The increase in the lifespan of individuals and higher success rates in endodontics have widened the scope of this field [1]. Root Canal Treatment (RCT) is a meticulous, conservative approach that removes infected pulpal tissue, addresses pulpal or periradicular issues and protects the tooth from future infections, thereby ensuring its long-term health [2]. Advances in endodontics have made RCT the preferred alternative to tooth extraction, with success rates exceeding 90% [3,4].
Post-endodontic pain, experienced by 25% to 40% of patients, refers to the discomfort felt after RCT, irrespective of pulp and periradicular conditions [5-7]. According to Pak JG and White SN (2011), 40% of patients report discomfort within the first 24 hours, which decreases to 11% after seven days [8].
Post-endodontic pain is influenced by host factors, such as immunity and preoperative pain history, as well as operator factors, including mechanical, chemical, or bacterial damage during preparation [9]. A significant cause of this pain is the unintended extrusion of dentin chips, microorganisms, tissue remnants, or necrotic debris into the periapical region [10], leading to inflammation, increased vascular permeability, oedema and nerve compression [11]. The amount of debris extruded varies with instrumentation techniques and no current technology completely prevents it [11].
Rotary systems differ in debris extrusion due to variations in cross-sectional geometry, flute depth, cutting blade design, kinematics, taper, file sequence, tip diameter and cutting efficiency. Both rotary and reciprocating NiTi instruments are effective in reducing endotoxins and bacterial by-products in infected root canals. NiTi instruments, regardless of their motion, improve canal centering and reduce cycle fatigue. However, different NiTi systems may elicit varied inflammatory responses in periradicular tissues due to differing amounts of extruded irritants [12].
Recent advancements in endodontic instruments include new thermomechanically treated NiTi alloys and variable kinematics. The XP Endo Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland) is a single-file system designed to minimise stress on the dentinal walls. It utilises Max Wire (Martensite-Austenite Electropolishing-Flex, FKG) alloys that transition from martensite at room temperature to austenite at body temperature. This system achieves a minimum canal preparation size of 30/0.04 and operates at 800 rpm with a torque of 1 Ncm [13].
Another continuous rotation system, Mtwo (VDW; Munich, Germany), features a non cutting tip and a cross-section resembling an italic “S”, with two cutting blades. It operates at speeds ranging from 250 to 350 rpm with a torque of 0.981 Ncm [14].
Reciprocating systems, such as WOG by Dentsply Sirona (Ballaigues, Switzerland), employ a single-file design with an off-centered parallelogram cross-section, a reverse helix and semi-active modified guiding tips. Its Gold Wire heat treatment provides flexibility and fatigue resistance, operating at 350 rpm with alternating 150° counter-clockwise and 30° clockwise motions [15]. Similarly, E-Flex Rec (Orikam India) features a non cutting tip, a double “S” cross-section and heat-treated control memory NiTi wire, operating at 300 rpm with similar reciprocating motions.
Clinical studies on the effects of continuous versus reciprocating kinematics on postoperative pain have shown disparities in outcomes, likely due to differences in equipment and mechanical properties [1,10-12,14-16]. Consequently, further clinical research is necessary to fully understand the impact of endodontic tools on postoperative discomfort. Therefore, the aim of this randomised clinical study was to compare WOG and E-Flex Rec (reciprocating systems) with Mtwo and XP Endo Shaper (rotary systems) regarding the level of discomfort experienced following endodontic therapy for both single- and multi-rooted teeth.
Materials and Methods
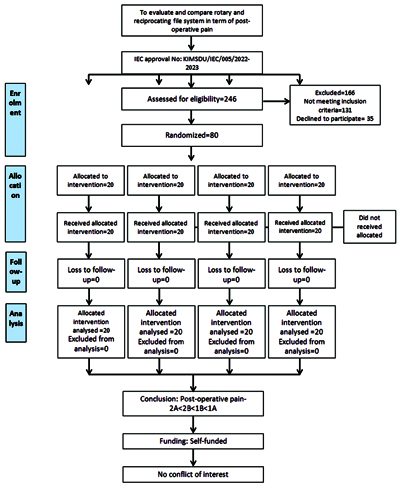
This was a prospective, parallel-group, single-centre, double-blinded, equivalence, randomised clinical trial conducted from October 2023 to March 2024 in the Department of Conservative Dentistry and Endodontics at School of Dental Sciences, Krishna Vishwa Vidyapeeth (Deemed To be University), Karad, Maharashtra, India. The study was conducted after obtaining ethical clearance from the Institutional Ethical Committee (IEC approval No: with protocol number 005/2022-2023 KIMSDU/IEC/08/2022).
Inclusion and Exclusion criteria: A total of 246 consecutive patients were screened based on the following selection criteria: Participants aged between 19 to 70 years with symptomatic irreversible pulpitis without apical periodontitis, involving either single-rooted or multi-rooted teeth, were included in the study. Individuals were excluded if they presented with a periapical lesion, abscess, or cellulitis; had complicating systemic diseases; had teeth with open apices or associated with a sinus opening; or had poor oral hygiene.
Sample size calculation: A power analysis was performed using G*Power version 3.0.1 (Franz Faul, Universität Kiel, Germany). The total minimum calculated sample size was 76, rounded to 80 samples (20 samples per group; total of 4 groups), which would yield 80% power to detect significant differences, with an effect size of 0.4 and a significance level of 0.05 [17]. Thus, a total of 80 patients were recruited for the study and randomised into 4 groups with the aid of a computer-generated simple randomisation method (www.random.org) as follows:
Group 1: Rotary File Systems
1A: The Mtwo system, manufactured by Dentsply-Maillefer in Ballaigues, Switzerland;
1B: The XP Endo Shaper (XPS), produced by FKG Dentaire SA in La Chaux-de-Fonds, Switzerland.
Group 2: Reciprocating File Systems
2A: The E-Flex Rec File, made by Orikam India;
2B: The WOG, produced by Dentsply Sirona in York, PA [Table/Fig-1].
Consolidated Standards of Reporting Trials (CONSORT) flow chart.
Study Procedure
Prior to administering the anaesthetic, a skin test was performed on the forearm using a 1:10 dilution of 2% lignocaine to ensure that the patient did not have an allergic reaction to the local anaesthetic. Once it was established that the patient was not allergic to the anaesthetic, the root canal procedure was initiated. Each patient received anaesthesia through a solution containing 2% lignocaine with 1:100,000 epinephrine.
The tooth was isolated with a rubber dam. A sanitised round bur was used to create coronal access after performing an occlusal cuspal reduction. The working length was determined and the instrument was kept 0.5 mm short of the radiographic apex. After the establishment of the working length, an initial glide path was created using a hand file.
Upon completion of instrumentation, irrigation was repeated with 5 mL of 3% Sodium Hypochlorite (NaOCl), followed by a final irrigation step using 5 mL of physiological saline solution (0.9%) to conclude the procedure.
Following instrumentation and irrigation, the canals were dried using paper points. The obturation process involved utilising a resin-based root canal sealer (AH Plus, Dentsply, Konstanz, Germany) along with a master cone gutta-percha. Upon completion of the root canal treatment, a periapical radiograph was taken to determine the accuracy of root canal obturation. To secure the treated teeth, a temporary restorative material was applied. Patients were then scheduled for the placement of a permanent restoration within seven days.
Assessment of outcomes: The primary outcome assessed in this study was the severity of postoperative pain, evaluated through a VAS at 24 hours, 48 hours, 72 hours and seven days. Each patient was provided with a VAS (ranging from 0 to 10) to assist the outcome assessor in evaluating pain levels while completing the postoperative questionnaire. The scale was thoroughly explained to patients both before the commencement of treatment and before leaving the clinic, utilising visual, verbal and numerical methods to ensure comprehension. Patients received instructions and were trained on how to fill out the VAS score. Subsequently, the outcome assessor contacted patients via telephone approximately 24 hours, 48 hours, 72 hours and seven days after treatment to record VAS scores for postoperative pain.
After the completion of endodontic therapy, patients were directed to use only 400 mg of ibuprofen as their analgesic, adhering to a therapeutic dose of one tablet every six hours in case of unbearable pain [18]. Analgesic consumption after 24 hours, 48 hours, 72 hours and seven days was also analysed.
Statistical Analysis
The data was entered into an Excel worksheet created by Microsoft (Microsoft, USA) after it was collected. The IBM Statistical Package for Social Sciences (SPSS, Version 21.0; Armonk, NY: IBM Corp.) was used to analyse the data. The Shapiro-Wilk test was employed to evaluate the normality of the data and it was found to be normally distributed. Categorical data were described in terms of frequencies and percentages, while continuous data were presented as means and Standard Deviations (SD). The comparison of means was conducted using one-way ANOVA, followed by post-hoc analysis using Tukey’s post-hoc test. For categorical data, the Chi-square test was used to compare the proportions. A p-value of less than 0.05 was considered statistically significant.
Results
The study involved four groups with the following gender distributions: Groups 1A and 2B each had 10 males (50%) and 10 females (50%), Group 1B had 11 males (55%) and 9 females (45%), while Group 2A had 9 males (45%) and 11 females (55%) [Table/Fig-2]. [Table/Fig-3] shows that the mean ages were 39.00±12.70 years for Group 1A, 34.70±9.48 years for Group 1B, 42.15±12.59 years for Group 2A and 39.10±13.65 years for Group 2B, with no significant differences between groups (p-value >0.05).
Gender-wise distribution of study participants in the groups.
| Gender | 1A | 1B | 2A | 2B |
|---|
| n | % | n | % | n | % | n | % |
|---|
| Male | 10 | 50% | 11 | 55% | 9 | 45% | 10 | 50% |
| Female | 10 | 50% | 9 | 45% | 11 | 55% | 10 | 50% |
| Total | 20 | 100% | 20 | 100% | 20 | 100% | 20 | 100% |
Comparison of mean age of study participants in various groups.
| Group | Mean | SD | Minimum | Maximum | F value, p-value |
|---|
| 1A | 39.00 | 12.70 | 20 | 60 | F=1.295, p=0.295 NS |
| 1B | 34.70 | 9.48 | 19 | 54 |
| 2A | 42.15 | 12.59 | 25 | 65 |
| 2B | 39.10 | 13.65 | 19 | 66 |
NS: Not significant
The mean VAS scores were assessed postoperatively across various time intervals. In Group 1A, scores decreased significantly from 6.55±1.09 at 24 hours to 0 at seven days (p-value <0.001) [Table/Fig-4]. Group 1B exhibited similar trends, with scores dropping from 5.55±0.94 at 24 hours to 0 at seven days (p-value <0.001) [Table/Fig-5]. In Group 2A, scores reduced from 3.55±0.94 at 24 hours to 0 at seven days (p-value <0.001) [Table/Fig-6]. Group 2B showed a decrease from 4.55±1.05 at 24 hours to 0 at seven days (p-value <0.001) [Table/Fig-7]. All comparisons between intervals within each group were statistically significant. By the 7th day, no pain was reported in any group.
Mean VAS scores in group 1A at various time intervals postoperatively.
| Time | Mean | SD | F value, p-value |
|---|
| 24 hours | 6.55 | 1.09 | F=262.617,p<0.001** |
| 48 hours | 5.10 | 0.96 |
| 72 hours | 1.80 | 0.76 |
| 7 days | 0.00 | 0.00 |
| Between times | p-value |
| 24 hours vs 48 hours | <0.001** |
| 24 hours vs 72 hours | <0.001** |
| 24 hours vs 7 days | <0.001** |
| 48 hours vs 72 hours | <0.001** |
| 48 hours vs 7 days | <0.001** |
| 72 hours vs 7 days | <0.001** |
**Statistically highly significant
Mean VAS scores in group 1B at various time intervals postoperatively.
| Time | Mean | SD | F value, p-value |
|---|
| 24 hours | 5.55 | 0.94 | F=300.765,p<0.001** |
| 48 hours | 3.90 | 0.71 |
| 72 hours | 0.70 | 0.65 |
| 7 days | 0.00 | 0.00 |
| Between times | p-value |
| 24 hours vs 48 hours | <0.001** |
| 24 hours vs 72 hours | <0.001** |
| 24 hours vs 7 days | <0.001** |
| 48 hours vs 72 hours | <0.001** |
| 48 hours vs 7 days | <0.001** |
| 72 hours vs 7 days | 0.009* |
*Statistically significant; **Statistically highly significant
Mean VAS scores in group 2A at various time intervals postoperatively.
| Time | Mean | SD | F value, p-value |
|---|
| 24 hours | 3.50 | 0.94 | F=123.383, p<0.001** |
| 48 hours | 1.70 | 0.80 |
| 72 hours | 0.15 | 0.36 |
| 7 days | 0.00 | 0.00 |
| Between times | p-value |
| 24 hours vs 48 hours | <0.001** |
| 24 hours vs 72 hours | <0.001** |
| 24 hours vs 7 days | <0.001** |
| 48 hours vs 72 hours | <0.001** |
| 48 hours vs 7 days | <0.001** |
| 72 hours vs 7 days | 0.768 NS |
NS: Not significant; **Statistically highly significant
Mean VAS scores in group 2B at various time intervals postoperatively.
| Time | Mean | SD | F value, p-value |
|---|
| 24 hours | 4.55 | 1.05 | F=232.066,p<0.001** |
| 48 hours | 2.45 | 0.60 |
| 72 hours | 0.20 | 0.41 |
| 7 days | 0.00 | 0.00 |
| Between times | p-value |
| 24 hours vs 48 hours | <0.001** |
| 24 hours vs 72 hours | <0.001** |
| 24 hours vs 7 days | <0.001** |
| 48 hours vs 72 hours | <0.001** |
| 48 hours vs 7 days | <0.001** |
| 72 hours vs 7 days | 0.877 NS |
NS: Not significant; **Statistically highly significant
Comparative analyses between groups at specific intervals revealed significant differences. At 24 hours, Group 1A had the highest VAS scores, while Group 2A had the lowest (p-value <0.05) [Table/Fig-8]. At 48 hours, all groups showed highly significant differences in VAS scores (p-value <0.001), with Group 2A consistently having the lowest scores [Table/Fig-9]. By 72 hours, Group 1A had significantly higher scores than the others (p-value <0.001), while the differences between Group 2A and Group 2B were not significant [Table/Fig-10].
Mean VAS scores at 24 hours postoperatively, among various groups.
| Group | Mean | SD | F value, p-value |
|---|
| 1A | 6.55 | 1.09 | F=33.530,p<0.001* |
| 1B | 5.55 | 0.94 |
| 2A | 3.5 | 0.94 |
| 2B | 4.55 | 1.05 |
| Between groups | p-value |
| 1A vs 1B | 0.013* |
| 1A vs 2A | <0.001** |
| 1A vs 2B | <0.001** |
| 1B vs 2A | <0.001** |
| 1B vs 2B | 0.013* |
| 2A vs 2B | 0.008* |
*Statistically significant; **Statistically highly significant
Mean VAS scores at 48 hours postoperatively, among various groups.
| Group | Mean | SD | F value, p-value |
|---|
| 1A | 5.10 | 0.96 | F=74.584, p<0.001** |
| 1B | 3.90 | 0.71 |
| 2A | 1.70 | 0.80 |
| 2B | 2.45 | 0.60 |
| Between groups | p-value |
| 1A vs 1B | <0.001** |
| 1A vs 2A | <0.001** |
| 1A vs 2B | <0.001** |
| 1B vs 2A | <0.001** |
| 1B vs 2B | <0.001** |
| 2A vs 2B | 0.018* |
*Statistically significant; **Statistically highly significant
Mean VAS scores at 48 hours postoperatively, among various groups.
| Group | Mean | SD | F value, p-value |
|---|
| 1A | 1.80 | 0.76 | F=35.494, p<0.001** |
| 1B | 0.70 | 0.65 |
| 2A | 0.15 | 0.36 |
| 2B | 0.20 | 0.41 |
| Between groups | p-value |
| 1A vs 1B | <0.001** |
| 1A vs 2A | <0.001** |
| 1A vs 2B | <0.001** |
| 1B vs 2A | 0.037* |
| 1B vs 2B | 0.018* |
| 2A vs 2B | 0.993 NS |
NS: Not significant; *Statistically significant; **Statistically highly significant
Analgesic consumption was also analysed. At 24 hours postoperatively, more participants in Groups 2A and 2B required fewer analgesics compared to Groups 1A and 1B, showing significant differences (p-value=0.001). By 48 hours, analgesic use declined across all groups and none required analgesics at 72 hours or on the 7th day. These findings underscore the effective reduction of pain over time in all groups, with significant variation in analgesic needs [Table/Fig-11].
Consumption of analgesic amongst the groups at various time intervals postoperatively.
| No. of analgesics taken | 1A | 1B | 2A | 2B | χ2, p-value |
|---|
| n | % | n | % | n | % | n | % |
|---|
| 24 hours | 0 | 4 | 20% | 7 | 35% | 16 | 80% | 13 | 65% | χ2=23.667 p=0.001* |
| 1 | 9 | 45% | 8 | 40% | 4 | 20% | 7 | 35% |
| 2 | 7 | 35% | 5 | 25% | 0 | 0% | 0 | 0% |
| 48 hours | 0 | 8 | 40% | 11 | 55% | 18 | 90% | 16 | 80% | χ2=14.032, p=0.003* |
| 1 | 12 | 60% | 9 | 45% | 2 | 10% | 4 | 20% |
| 2 | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% |
| 72 hours | 0 | 20 | 100% | 20 | 100% | 20 | 100% | 20 | 100% | - |
| 1 | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% |
| 2 | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% |
| 7 days | 0 | 20 | 100% | 20 | 100% | 20 | 100% | 20 | 100% | - |
| 1 | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% |
| 2 | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% |
*Statistically significant
Discussion
Pain is a multifaceted phenomenon and is often regarded as the fifth vital sign. According to the International Association for the Study of Pain, it is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage. Postoperative pain following root canal treatment is characterised by the perception of discomfort that occurs after endodontic intervention [19].
Nevertheless, instrumentation of the root canal has been linked to the onset of postoperative pain [20], a phenomenon that can vary based on the technique employed [21] or the specific instrumentation system utilised. This study was planned to assess and compare postoperative pain following endodontic treatment using WOG and E-Flex Rec (reciprocating systems) versus Mtwo and XP Endo Shaper (rotary systems). Several factors can influence the results of endodontic treatment. The patient’s age and gender, arch position, tooth type and periapical status have been identified as potentially important prognostic factors [22].
In the context of the ongoing research, the examination of demographic data yielded outcomes indicating that there is no statistically meaningful distinction in the mean age among the studied participants. In the current study, participants aged 19-70 years were included. Similar age groups were included in studies conducted by other authors [12,23,24]. The mean age of participants was 39.00±12.70, 34.70±9.48, 42.15±12.59 and 39.10±13.65 years in groups 1A, 1B, 2A and 2B, respectively. No significant difference was observed in the mean age among the groups. This finding is in agreement with studies conducted by Pamboo J et al., Walton R and Fouad A and Mor C et al., wherein no significant difference was found between groups based on mean age [25-27].
This study, focusing on single-visit endodontic treatment for both single and multirooted teeth diagnosed with asymptomatic irreversible pulpitis without apical periodontitis, utilised the VAS. Pain levels were recorded at 24 hours, 48 hours and 72 hours, as well as on the 7th day, using a scale ranging from 0 to 10. The choice of VAS in this research is based on its extensive application in pain level assessments and its established reliability in prior studies [28-31].
A single-visit endodontic treatment approach was chosen to simplify the protocol, make the process transparent and minimise the risk of discrepancies in intracanal medication application. After endodontic therapy, Non Steroidal Antiinflammatory Drugs (NSAIDs) have been widely recommended as the primary medication for postoperative pain control. The decision to use ibuprofen was influenced by its well-documented antiiinflammatory properties, analgesic effects and favourable safety profile [32,33].
In this study, the maximum postoperative pain was experienced by patients in the first 24 hours and the pain gradually decreased over the next 48 and 72 hours in all groups. By the 7th day, none of the patients in any group reported experiencing pain. In a systematic review, Pak JG and White SN found that the prevalence of postoperative pain decreased significantly during the first 48 hours after root canal treatment and dropped to 10% or less after the first week, which was consistent with the results of the current study [8]. The maximum intensity of pain was experienced by patients using the Mtwo rotary file system, followed by the XP Endo Shaper rotary file system, the WOG reciprocating file system and the E-flex reciprocating file system, in decreasing order across all time intervals. The differences between the groups were statistically significant. Thus, pain experienced was greater with rotary file systems compared to reciprocating file systems.
The high incidence of postoperative pain associated with the XP Endo Shaper can be attributed to its alloy, diameter and the kinematic movements applied during its use. The instrument deforms or changes its shape during canal preparation at body temperature, leading to dimensional changes that are beyond the operator’s control and can potentially damage the Periodontal Ligament (PDL). This PDL damage is linked to the release of Substance P as well as Calcitonin Gene-related Peptide (CGRP) [34]. Additionally, the use of high speed and a greater tip diameter results in a higher amount of debris extrusion due to increased wear of the dentinal walls [35]. These findings align with a study by Pawar AM et al., which compared postoperative pain using the XP Endo Shaper with the self-adjusting file system and hand K-files. They found that pain levels with the XP Endo Shaper were higher compared to the self-adjusting file system but lower than those associated with hand K-files [12].
In this study, postoperative pain in the M-Two group was less than that of the XP Endo Shaper file system. The design characteristics of the M-Two file system can be attributed to its S-shaped cross-section and flute design, which tend to pull debris back towards the orifices, leading to less debris extrusion and, consequently, reduced postoperative pain for the patients [36]. In contrast, the XP Endo Shaper file system, with its continuous rotation, high speed and greater tip diameter, results in a higher volume of debris extrusion [34]. Based on file design and motion kinematics, these results are consistent with several studies [12,35] that show reduced debris extrusion associated with M-Two file systems. The progressive pitch of the M-Two files reduces the possibility of debris extrusion at the apical region by creating space for dentin removal. Furthermore, by rotating continuously, the file can function as a screw conveyor, enhancing the coronal transportation of dentin chips and debris [36].
In the present study, higher intensity postoperative pain was observed among patients treated with rotary file systems compared to those treated with reciprocating file systems. A systematic review conducted by Martins CM et al., observed that continuous rotary motion has an adverse effect on postoperative pain following endodontic treatment when compared to reciprocating motion, aligning with the outcomes of this study [16].
In the current study, the Wave One Gold reciprocating file system demonstrated less postoperative pain compared to the rotary file system. This could be attributed to its single-file system with safety non cutting tips. These features help maintain the original path of the root canal, which in turn reduces unnecessary wear of the dentinal walls, producing less debris and ultimately resulting in less apical extrusion. The design of the file also facilitates the upward movement of debris. These results align with the study conducted by Xavier F et al., who found that the Wave One Gold caused less postoperative pain compared to the XP Endo Shaper [34].
In contrast to the present study’s results, a randomised clinical trial conducted by Nekoofar MH et al., demonstrated a noteworthy disparity, showing significantly lower postoperative pain in patients treated with the ProTaper Universal rotary system compared to those treated with the Wave One reciprocating system [37].
The E-Flex Rec reciprocating file system exhibited the lowest postoperative pain compared to the other file systems used in this study. This could be attributed to its composition of heat-treated control memory NiTi wire, which features a double-edge cross-section with safety non cutting tips and operates as a single-file system. Its variable pitch increases from the tip to the handle, preventing suction and locking, thereby reducing the apical extrusion of debris [38]. There is a paucity of literature regarding the in-vivo use of the E-Flex Rec file system. Based on the aforementioned design characteristics, the E-Flex Rec file system may explain the least postoperative pain observed among all groups.
As depicted in [Table/Fig-11], reciprocating file systems resulted in less postoperative pain compared to rotary file systems, which is consistent with the findings of our study that utilised various brands of file systems.
In the present study, the intake of analgesics at 24 and 48 hours postoperatively was statistically significantly higher in the rotary file system groups compared to the reciprocating file systems, with no analgesic consumption recorded after 48 hours. These results are not in agreement with studies conducted by Kherlakian D et al., and Adiguzel M et al., who found no difference in analgesic consumption between rotary and reciprocating file systems [29,39]. A comparison of the results of the current study with similar studies has been presented in [Table/Fig-12] [12,28,34].
Comparison of results of current study with similar studies [12,28,34].
| S. No. | Author’s name and year | Place of study | Number of subjects | Files compared | Parameters assessed | Conclusion |
|---|
| 1. | Bansod A et al., (2024)(Present study) | Karad, Maharashtra | 80 | Mtwo, XP Endo Shaper. E-Flex Rec File, WaveOne Gold (WOG) | Postoperative pain at hours, 48 hours, 72 hours, and 7 days using VAS analgesic consumption | Postoperative: M-Two group >XP Endo Shaper>WaveOne Gold (WOG)>E-flex RecAnalgesic consumption: Mtwo>XP Endo Shaper>WaveOne Gold (WOG)>E-flex Rec |
| 2. | Neelakantan P and Sharma S, (2015) [28] | Chennai, India | 605 | Reciproc, One Shape | Postoperative pain every day till 7 days. | One Shape>Reciproc |
| 3. | Xavier F et al., (2021) [34] | Brazil | 148 | XP Endo Shaper, WaveOne Gold (WOG) | Postoperative pain at 24, 48, and 72 hours and 7 days. | XP Endo Shaper>WaveOne Gold (WOG) |
| 4. | Pawar AM et al., (2022) [12] | Rau, Madhya Pradesh | 120 | XP Endo shaper sequence, full-sequence self-adjusting file and manual K-files | Postoperative pain at 6 hours, 24 hours, 48 hours and 72 hours using VAS | Hand K-files>XP Endo Shaper>Self adjusting file system |
The apical third of the root canal is particularly crucial, given the presence of ramifications and lateral canals with a high prevalence of bacterial biofilms, sometimes extending into the extraradicular region [39]. Given that the elimination and prevention of infection within the root canal system are fundamental to root canal treatment, the apical portion becomes a critical zone for chemomechanical preparation [40].
Limitation(s)
The present study has inherent limitations due to the in-vivo nature of the conditions. The inability to standardise the final apical preparation sizes arises from the unique dimensions of each root canal. While the collected sample size was sufficient to achieve statistical significance, a larger number of participants might have revealed additional statistically significant data that could differentiate between the two treatment modalities. Uniformity in variables, such as the number of root canals (i.e., single-rooted or multi-rooted teeth) and baseline health status, can reduce variability related to individual differences, thereby eliminating their effect on the results. Another important aspect is that pain, being a subjective symptom, might result in bias depending on the pain threshold of the patient, which varies from individual to individual.
Conclusion(s)
Given the constraints inherent in the present study, it can be concluded that postoperative pain was statistically significantly higher in rotary file systems compared to reciprocating file systems. Specifically, postoperative pain was significantly higher in the M-two group, followed by the XP Endo Shaper, WOG and E-flex Rec. Additionally, the consumption of analgesics was also statistically significantly higher in rotary file systems compared to reciprocating file systems, with the following order observed: M-two, XP Endo Shaper, WOG and E-Flex Rec.
NS: Not significant
**Statistically highly significant
*Statistically significant; **Statistically highly significant
NS: Not significant; **Statistically highly significant
NS: Not significant; **Statistically highly significant
*Statistically significant; **Statistically highly significant
*Statistically significant; **Statistically highly significant
NS: Not significant; *Statistically significant; **Statistically highly significant
*Statistically significant