Introduction
The complete removal of Calcium Hydroxide {Ca(OH)2} using various techniques remains a challenge in root canal therapy. One of the most commonly used methods for removing calcium hydroxide is by using a Master Apical File (MAF) along with sodium hypochlorite and Ethylenediaminetetracetic Acid (EDTA). Various new modalities, like Canal Brush, NaviTip and file systems, have emerged to tackle the residual calcium hydroxide in the canal; but none of these methods have been able to completely remove it from the canal.
Aim
To evaluate and compare the efficacy of H-files, NaviTip FX and Canal Brushes in removing calcium hydroxide intracanal medicament from root canals.
Materials and Methods
This in-vitro study was carried out in the Department of Conservative Dentistry and Endodontics at KM Shah Dental College and Hospital, Vadodara, Gujarat, India, from December 2023 to March 2024. To standardise the length at 14 mm, 30 mandibular premolar teeth (n=30) with a single root were decoronated at the Cementoenamel Junction (CEJ). The working length was determined, followed by the cleaning and shaping of all specimens using ProTaper Rotary Files. Intracanal medicament (Metapex) was placed and the canals were sealed with Glass Ionomer Cement (GIC). The specimens were then placed at 37±1°C and 100% relative humidity for 30 days. The medicament was subsequently removed by three different protocols: H-file, NaviTip FX and Canal Brush (n=10 each). The residual volumes in the mesial, distal and apical thirds were assessed, referring to the volume of medicament left in the canal, which was measured using Cone-beam Computed Tomography (CBCT). The recorded variables were analysed using one-way Analysis of Variance (ANOVA) post-hoc tests (p<0.05).
Results
The Canal Brush removed the maximum amount of Metapex in the apical third (0.108) of the roots of the premolars, followed by NaviTip FX and then H-file. In the middle third of the root, NaviTip FX removed more Metapex than the Canal Brush, followed by H-files. A comparison of retrieval between and within the groups it showed that none of the techniques were capable of removing all the Metapex from the specimens, with p>0.05.
Conclusion
The present study demonstrated that the Canal Brush showed superior results in retrieving Metapex from the apical third of the root and the distal side (middle third), whereas NaviTip FX removed more Metapex from the mesial side (middle third) of the root, but H-file exhibited the least efficacy in the retrieval of Metapex. Total removal of calcium hydroxide from the entire canal is not possible regardless of the technique used.
Introduction
Intracanal medicaments aim to eliminate bacteria in the root canal and prevent their proliferation inside the canal, thus preventing reinfection [1]. A vital pulp treatment does not require an intracanal medicament; however, periradicular diseases like apical periodontitis necessitate these antibacterial medications to eradicate microbial growth that has not been adequately instrumented or irrigated [2]. In cases like periapical periodontitis, intracanal dressing plays a major role. Calcium hydroxide is one such intracanal dressing that is most widely used during the interappointment period, as it can inactivate bacterial Lipopolysaccharides (LPS), induce the formation of mineralised tissue and change the pH through the diffusion of hydroxyl ions [3]. Various factors, like anatomical complexities of the root canal system, the irrigating solution used, the medicament formulation and the use of chelating agents and techniques for removal, affect the removal of medicament removal. Due to the anatomical complexities of the root canal system, cleaning and shaping is a major challenge [4]. The medicament placed within root canals should be removed before obturation, as residual material on the canal walls can hinder sealer penetration into the dentinal tubules, which can lead to microleakage [5].
Calcium hydroxide, as an intracanal medicament, can be placed inside the root canal for different time durations depending upon the clinical situation [6]. The mechanism of action which takes place is that since Ca(OH)2 is unstable in aqueous environments, causing it to immediately dissociate into calcium and hydroxyl ions. The high concentration of these hydroxyl ions damages the bacterial cytoplasmic membrane.
Also, these calcium and hydroxyl ions promote mineralisation in the root canal, leading to hard tissue formation.
A major drawback of calcium hydroxide as an intracanal medicament is that it has to be completely removed before the final obturation, as it hinders the penetration of sealer into the tubules, leading to increased apical leakage of the treated tooth. It also causes granulation and brittleness of zinc oxide-eugenol-based sealers [7].
Complete removal of Ca(OH)2 using various techniques remains a challenge in root canal therapy and several studies assessing the ability to remove Ca(OH)2 have been published over recent years [8]. One of the most commonly used methods for removing calcium hydroxide is by using a MAF along with sodium hypochlorite and EDTA in combination [9,10]. The combination of Nickel Titanium (NiTi) instruments along with Sodium Hypochlorite (NaOCl) and passive ultrasonic irrigation has also been an effective removal method.
During the early 1990s, Keir et al., reported that the Endobrush improved canal debridement [11]. Their results showed that the Endobrush was significantly better than instrumentation alone in debriding the root canal. The major problem with the Endobrush was that it could not be used to the full working length because of its size, which might lead to the packing of debris into the apical section of the canal after brushing.
Another recently used technique is the Canal Brush (Roeko Canal BrushTM, Coltène/Whaledent, Langenau, Germany). It is a flexible endodontic microbrush that can be used either manually or with a contra-angle handpiece at a speed of 600 rpm. According to International Organisation for Standardisation (ISO) classification, Canal Brushes are available in three sizes (small, medium and large), which correspond to the apical diameters of 25, 30 and 40, respectively. The Canal Brush can be used along with NaOCl for about 30 seconds at a speed of 650 rpm [12]. A study reported by Garip Y et al., concluded that the Canal Brush, along with irrigating solutions, removes debris more effectively from root extensions and irregularities than irrigation alone [13]. Another author advocated the use of an endodontic file or broach wrapped in cotton and compared it with the Endobrush. It was concluded that the cotton wrapped around a file or broach was not able to clean the canal properly, especially in irregularities, whereas the Endobrush used with hand instrumentation demonstrated better cleaning [14,15].
An irrigation needle covered with a brush (NaviTip FX, Ultradent UT) is one more contribution that aids in the removal of calcium hydroxide from the canal. NaviTip FX (Ultradent Products Inc., South Jordan, UT) features optimal delivery tips designed in such a way that the base and centre, while the tip remains flexible, allowing for easy navigation of curved canals [16,17]. The literature has reported the use of needle NaviTip FX needle in removing the smear layer. Studies have also evaluated the effectiveness of NaviTip FX in removing calcium hydroxide from root canals [18].
Passive ultrasonic agitation of irrigants is a current area of interest in the field of endodontics. During ultrasonically activated irrigation, a piezoelectric element drives an oscillating file in the canal at frequencies of 25-30 kHz, resulting in acoustic streaming and cavitation within the root canal. Thus, acoustic energy from the file to the solution. Ultrasonic agitation of irrigants is an additional step that follows syringe irrigation. The irrigant is first delivered and then activated [19].
Three-dimensional volume analysis using CBCT is used in the field of dentistry for various applications. Volumetric analysis using CBCT gives a more accurate measurement of pre- and post-removal of calcium hydroxide from root canals. However, very few studies have compared the effectiveness of different techniques for the removal of calcium hydroxide using CBCT [20].
Similarly, there are limited studies that have compared mechanical means to evaluating the retrieval of metapex from the canal [9,11-13,21]. Hence, the present study aimed to evaluate and compare the efficiency of various calcium hydroxide removal techniques, namely H-file, NaviTip FX and Canal Brush, using CBCT.
Materials and Methods
The present in-vitro study was carried out in the Department of Conservative Dentistry and Endodontics at KM Shah Dental College and Hospital in Vadodara, Gujarat, India for about four months, from December 2023 to March 2024. The Institutional Review Board (IRB) determined that the protocol is exempt because this is an in-vitro study and does not involve any animals or humans.
Sample size calculation: The sample size calculation was conducted using a Chi-square test family and variance statistical test (G*Power 3.1 software; Heinrich Heine University, Düsseldorf, Germany) with α=0.05 and β=0.95. A minimum sample size of 10 per group was calculated.
Inclusion and Exclusion criteria: All the samples were prepared by a single operator (DC). A total of 30 freshly extracted single-rooted mandibular premolar teeth with completely formed apices, having angles of curvature ranging between 50 and 250 degrees (as described by Schneider in 1971), were collected [22]. Teeth with resorptive defects, developmental anomalies, caries, root fractures, cracks and canal calcifications were excluded from the study. The experimental teeth were kept in a physiological saline solution after their external root surfaces were cleared of debris and adhering remnants using a periodontal curette.
Study Procedure
The external root surfaces of the experimental teeth were cleared of debris and adhering remains before being preserved in a physiological saline solution. Thirty mandibular premolar teeth with a single root were decoronated at the CEJ to standardise the length at 14 mm. A #15 K-file (Dentsply/Maillefer, Petropolis, Brazil) was inserted until it was visible at the apex to establish the working length. The working length was then determined by measuring the length and subtracting one millimetre from it.
An X-Smart electric motor (Dentsply Malleifer, Petrópolis, Brazil) was used with a torque control of 2 Ncm and a speed of 300 rpm. The canals were prepared using ProTaper Universal (Dentsply Malleifer, Petrópolis, Brazil). Canal preparation was performed using the crown-down technique, according to manufacturer’s instructions, up to finishing file 4 (F4) at the working length.
Using a syringe and a 30-gauge needle (Ultradent Products Inc., Indaiatuba, SP, Brazil), the canal was irrigated with 2 mL of a 2.5% Sodium Hypochlorite solution (NaOCl) (PREVEST DenPro) between each filling. The final rinse with 3 mL of 17% EDTA (PREVEST DenPro), followed by 5 mL of normal saline. The canals were dried using F4 paper points.
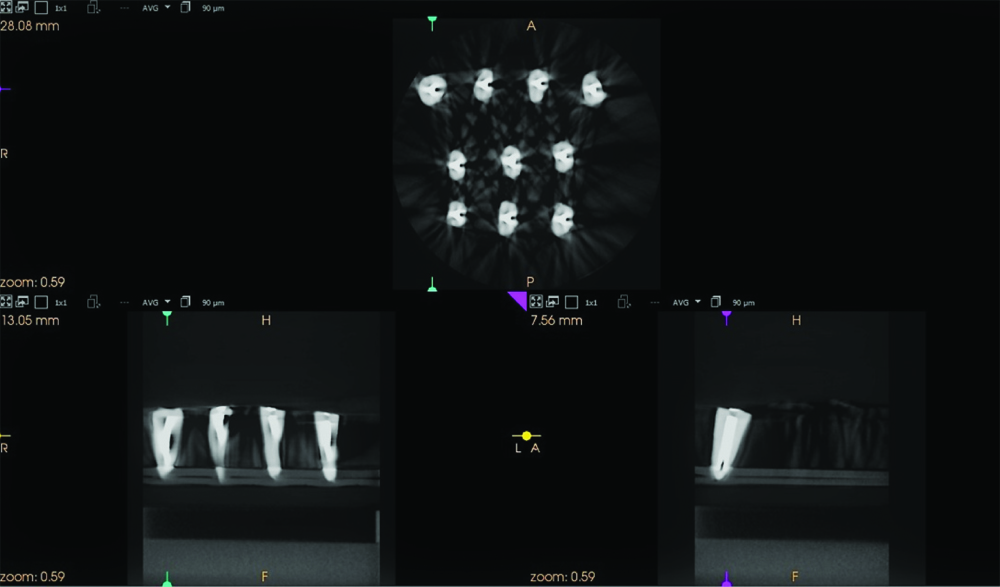
Root canals were filled with Metapex (Ca(OH)2, iodoform and silicon oil). The coronal part of the canal was then sealed with type II GIC. The teeth were stored at 37±1°C and 100% relative humidity for 30 days. After 30 days, 1st CBCT scan was performed to assess the total volume of METAPEX in the canal (a) [Table/Fig-1].
Illustrates CBCT scan before retrieval of metapex.
Samples were randomly (Computer randomisation method) divided into three experimental groups (n=10) depending on the calcium hydroxide removal technique.
Group 1: In this group, Metapex was removed using an H-file (#40). Irrigation was done using 2 mL of 2.5% NaOCl with the #40 H-file placed through the working length, followed by filing for one minute. This was followed by a rinse with 3 mL of 17% EDTA for three minutes.
Group 2: In this group, Metapex was removed using the NAVITIP FX irrigation needle (brush-covered) with the aid of an H-file (#40). Irrigation was performed with 2 mL of 2.5% NaOCl for one minute, followed by a rinse with 3 mL of 17% EDTA for three minutes.
Group 3: In this group, Metapex was removed with a canal brush. The root canals were cleaned using a #40 H-file, followed by irrigation with 2 mL of 2.5% NaOCl for one minute. A medium-sized canal brush was then placed in a slow-speed handpiece running at 600 rpm and advanced to the working length. A circumferential motion was made with the canal brush for 30 seconds. This was followed by a rinse with 3 mL of 17% EDTA for three minutes.
All canals were dried by paper points after the removal of the medicament was completed. After the removal of Metapex 2nd CBCT scan was done to assess the residual volume of medicament left in the canal.
CBCT scanning: Two CBCT scans were performed on each sample to get the canal volume in cubic millimetres:
The first scan was conducted after the placement of Metapex inside the root canal and a storage period of 30 days [Table/Fig-1], which illustrates CBCT scan before retrieval of metapex).
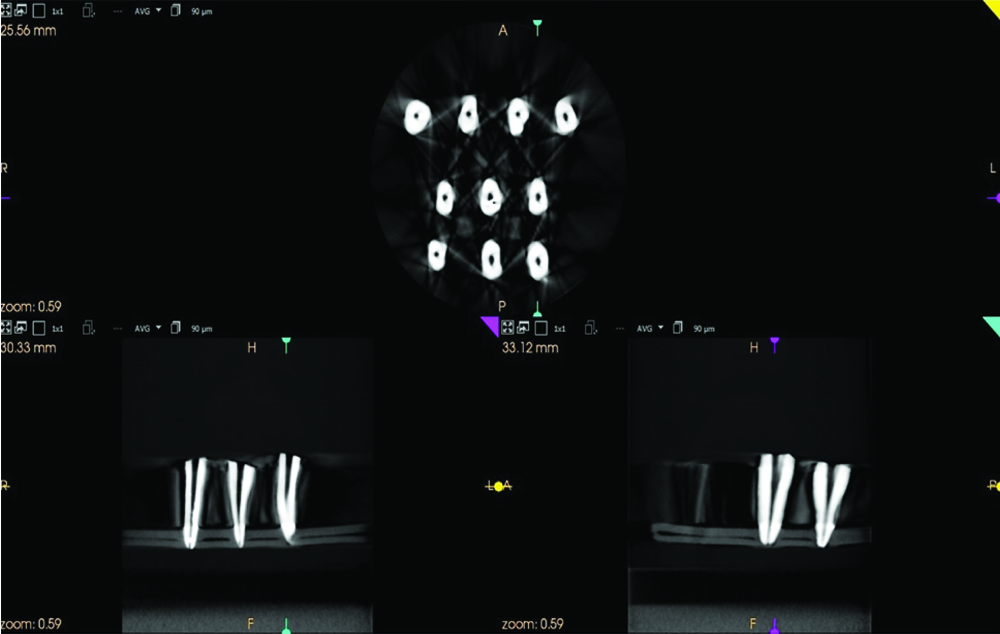
The second scan was performed to assess the residual volume of Metapex left after its removal from the middle third (both the mesial and distal sides) and the apical third of the root canals [Table/Fig-2], which depicts the CBCT scan after the removal of Metapex).
Depicts CBCT scan after removal of metapex.
Statistical Analysis
Descriptive and comparative statistics were performed using IBM Statistical Package for the Social Sciences (SPSS) version 21.0. Differences among the groups were analysed by analysis of variance tests and compared with post-hoc tests. A p-value of less than 0.05 was considered statistically significant for all tests. Variables were expressed as means±standard deviation.
Results
The Canal Brush removed the maximum amount of Metapex in the apical third of the roots (0.108 mm3) of the premolar, followed by NaviTip FX (0.138 mm3) and then the H-file (0.187 mm3). On evaluating both the mesial and distal sides of the middle third of the premolars, NaviTip FX removed more Metapex than the Canal Brush, followed by the H-file [Table/Fig-3].
Descriptive data showing the mean volumes of Metapex before and after removal from the mesial, distal sides of middle third and apical third of the canal.
| Technique | Mean±SD - Before removal of Metapex (mm3) | Mean±SD - residual metapex mesial side- Middle Thirs (mm3) | Mean±SD - residual metapex distal side- Middle Third (mm3) | Mean±SD - residual metapex apical third (mm3) |
|---|
| H-File(n=10) | 5.76±3.06 | 0.126±.17 | 0.129±0.21 | 0.187±0.37 |
| NaviTip FX (n=10) | 6.80±4.0 | 0.07±.195 | 0.08±0.248 | 0.138±0.24 |
| Canal brush (n=10) | 5.71±3.43 | 0.08±0.130 | 0.07±0.132 | 0.108±0.263 |
In comparison, the retrieval of Metapex among the groups showed that none of the techniques was capable of removing all the Metapex from the roots of the premolar, as indicated by p>0.05 {[Table/Fig-4]: Inter group analysis using ANOVA}.
Intergroup analysis using ANOVA comparing all of the techniques.
| Variables | Mean square | F | Sig. |
|---|
| Before removal of Metapex | Between groups | 3.813 | 0.306 | 0.739 |
| Within groups | 12.454 |
| After removal of Metapex (mesial side) | Between groups | 0.009 | 0.300 | 0.743 |
| Within groups | 0.029 |
| After removal of Metapex (distal side) | Between groups | 0.011 | 0.277 | 0.760 |
| Within groups | 0.041 |
| After removal of Metapex (apical third) | Between groups | 0.094 | 1.389 | 0.267 |
| Within groups | 0.068 |
*Significant
The mean differences in the removal of Metapex from the mesial and distal sides of the middle third and apical third between the H-file, Canal Brush and NaviTip FX groups is shown in [Table/Fig-5]. It showed that none of the techniques was capable of completely removing Metapex from the roots of the premolar and no removal technique is better than the others [Table/Fig-5].
Showing the mean difference between all the techniques for the remaining Metapex on mesial and distal sides of middle third and apical third of the canal.
| Dependent variables | (I) gp | (J) gp | Mean difference (I-J) | Sig. |
|---|
| After removal of Metapex (mesial side) | H-file | CB | 0.048 | 1.000 |
| NT | H-file | 0.053 | 1.000 |
| CB | NT | 0.004 | 1.000 |
| After removal of Metapex (distal side) | H-file | CB | 0.064 | 1.000 |
| NT | H-file | 0.050 | 1.000 |
| CB | NT | 0.013 | 1.000 |
| After removal of Metapex (apical third) | H-file | CB | 0.187 | 0.359 |
| NT | H-file | 0.048 | 1.000 |
| CB | NT | -0.138 | 0.737 |
The Canal Brush showed overall superior results in retrieving Metapex from the apical third of the roots, whereas NaviTip FX removed more effective in removing Metapex from the mesial and distal sides of the middle third of the roots of the premolar, but the H-file file showed the least efficacy in retrieval of the Metapex.
Discussion
The present study attempted to evaluate the efficiency of the H-file, NaviTip FX and Canal Brush in removing calcium hydroxide-based intracanal medicaments. Recapitulation with a Master Apical File (MAF) in combination with conventional needle irrigation has been shown to improve the removal of Ca(OH)2 compared to a final irrigant flush alone [13]. The frequently described technique uses a MAF at working length in conjunction with irrigation using sodium hypochlorite and EDTA. The most commonly described method is instrumentation along with irrigation by sodium hypochlorite and EDTA, combined with the use of a MAF at working length [13,23,24]. Nowadays, passive ultrasonic irrigation used along with mechanical means, have resulted in thorough cleaning of the canal system [25]. Instrument motions performed to disrupt and loosen the medication are up-and-down filing/oscillation with a #15 K-file or #40 H-file [23], a reaming motion with a small endodontic instrument, or with the MAF [24]. In this study, a #40 H-file was used along with various calcium hydroxide removal techniques.
The results of this in-vitro study demonstrated that the removal of calcium hydroxide was most effectively performed by the NaviTip FX and Canal Brush. The effectiveness of the NaviTip FX irrigation needle in removing intracanal calcium hydroxide in the apical third may be associated with the mechanical action of the bristles during the irrigation process, which increases the debridement of the root canal walls [26]. A study using NaviTip concluded that close contact with the bristles in the apical portion of the canal results in mechanical friction. During the rollback (incoming and outgoing movement) of the NaviTip FX needle, the bristles keep contact with the dentin walls, hindering the return of the solution and promoting greater pressure of the irrigating fluid and turbulent flow in the vicinity of or between the bristles. Thus, the washing action facilitated by the use of NaviTip FX may have been facilitated by the change in flow dynamics [27].
Regardless of the mechanical means used in the study, none of the tested methods was able to completely remove the Ca(OH)2 medicament from the samples. Jain A et al., compared the efficiency of H and K files and also single and multiple rotary file systems, in the removal of calcium hydroxide. They concluded that a multiple rotary file system is more effective in the removal of Ca(OH)2 than a single file system [28].
Similar research done compared the effectiveness of ultrasonic and manual techniques in calcium hydroxide removal, determined that neither manual nor ultrasonic techniques completely removed calcium hydroxide from the root canal [29,30]. Gorduysus M et al., evaluated the effectiveness of the Canal Brush in removing Ca(OH)2 from the root canal system using SEM and, after placing the medicaments, stored their samples in 100% humidity for one week at 37°C [31]. They concluded that it is essential to re-instrument the root canal walls using instrumentation techniques while irrigating with a combination of NaOCl and EDTA. The Canal Brush technique resulted in the packing effect of the Ca(OH)2 through to the apex.
Markovic L et al., evaluated the efficacy of the canal brush, either used with permanent rotation or sonic activation, in removing calcium hydroxide from root canals compared to syringe irrigation. They summarised that the canal brush significantly improves the removal of calcium hydroxide [32], with no significant difference between rotary motion and sonic activation. However, Turker SA et al., conducted a study comparing calcium hydroxide removal by self-adjusting files, Endovac and Canal Brush agitation techniques. They found that, when it came to extracting Ca(OH)2 from the apical third of the root canals, SAF and EndoVac performed noticeably better than the Canal Brush and traditional syringe irrigation [33].
They determined that in the apical third of the root canals, SAF and EndoVac performed noticeably better than Canal Brush and traditional syringe irrigation. SAF and EndoVac demonstrated significantly better results than the Canal Brush and conventional syringe irrigation in removing Ca(OH)2 from the apical third of the root canals [33]. Another study by Silva FBR et al., compared the effectiveness of the NaviTip FX on intracanal calcium hydroxide removal. They concluded that the NaviTip FX irrigation needle shows greater effectiveness in removing calcium hydroxide medication than the NAVI TIP needle in the apical third of the canal [34].
Studies have shown that canal brushes exhibit reduced efficacy after 30 seconds of use due to deformation. Additionally, another drawback of using a canal brush is that it can lead to the accumulation of medicament in the apical region of the tooth, potentially causing extrusion into the periapical area [31].
Limitation(s)
The present research has certain limitations. Being an in-vitro study, the efficacy of various mechanical means of medicament removal is reduced, as the research was being carried out in a controlled laboratory environment. Also, more clinical research is required in this field, as the sample size was less and no patient participation was done. Another limitation that needs to be addressed is the amount of root dentin loss associated with mechanical methods used for the removal of Ca(OH)2. This loss can weaken the root, potentially leading to vertical root fractures later on.
Conclusion(s)
In the present study, the author found that mechanical means alone cannot completely remove oil-based calcium hydroxide (Metapex) from the canal. The adjunct use of agitated irrigation is required. Metapex removal of Metapex in the apical third of the roots of premolars using a canal brush was superior compared to the NaviTip FX and H-file. Additionally, the NaviTip FX removed more Metapex from the middle third of the roots, whereas the H-file showed the least efficacy in retrieving the Metapex. Thus, based on CBCT analysis, total removal of calcium hydroxide from the entire canal is not possible, regardless of the technique used.
Author’s contribution: DC: Conceptualisation, methodology, validation, resource, data curation, writing and supervision. All investigators have acknowledged the published version of the document.
*Significant
[1]. Zancan RF, Vivan RR, Milanda Lopes MR, Weckwerth PH, de Andrade FB, Ponce JB, Antimicrobial activity and physicochemical properties of calcium hydroxide pastes used as intracanal medicationJ Endod 2016 42(12):1822-28. [Google Scholar]
[2]. Mohammadi Z, Shalavi S, Yazdizadeh M, Antimicrobial activity of calcium hydroxide in endodontics: A reviewChonnam Med J 2012 48(3):133-40. [Google Scholar]
[3]. Alfadda S, Alquria T, Karaismailoglu E, Aksel H, Azim AA, Antibacterial effect and bioactivity of innovative and currently used intracanal medicaments in regenerative endodonticsJ Endod 2021 47(8):1294-300. [Google Scholar]
[4]. Uzunoglu-Ozyurek E, Erdogan AktemurTurker S, Effect of calcium hydroxide dressing on the dentinal tubule penetration of 2 different root canal sealers: A confocal laser scanning microscope studyJ Endod 2018 44:1018-23. [Google Scholar]
[5]. Hamdan R, Michetti J, Pinchon D, Diemer F, Georgelin-Gurgel M, The XP-Endo Finisher for the removal of calcium hydroxide paste from root canals and from the apical thirdJ Clin Exp Dent 2017 9(7):e855-60. [Google Scholar]
[6]. Lin J, Zeng Q, Wei X, Zhao W, Cui M, Gu J, Regenerative endodontics versus apexification in immature permanent teeth with apical periodontitis: A prospective randomized controlled studyJ Endod 2017 43(11):1821-27. [Google Scholar]
[7]. Hargreaves KM, Cohen P, Cohen’s pathway of pulp 2011 10th edMissouriMosby Elsevier [Google Scholar]
[8]. Usta SN, Eymirli A, Arias-Moliz MT, Evaluation of the removal of 2-Hydroxyisocaproic acid from the root canal and its effect on the bond strength of MTAAust Endod J 2023 49(2):311-17. [Google Scholar]
[9]. Donnermeyer D, Wyrsch H, Bürklein S, Schäfer E, Removal of calcium hydroxide from artificial grooves in straight root canals: Sonic activation using EDDY versus passive ultrasonic irrigation and XPendo FinisherJ Endod 2019 45(3):322-26. [Google Scholar]
[10]. Pereira TC, da Silva Munhoz Vasconcelos LR, Graeff MSZ, Ribeiro MCM, Duarte MAH, de Andrade FB, Intratubular decontamination ability and physicochemical properties of calcium hydroxide pastesClin Oral Investig 2019 23(3):1253-62. [Google Scholar]
[11]. Türker SA, Koçak MM, Koçak S, Sağlam BC, Comparison of calcium hydroxide removal by self-adjusting file, EndoVac, and Canal Brush agitation techniques: An in-vitro studyJ Conserv Dent 2013 16(5):439-43. [Google Scholar]
[12]. Thakur DA, Patil S, Gade V, Jogad N, Gangrade A, Sinkar R, Comparative scanning electron microscopy evaluation of Canal Brushing technique, sonic activation, and master apical file for the removal of triple antibiotic pastefrom root canal (in-vitro study)Contemp Clin Dent 2015 6(4):517-21. [Google Scholar]
[13]. Garip Y, Sazak H, Gunday M, Hatipoglu S, Evaluation of smear layer removal after use of a canal brush: An SEM studyOral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 110(2):e62-66. [Google Scholar]
[14]. Thé SD, The use of a cotton-wrapped file to evacuate necrotic pulp tissueOral Surg Oral Med Oral Pathol 1979 48(1):77-88. [Google Scholar]
[15]. Pashley DH, Kalathoors S, Burnhan D, The effects of calcium hydroxide on dentin permeabilityJ Dent Res 1986 65(3):417-20. [Google Scholar]
[16]. Shi L, Wu S, Yang Y, Wan J, Efficacy of five irrigation techniques in removing calcium hydroxide from simulated S-shaped root canalsJ Dent Sci 2022 17(1):128-34. [Google Scholar]
[17]. Goel S, Tewari S, Smear layer removal with passive ultrasonic irrigation and the NaviTip FX: A scanning electron microscopic studyOral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 108(3):465-70. [Google Scholar]
[18]. Bramante CM, Pinheiro BC, Garcia RB, Bramante AS, Bernardineli N, de Moraes IG, Efficacy of the NaviTip FX irrigation needle in removing calcium hydroxide from root canalJ Clin Exp Dent 2012 4(4):e226-29. [Google Scholar]
[19]. Van der Sluis LW, Versluis M, Wu MK, Wessenlink PR, Passive ultrasonic irrigation of the root canal: A review of the literatureInt Endod J 2007 40(6):415-26. [Google Scholar]
[20]. Pinsky HM, Dyda S, Pinsky RW, Misch KA, Sarment DP, Accuracy of three-dimensional measurements using cone-beam CTDentomaxillofac Radiol 2006 35(6):410-16. [Google Scholar]
[21]. Wang Y, Guo LY, Fang HZ, Zou WL, Yang YM, Gao Y, An in-vitro study on the efficacy of removing calcium hydroxide from curved root canal systems in root canal therapyInt J Oral Sci 2017 9(2):110-16. [Google Scholar]
[22]. Schneider SW, A comparison of canal preparations in straight and curved root canalsOral Surg Oral Med Oral Pathol 1971 32(2):271-75. [Google Scholar]
[23]. Tavella E Silva NC, Gibin JT, Rivera ICMM, Rached Junior FJA, Leoni GB, Raucci-Neto W, Calcium hydroxide paste removal strategies and bond strengths of epoxy- and silicate-based sealersAust Endod J 2021 47(2):236-44. [Google Scholar]
[24]. Uslu G, Gündoğar M, Üngör M, Özyürek T, Erkan E, Keskin NB, Investigation of the effectiveness of sonic, ultrasonic and new laser-assisted irrigation activation methods on smear removal and tubular penetrationLasers Med Sci 2023 38(1):30 [Google Scholar]
[25]. Gupta R, Sharma H, Kumari RA, Prakash AC, Rai N, Jain L, Effectiveness of two techniques in removal of calcium hydroxide medicament from root canals: An in-vitro assessmentJ Clin Diagn Res 2018 12(7):ZC53-ZC55. [Google Scholar]
[26]. Küçükkaya Eren S, Aksel H, Parashos P, A novel model for testing the efficiency of removal of calcium hydroxide from complex root canal anatomiesAust Endod J 2017 43(1):05-10. [Google Scholar]
[27]. Pérez AR, Alves FRF, Marceliano-Alves MF, Provenzano JC, Gonçalves LS, Neves AA, Effects of increased apical enlargement on the amount of unprepared areas and coronal dentine removal: A micro-computed tomography studyInt Endod J 2018 51(6):684-90. [Google Scholar]
[28]. Jain A, Patidar N, Nigam N, Bhadoria K, Choudhary B, An in-vitro study: Evaluation of intracanal calcium hydroxide removal with different file systemsIndian J Dent Sci 2017 9:26-29. [Google Scholar]
[29]. Yang Q, Liu M, Zhu L, Zhang J, Peng B, Comparison of needle, ultrasonic, and laser irrigation for the removal of calcium hydroxide from mandibular molar root canalsPhotobiomodul Photomed Laser Surg 2021 39(5):349-54. [Google Scholar]
[30]. Yücel AÇ, Gürel M, Güler E, Karabucak B, Comparison of final irrigation techniques in removal of calcium hydroxideAust Endod J 2013 39(3):116-21. [Google Scholar]
[31]. Gorduysus M, Yilmaz Z, Gorduysus O, Atila B, Karapinar SO, Effectiveness of a new canal brushing technique in removing calcium hydroxide from the root canal system: A scanning electron microscope studyJ Conserv Dent 2012 15(4):367-71. [Google Scholar]
[32]. Markovic L, Booth F, Zimmer S, Use of the CanalBrush improves removal of calcium hydroxide paste from instrumented straight root canalsJournal of Dental Sciences 2015 10(3):233-39. [Google Scholar]
[33]. Silva FBR, Fagundes NCF, Nogueira BCL, Silva LJM, Lima RR, Effectiveness of NaviTip FX on intracanal calcium hydroxide removalInt J Odontostomat 2016 10(1):143-48. [Google Scholar]