subsequent eligibility stage, full-text assessments were conducted to rigourously evaluate the remaining studies against our predefined criteria, resulting in the exclusion of those with insufficient data. Ultimately, only studies that fully met the inclusion and exclusion criteria were incorporated into the final review. An additional literature search was performed by assessing the references of the articles included in the systematic review.
Flow chart presenting the selection process of included studies.
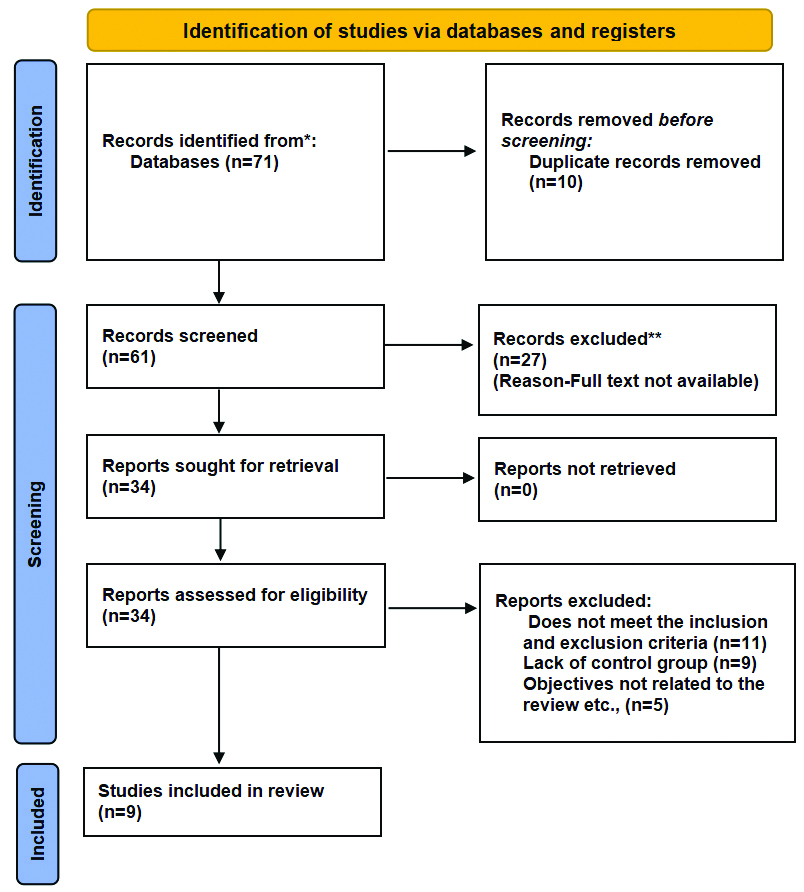
Inclusion criteria: Studies evaluating interventions for MLBP, studies that specifically investigated the use of Maitland mobilisation, Randomised Controlled Trials (RCTs), studies published between January 2017 and March 2024 were included in the review.
Exclusion criteria: Studies not related to MLBP, non randomised studies, studies with insufficient data were excluded from the study.
A total of nine studies met the inclusion criteria and were included for further analysis.
Data extraction: To ensure consistent and accurate data collection, the researcher meticulously extracted information from each of the nine included studies using a standardised data extraction form. This form encompassed sections for study characteristics (e.g., authors, publication year, study design), intervention details (specific Maitland mobilisation techniques used, dosage, and comparator intervention details, if applicable), outcome measures (specific methods employed to assess lumbar spine flexion and extension range of motion), and results (key findings regarding the effects of the interventions on participants’ range of motion). By systematically extracting this information using the standardised form, the researcher ensured a comprehensive and reliable data collection process for the review.
Quality assessment: To rigourously evaluate the methodological quality and potential bias of the included studies, two established tools were employed: the Cochrane Collaboration’s Risk of Bias Tool for randomised trials and the Physiotherapy Evidence Database (PEDro) scale. The Cochrane tool assesses seven critical domains that could lead to bias, including random sequence generation, allocation concealment, blinding of participants and personnel (where applicable), blinding of outcome assessment, handling of incomplete outcome data, selective reporting, and other potential sources of bias. Each domain was rated as having a high, low, or unclear risk of bias based on the provided study details. In addition to the Cochrane tool, the PEDro scale was used to further ensure the methodological rigour of the studies. The PEDro scale, specifically designed for evaluating physiotherapy trials, includes 11 criteria such as eligibility criteria, random allocation, concealed allocation, baseline comparability, blinding of subjects, therapists, and assessors, adequate follow-up, intention-to-treat analysis, statistical comparisons between groups, and the reporting of point estimates and variability. Each criterion is scored as either met (1) or not met (0), with a maximum score of 10 (since the eligibility criterion is not included in the total score). By using these two complementary tools, a comprehensive assessment of the studies’ methodological quality and risk of bias was achieved. This approach ensures a thorough and reliable evaluation, providing a robust foundation for interpreting the findings and drawing meaningful conclusions from the included research [11,12].
Data synthesis: A narrative synthesis approach was used to summarise the findings of the included studies. This approach involved a comprehensive description and analysis of the data extracted from each study. Data on study characteristics (e.g., authors, publication year, study design), intervention details (specific techniques, dosage), outcome measures (methods used to assess range of motion), and risk of bias were synthesised descriptively. Additionally, quantitative data such as effect sizes and confidence intervals (if reported in the studies) were presented to provide further context and strengthen the narrative synthesis.
Results
The current review focused on the immediate effects of Maitland mobilisation on flexion and extension ROM in patients with MLBP. Nine studies were included, investigating the impact of various interventions on ROM and related outcomes in these patients. Briefly, the studies employed various methodologies, including RCTs and cohort studies. Sample sizes ranged from 12 to 70 participants.
Interventions included Maitland mobilisation alone or combined with other therapies (e.g., core stability exercises) and were compared to exercise programs, sham manipulations, or other manual therapy techniques. Outcome measures varied across studies but commonly assessed pain intensity, functional disability, lumbar ROM, and other parameters [Table/Fig-2,3] [13-21].
Study characteristics [19-21].
| Study | Design | Subjects | Intervention | Duration | Outcome measure | Summary |
|---|
| Ejaz R et al., 2024 [16] | Randomised Controlled Trial (RCT) | N=26 | Group A: Shockwave therapy Group B: Maitland lumbar mobilisations | 30 days, eight sessions | Numeric pain rating scale, Oswestry LBP disability index, lumbar flexion and extension ROM | Compared shockwave therapy and Maitland lumbar mobilisations in MLBP patients. The study found significant improvements in pain levels, disability scores, and ROM values in both groups, with greater improvements observed in the Maitland mobilisation group. |
| Ibrahim A et al., 2023 [17] | Randomised Controlled Trial (RCT) | N=54 | Group A: Selected exercise program and Maitland mobilisationGroup B: Selected exercise program only | Four weeks | Lumbar repositioning error, pain intensity, functional disability | Investigated the efficacy of a selected exercise program combined with Maitland mobilisation versus exercise program alone. The study found that the combined intervention resulted in reduced lumbar repositioning error, pain intensity, and functional disability compared to exercise alone. |
| Ahmed F et al., 2020 [20] | Randomised Controlled Trial (RCT) | N=70 | Group A: Maitland manual therapy+core stability exercisesGroup B: Conventional physical therapy | Five weeks | Roland Morris Disability Index | Investigated the effectiveness of Maitland manual therapy combined with core stability exercises versus conventional physical therapy alone. The Maitland manual therapy group showed greater improvements in functional disability compared to conventional therapy. |
| Zaidi F and Ahmed I 2020 [21] | Randomised Controlled Trial (RCT) | N=60 | Group A: Muscle energy technique+Lumbopelvic stability exercisesGroup B: Maitland mobilisations+Lumbopelvic stability exercises | Four weeks | Visual Analogue Scale (VAS), Modified Oswestry Disability Index | Compared muscle energy technique with Maitland mobilisations combined with lumbopelvic stability exercises. Both groups exhibited significant improvements in pain intensity and disability, with no significant difference between the two interventions. |
| Chopade P, 2018 [18] | Randomised Controlled Trial (RCT) | N=60 | Group A: Conventional therapy and Maitland mobilisationGroup B: Conventional and McKenzie therapy Group C: Conventional therapy | Three weeks, three visits per week | VAS, Lumbar Range of Motion (ROM) with Inclinometer, Oswestry Disability Index | Compared conventional therapy combined with Maitland mobilisation, conventional therapy combined with McKenzie therapy, and conventional therapy alone. All groups showed improvements in pain intensity, lumbar ROM, and functional disability, with no significant differences between the groups. |
| Khan S et al., 2018 [13] | Randomised Controlled Trial (RCT) | N=60 | Group A: SNAGGroup B: Maitland’s mobilisation | Four weeks, three sessions per week, one session per day | VAS, ODI, Lumbar Range of Motion (ROM) | Compared SNAG technique with Maitland’s mobilisation in MLBP patients. Both groups showed significant improvements in pain intensity, functional disability, and lumbar ROM after 4 weeks of treatment. |
| Javaherian M et al., 2017 [14] | Randomised Controlled Trial (RCT) | N=18 | Group A: Posteroanterior (PA) mobilisationGroup B: SNAG Group C: Sham SNAG | One-time study | Lumbar flexion and extension ROM | Compared Posteroanterior (PA) mobilisation, SNAG technique, and sham SNAG in MLBP patients. The study found no significant differences in lumbar flexion and extension ROM between the groups. |
| Tavares FA et al., 2017 [15] | Randomised Controlled Trial (RCT) | N=60 | Group A: Joint Mobilisation Group B: Sham Mobilisation Group C: Control | Ten sessions | Pain numeric scale, Oswestry Disability Index, Catastrophic Thoughts Scale | Compared joint mobilisation, sham mobilisation, and control in MLBP patients. Joint mobilisation led to significant reductions in pain intensity, disability, and catastrophic thoughts compared to sham mobilisation and control. |
| De Mèlo LC et al., 2017 [19] | Randomised Controlled Trial (RCT) | N=12 | Intervention Group: Maitland method+Exercisescontrol group: Exercises only | Six weeks | Finger-ground index, Roland Morris Questionnaire, Visual Analogue Scale | Investigated the efficacy of Maitland method combined with exercises versus exercises alone in MLBP patients. Both groups showed improvements in finger-ground index, functional disability, and pain intensity, with no significant difference between the groups. |
| Study | Intervention | Results |
|---|
| Ejaz R et al., 2024 [16] | Shockwave therapy vs. Maitland lumbar mobilisations | Significant improvements in pain levels, disability scores, and ROM values in both groups, with greater improvements observed in the Maitland mobilisation group (p-value <0.005). |
| Ibrahim A et al., 2023 [17] | Maitland mobilisation vs. Exercise program only | Maitland mobilisation resulted in significant improvement in lumbar proprioception, pain intensity, and functional disability compared to exercise program alone. |
| Ahmed F et al., 2020 [20] | Maitland manual therapy+Core stability exercises vs. Conventional physical therapy | Maitland manual therapy+Core stability exercises significantly improved MLBP-related disability compared to conventional therapy. |
| Zaidi F and Ahmed I 2020 [21] | Muscle energy technique+Lumbopelvic stability exercises vs. Maitland mobilisations+Lumbopelvic stability exercises | Both MET and Maitland mobilisations effective in treating chronic sacroiliac joint dysfunction, with no significant difference between them. |
| Chopade P 2018 [18] | Maitland mobilisation vs. McKenzie therapy | McKenzie therapy with conventional therapy resulted in greater pain alleviation and ROM improvement compared to Maitland’s mobilisation. |
| Khan S et al., 2018 [13] | SNAG vs. Maitland’s mobilisation | Both SNAG and Maitland’s improved symptoms of MLBP, with better improvement in SNv group. |
| Javaherian M et al., 2017 [14] | PA Mobilisation vs. SNAG vs. Sham SNAG | Significant changes in ROMs in SNAG and PA mobilisation groups. |
| Tavares FA et al., 2017 [15] | Joint mobilisation vs. Sham mobilisation vs. Control | Significant reductions in pain intensity have been observed in the group receiving mobilisation therapy. |
| De Mèlo LC et al., 2017 [19] | Maitland method+Exercises vs. Exercises only | Maitland method+Exercises effective in reducing pain and improving functionality in physical therapy students with MLBP. |
The risk of bias assessment was conducted using the PEDro chart, and is described in [Table/Fig-4]. This review investigated the immediate effects of Maitland mobilisation on improving flexion and extension ROM in patients with MLBP. The findings presented mixed results regarding its effectiveness as a standalone intervention. Several studies (e.g., Ejaz R et al., 2024; Ibrahim A et al., 2023) demonstrated significant improvements in pain, disability, and ROM following Maitland mobilisation compared to controls [16,17]. These findings support the potential benefits of Maitland mobilisation for managing MLBP. This aligns with the theoretical principles of manual therapy, which suggest that improved joint mobility can reduce pain and muscle guarding, ultimately leading to better functional movement. However, other studies did not observe a significant difference in ROM or pain reduction between Maitland mobilisation and other interventions [17,18]. This inconsistency highlights the need for further exploration into specific protocols and techniques within Maitland mobilisation that may be most effective for improving ROM in MLBP patients.
PEDro chart for all the studies.
| Study | 1* | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|
| Ejaz R et al., 2024 [16] | 1* | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 8 |
| Ibrahim A et al., 2023 [17] | 1* | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Ahmed F et al., 2020 [20] | 1* | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 8 |
| Zaidi F and Ahmed I, 2020 [21] | 1* | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 6 |
| Chopade P, 2018 [18] | 1* | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Khan S et al., 2018 [13] | 1* | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Javaherian M et al., 2017 [14] | 1* | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Tavares FA et al., 2017 [15] | 1* | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| De Mèlo LC et al., 2017 [19] | 1* | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 9 |
(0-Criteria not met; 1-Criteria met; *Eligibility criteria were not considered in the total score)
Interestingly, several studies compared Maitland mobilisation to other techniques. Khan S et al., reported superior results for the Sustained Natural Apophyseal Glides (SNAG) technique compared to Maitland mobilisation in terms of ROM and pain reduction [13]. Similarly, Javaherian M et al., observed comparable improvements in ROM with both SNAG and PA mobilisation, but SNAG outperformed the sham treatment [14]. These findings suggest that SNAG might be a more effective approach for managing pain and improving ROM in some cases. Further research is needed to explore the mechanisms underlying these observed differences and to identify the most suitable technique for different patient presentations [13,14].
Tavares FA et al., observed a significant pain reduction within the sham mobilisation group, highlighting the potential for a placebo effect associated with manual therapy techniques for MLBP management. Future studies should consider robust blinding protocols to minimise this influence [15]. While the core focus was on ROM improvements, some studies explored broader outcomes. Ejaz R et al., compared Maitland mobilisation to shockwave therapy, finding both interventions effective, but Maitland mobilisation was superior in improving ROM [16]. This suggests potential benefits beyond pain reduction for Maitland mobilisation. protocols [19-21]. It is important to note that some studies had limitations. The studies by De Mèlo LC et al., Ahmed F et al., and Zaidi F and Ahmed I did not specify the exact techniques used within Maitland mobilisation, making it difficult to draw definitive conclusions about specific protocols [19-21].
Discussion
The evidence regarding Maitland mobilisation for improving ROM in MLBP was mixed. While some studies show promise, particularly when combined with other interventions, further research is necessary to explore optimal protocols and techniques, understand the role of placebo effects, and determine long-term benefits. Additionally, investigating the mechanisms underlying the potential effectiveness of SNAG compared to Maitland mobilisation warrants further examination.
To overcome these methodological obstacles and strengthen the body of evidence, future research should prioritise well-designed RCTs with larger sample sizes and standardised Maitland mobilisation protocols. Blinding protocols and extended follow-up periods are crucial to minimise bias and understand long-term effects. Incorporating a broader range of outcome measures, including patient-reported outcomes, alongside comparisons to conventional treatments, will provide a more comprehensive understanding of Maitland mobilisation’s effectiveness and cost-effectiveness for managing MLBP across diverse patient populations.
Limitation(s)
This review was limited by the heterogeneity of the included studies, particularly regarding the specific techniques and protocols used within Maitland mobilisation. Additionally, the focus on immediate effects limits the understanding of long-term benefits.
Conclusion(s)
The findings summarised here highlight the difficulty in conclusively establishing the effectiveness of Maitland mobilisation in treating MLBP. Although Maitland mobilisation showed some promise in terms of reducing pain, increasing ROM, and improving functional outcomes, the overall picture was complex, with different interventions and patient populations producing varying results. Mixed outcomes were observed in studies comparing alternative interventions to Maitland mobilisation. While some research claims that Maitland mobilisation significantly reduces pain intensity, ROM, and functional disability compared to exercise regimens alone, others suggest that when combined with conventional therapy, alternative therapies such as McKenzie therapy may reduce pain even more and improve ROM. Furthermore, studies comparing Maitland mobilisation to other modalities, like Feng Spinal Mobilisation (FSM), indicate that FSM may be more effective than Maitland mobilisation in lowering pain scores and enhancing functional outcomes. This underscores the importance of investigating different manual therapy modalities when managing MLBP. The body of evidence also emphasises the necessity of considering each patient’s unique characteristics and preferences when choosing a course of treatment. While Maitland mobilisation may be beneficial for some MLBP patients, others may respond better to alternative approaches.
(0-Criteria not met; 1-Criteria met; *Eligibility criteria were not considered in the total score)
[1]. Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, The global burden of low back pain: Estimates from the global burden of disease 2010 studyAnn Rheum Dis 2014 73(6):968-74. [Google Scholar]
[2]. Froud R, Patterson S, Eldridge S, Seale C, Pincus T, Rajendran D, A systematic review and meta-synthesis of the impact of low back pain on people’s livesBMC Musculoskeletal Disorders 2014 15(1):50 [Google Scholar]
[3]. Grieve GP, Grieve’s modern manual therapy: The vertebral column 2004 Elsevier Health Sciences [Google Scholar]
[4]. Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, A systematic review of the global prevalence of low back painArthritis Rheum 2012 64(6):2028-37. [Google Scholar]
[5]. Dagenais S, Caro J, Haldeman S, A systematic review of low back pain cost of illness studies in the United States and internationallySpine J 2008 8(1):08-20. [Google Scholar]
[6]. Luo X, Pietrobon R, Sun SX, Liu GG, Hey L, Estimates and patterns of direct health care expenditures among individuals with back pain in the United StatesSpine 2004 29(1):79-86. [Google Scholar]
[7]. Flynn T, Fritz J, Whitman J, A clinical prediction rule for classifying patients with low back pain who demonstrate short-term improvement with spinal manipulationSpine 2002 27(24):2835-43. [Google Scholar]
[8]. Halliday MH, Pappas E, Hancock MJ, Clare HA, Manual therapy and exercise for mechanical neck pain: A systematic review and meta-analysisJ Back and Musculoskeletal Rehabilitation 2019 32(3):351-61. [Google Scholar]
[9]. Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alén M, Videman T, Orthopaedic manual therapy, McKenzie method or advice only for low back pain in working adults: A randomized controlled trial with one year follow-upJ Rehab Med 2018 50(6):541-49. [Google Scholar]
[10]. Hidalgo B, Hall T, Bossert J, The effectiveness of manual therapy for the management of musculoskeletal disorders of the upper and lower extremities: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) CollaborationManual Therapy 2020 46:53-64. [Google Scholar]
[11]. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, The Cochrane Collaboration’s tool for assessing risk of bias in randomized trialsBMJ 2011 343:d5928 [Google Scholar]
[12]. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M, Reliability of the PEDro scale for rating quality of randomized controlled trialsPhysical Therapy 2003 83(8):713-21. [Google Scholar]
[13]. Khan S, Al Torairi N, Shamsi S, Comparative study of SNAGS and Maitland’s mobilisation in chronic low back painEuro J Physical Education and Sport Sci 2018 4(2):71-84. [Google Scholar]
[14]. Javaherian M, Tajali SB, Moghaddam BA, Keshtkar AA, Azizi M, Immediate effects of Maitland mobilisation and Mulligan techniques on flexion and extension range of motion in patients with chronic nonspecific low back pain: A randomized pilot studyJ Modern Rehabilitation 2017 11(2):127-32. [Google Scholar]
[15]. Tavares FA, Chaves TC, Silva ED, Guerreiro GD, Gonçalves JF, Albuquerque AA, Immediate effects of joint mobilisation compared to Sham and control intervention for pain intensity and disability in chronic low back pain patients: Randomized controlled clinical trialRevista Dor 2017 18(1):02-07. [Google Scholar]
[16]. Ejaz R, Rafique S, Hamid K, Raza Q, Haider S, Comparative effects of shockwave therapy and Maitland lumbar mobilisation on pain, disability, and range of motion in patients with mechanical low back pain: A pilot studyJ Musculo Sur Res 2024 8(2):153-59. [Google Scholar]
[17]. Ibrahim A, Elkeblawy MM, Howeidy MS, Elkeblawy MM, Grase MO, Aneis YM, Effect of Maitland mobilisation on lumbar proprioception, pain, and disability in patients with Mechanical Low Back Pain (MLBP)Physiotherapy Quarterly 2023 31(4):87-92.Available from: https://doi.org/10.5114/pq.2023.125167 [Google Scholar]
[18]. Chopade P, Comparison of Maitland’s mobilisation and Mckenzie therapy in patients with nonspecific low back painInt J Biol Med Res 2018 9(2):6270-77. [Google Scholar]
[19]. De Mèlo LC, de Mendonça HCS, de Amorim Cabral KD, Rodrigues FTM, do Nascimento LSG, Guerino MR, Maitland in chronic lumbar pain of young adults improves pain and functionalityManual Therapy, Posturology & Rehabilitation Journal 2017 :01-07. [Google Scholar]
[20]. Ahmed F, Rahman MU, Ullah K, Bhutta AH, Combination of core stability exercises and maitland manual therapy is better alternative in the management of chronic low back painJ Riphah College of Rehab Sci 2020 8(01):S24-S28. [Google Scholar]
[21]. Zaidi F, Ahmed I, Effectiveness of muscle energy technique as compared to Maitland mobilisation for the treatment of chronic sacroiliac joint dysfunctionAge 2020 36(7.006):3738 [Google Scholar]