The Stomatognathic System (SS) is a complex network comprising the hard and soft tissues of the oral cavity, as well as components of the facial skeleton [1]. Dawson emphasised the need for a stable, balanced and harmonious occlusion that aligns with the surrounding orofacial structures [2]. Achieving occlusal neuromuscular harmony involves considering the interplay between the teeth, masticatory muscles, supporting periodontium and the temporomandibular joint. Any imbalances or discrepancies within these structures can result in detrimental consequences, such as tooth wear, muscle tension, pain and temporomandibular joint disorders [3]. A thorough diagnosis of bite force and muscle activity is required to ensure a patient’s masticatory function and comfort [4].
Mapelli A et al., found a positive correlation between muscle activity and bite force, indicating that higher muscle activity coincided with increased bite force [5]. Michier L et al., investigated the coordination between muscle activity and bite force during various chewing tasks [6]. The timing and intensity of muscle contractions, as measured by EMG, were closely associated with the corresponding changes in bite force. These findings highlighted the coordinated nature of masticatory function and the interdependence of muscle activity and bite force.
Several devices are commonly used to evaluate occlusal bite force, including electronic force sensors, tactile pressure sensors and surface Electromyography (sEMG) electrodes. T-Scan is a widely used digital occlusal analysis device that evaluates tooth contact, bite force and timing in real time [7]. However, the current system lacks devices for the simultaneous evaluation of both muscle activity and occlusal bite force in chairside clinical set-ups, leading to difficulties in diagnosis, need for additional inventory, increased treatment costs, suboptimal treatment outcomes and poor prognosis for restorations.
The present study aims to assess the efficacy of an ingeniously developed chairside diagnostic device that records occlusal bite force and muscle activity through an integrated bite force transducer and MyoWare sensors among dentate volunteers.
Materials and Methods
An observational study was conducted at the Department of Prosthodontics, Sri Ramachandra Dental College and Hospital (DU), Chennai, Tamil Nadu, India from February 5, 2024, to March 20, 2024, to validate the efficacy of an ingeniously designed integrated bite force and muscle activity recording device. Institutional Ethical Clearance (IEC-2) with reference number CSP- III/24/MAR/03/117 was obtained.
Sample size calculation: Sample size calculation was performed using the formula, with an effect size (d) of 2.3004620, an alpha error probability (α) of 0.05 and a power (1-β) of 0.99. The critical t-value was 2.1199053, resulting in a total sample size of 112. The actual power calculated was 0.9954786 [8].
Inclusion and Exclusion criteria: A total of 112 healthy dentate male and female volunteers aged between 21 and 35 years, who were apparently normal, were included as study participants. Participants with full coverage restorations, missing dentition, complex restorations covering the occlusal surface of the teeth, a history of temporomandibular joint disorders or any musculoskeletal disorders and those with pacemaker placements were excluded from the study.
Description of the device: The framework of the device comprises two key components: a square FSR - Alpha MF02A-N-221-A01, which is based on a piezoresistive force transducer and a MyoWare 2.0 muscle sensor from advancer technologies, used for measuring the electrical activity of muscles, as seen in [Table/Fig-1a]. The FSR sensor detects changes in resistance in response to applied force. This change in resistance can be used to quantify the amount of force exerted on the sensor. On the other hand, the MyoWare muscle sensor is placed on the skin over the targeted muscle to capture its electrical activity. The surface sensor is capable of recording electrical activity only from superficial muscles of mastication; deeply placed muscles of mastication be recorded with needle electrodes [9]. The muscle sensor converts the electrical signals generated by muscle contractions into measurable and analysable data.
a) Framework of the device with the various parts included; b) Android supportive MATLAB software for data intrepretation and storage; c) Device assembly on patient.
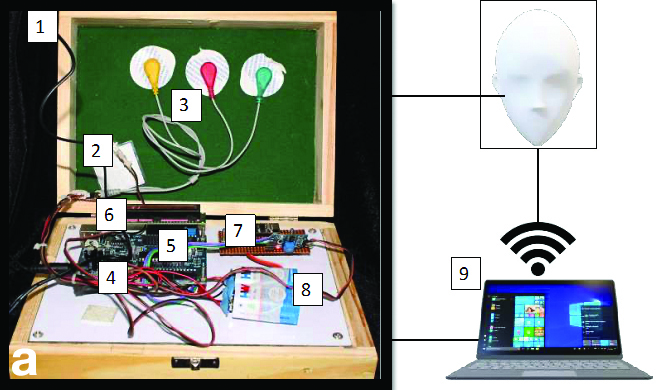 |
| S. No. | Part name | Part number |
| 1 | Integrated device | 1 |
| 2 | Force sensitive resistor | 2 |
| 3 | Muscle sensor with Arduino | 3 |
| 4 | Microcontroller | 4 |
| 5 | WiFi sensor | 5 |
| 6 | Amplifier | 6 |
| 7 | Capacitor | 7 |
| 8 | Power source | 8 |
| 9 | Computing system | 9 |
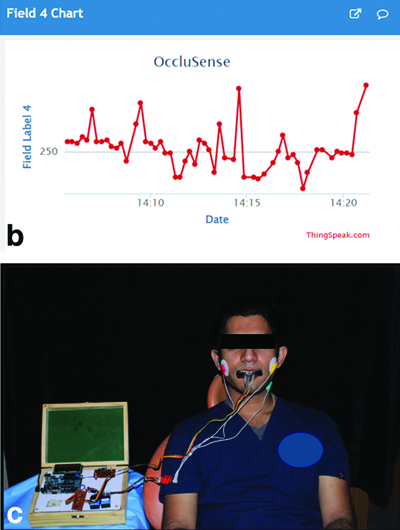 |
Both the FSR and MyoWare muscle sensors are connected to a microcontroller, which serves as the central processing unit of the device. The microcontroller is equipped with a Wi-Fi sensor, enabling the collection, processing and transmission of data wirelessly using Matrix Laboratory (MATLAB) software. Additionally, the microcontroller can be programmed to control other components of the device, such as a display and data storage. To facilitate data display and storage, a dedicated Android software application has been developed for the device, as seen in [Table/Fig-1b]. This software supports wireless connectivity, allowing the user to conveniently view and store the collected data. The entire data processing time, from measurement to display, is completed in less than five minutes. Bite force values are represented as quantitative data, while the muscle action potential is presented graphically, providing a comprehensive visualisation of the recorded muscle activity. The device has been filed for a patent under the Indian Patent Act of 1970, with application number: 202441028693.
Study Procedure
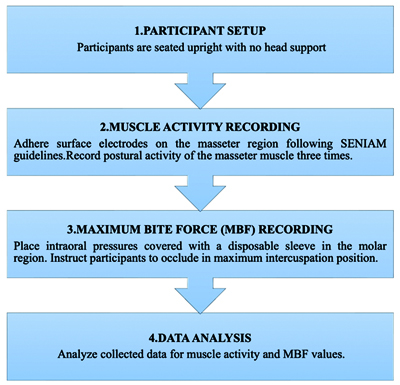
The participants in the study were seated in an upright position with their head unsupported. This positioning ensured that the Frankfort plane was parallel to the floor. To record muscle activity, surface electrodes were placed using adhesive hydrogel foam, following a skin preparation protocol and the guidelines provided by the Standard sEMG for the Non Invasive Assessment of Muscles (SENIAM) [10] on the masseter region. A ground electrode was placed on the side of the neck after applying conduction jelly [Table/Fig-1c]. The participants were instructed to relax completely and the postural activity of the masseter muscle was recorded three times. To measure the MBF, intraoral pressure sensors covered with disposable sleeves were placed intraorally in the right maxillary first molar region. The participants were instructed to occlude in the maximum intercuspation position. Three recordings of the MBF were taken, with a one-minute gap between each recording to prevent muscle fatigue. Similarly, the participants were asked to occlude maximally in the interincisal position and three recordings of the MBF were taken.
Statistical Analysis
The linear data sets were analysed using descriptive statistics. The Pearson’s correlation coefficient (r) was employed to quantify the strength and direction of the linear association between the average bite force values and isometric contraction values. The workflow of the step-by-step process, from participant setup to data collection and analysis, is depicted in [Table/Fig-2].
Workflow-the step by step process from participant set up to data. Collection and analysis.
Results
The right and left molar bite force measurements and EMG of masseter muscle was recorded for study participants. Descriptive statistics was used to evaluate the mean bite force and masseter EMG values. The mean right molar bite force was found to be 525.92 N, while the mean left molar bite force was 570.00 N. The mean incisor bite force was 166.89 N and the mean masseter EMG value was 547.96 N, as shown in [Table/Fig-3].
Bite force and masseter muscle EMG values.
| Descriptive statistics | Right molar bite forceN | Left molar bite forceN | Incisor bite forceN | EMG of masseter forceN |
|---|
| Mean | 525.93 | 570.00 | 166.89 | 547.96 |
| Std. Deviation | 151.98 | 158.66 | 23.04 | 150.075 |
| Median | 450.00 | 500.00 | 160.00 | 483.00 |
| Minimum | 350.00 | 360.00 | 135.00 | 350.00 |
| Maximum | 780.00 | 850.00 | 230.00 | 820.00 |
| Range | 430.00 | 490.00 | 95.00 | 470.00 |
N=Newtons
Pearson’s correlation coefficient test was employed to evaluate the correlation between molar bite force and masseter muscle EMG values. There was a significant positive correlation between right molar bite force and masseter EMG, with a correlation coefficient of r=0.964 (p<0.001). Similarly, a significant positive correlation was found between left molar bite force and masseter EMG (r=0.980, p<0.001) and between incisor bite force and masseter EMG (r=0.550, p=0.002), as presented in [Table/Fig-4].
Correlation between bite force and masseter muscle EMG values.
| Pearson’s correlation coefficient | Right molar bite force(r) | Left molar bite force(r) | Incisor bite force(r) | EMG of masseter force(r) |
|---|
| Right molar bite force(r) | Pearson’s CorrelationSig. (2 tailed)n | 1 | 0.976** | 0.603** | 0.964** |
| <0.0001 | 0.001 | <0.001 |
| Left molar bite force(r) | Pearson’s Correlation Sig. (2 tailed)n | 0.976** | 1 | 0.529** | 0.980** |
| <0.001 | | 0.004 | <0.001 |
| Incisor bite force(r) | Pearson’s CorrelationSig. (2 tailed)n | 0.603** | 0.529** | 1 | 0.550** |
| 0.001 | 0.004 | | 0.002 |
| EMG of masseter force | Pearson’s CorrelationSig. (2 tailed)n | 0.964** | 0.980** | 0.550** | 1 |
| <0.001 | <0.001 | 0.002 | |
Discussion
Occlusal instability is considered one of the most common factors responsible for catastrophic failure [11]. Occlusal bite force and muscle activity are the major determinants affecting harmony in occlusion [12]. Recording bite force is crucial for evaluating the functionality of the masticatory system, as variations in maximum voluntary bite force can indicate various conditions such as acute or chronic pain, Temporomandibular Disorders (TMD) and occlusal disharmony [13]. Hagberg C et al., found a significant linear relationship between bite force and EMG potentials, indicating that elevator muscle activity correlates with the occlusal bite force exerted during functional movements [14]. Gomes SG et al., emphasised a strong positive association between masticatory muscle myoelectric potential and bite force values in electromyographic and bite force studies [15]. Castroflorio T et al., highlighted the use of EMG activity of the surface elevator muscles of the mandible as an indicator for estimating bite forces indirectly [16].
The history of bite force measurement began with Borelli’s gnathodynamometer and has evolved to modern electronic devices like strain-gage transducers and pressure-sensitive foils [17]. Shinogaya T et al., have contributed to this progress by exploring various measurement techniques using devices such as digital dynamometers and deformation-sensitive piezoelectric films [18]. However, it is notable that these studies typically did not incorporate EMG recording alongside bite force measurement. Freeman PW and Lemen CA investigated the relationship between bite force and EMG activity of the masseter muscle in patients with TMD [19]. They found that individuals with TMD exhibited altered bite force and EMG patterns compared to healthy controls, suggesting a potential interdependence between muscle activity and dysfunctional biting patterns. This study emphasised the necessity of considering muscle activity in addition to bite force measurement when evaluating masticatory function in clinical populations. Additionally, a study by Stapelmann H and Türp JC, investigated the relationship between bite force, EMG activity and occlusal contact distribution in individuals with bruxism [20].
Technological advancements have led to the introduction of digital tools that enhance the precision and understanding of bite force and treatment planning. Current devices used to diagnose occlusal instability include Dentoforce 2 (ITLAB, Sollentuna, Sweden), IDDK (Kratos, Cotia, São Paulo, Brazil), FSR No. 151 (Interlink Electronics Inc., Camarillo, CA, United States), Flexiforce (Tekscan, South Boston, MA, United States), GM10 (Nagano Keiki, Japan), MPX 5700 (Motorola, SPS, Austin, TX, United States) and Tekscan Bio EMG (USA) [21].
Despite advancements in existing diagnostic and treatment planning tools, they lack the ability to simultaneously capture muscle activity and bite force values. Muller highlighted the need for a customised integrated system that measures both bite force values and masticatory muscle activity simultaneously, offering comprehensive data for improved diagnosis and treatment planning [22]. An integrated device is considered a powerful tool in the realm of digital prosthetic rehabilitation, enabling a comprehensive evaluation by providing detailed insights into how prosthetic interventions might affect or improve both bite force and the functionality of the masseter muscle.
In the present study, a customised device that integrates a piezoresistive force pressure transducer for recording bite force and a Myoware sensor for recording muscle activity was designed. Song P et al., have stated that piezoresistive sensors boast high sensitivity, fast response time, accuracy, stability and compact size, facilitating widespread adoption in medical applications [23]. They surpass strain gauge transducers by integrating multiple circuits on silicon chips, offering enhanced functionality and ease of production. Sattayasoonthorn P et al., demonstrated the effectiveness of Myoware sensors in capturing muscle EMG signals, highlighting their compact size, ease of use and compatibility with other recording systems [24]. The efficacy of the device used in the study was evaluated through a clinical trial involving 112 healthy volunteers, including men and women aged 21-35 years.
The study yielded measurements of bite force and masseter muscle EMG values. The recorded data included the minimum and maximum values for each variable, with the left molar bite force and masseter muscle action potential exhibiting the highest values, while the right molar bite force demonstrated the lowest values [Table/Fig-3]. The Pearson’s correlation coefficient was used to evaluate the association between bite force and masseter muscle activity. These findings demonstrate significant positive correlations between the variables. Higher molar bite forces were associated with increased masseter muscle EMG activity. A positive correlation between molar bite force and masseter muscle activity was observed for both the right (r=0.964) and left (r=0.980) sides, which were statistically significant at p<0.05 [Table/Fig-3,4]. Similarly, incisor bite forces exhibited a positive correlation with masseter muscle EMG activity (r=0.550), although the correlation coefficient was slightly lower compared to molar bite forces. This aligns with findings from a study by Thongudomporn U et al., utilising a novel bite force measurement device [25].
The findings of the present study agree with those of Christenson LV, who emphasised the direct proportionality between masticatory myoelectric potential and occlusal bite force [26]. Previous studies reported that average bite force values ranged from 200 N to 800 N in healthy adults, with average isometric contraction values of the masseter muscle coinciding with the maximum occlusal bite force of the molar region [27-29]. These values were utilised as standard benchmarks to compare the bite force values and muscle action potential values obtained using the device.
Recently, various innovative bite force measurement devices have been developed, offering promising capabilities for accurate and cost-effective assessment. Lin KR et al., introduced a flexible force sensor array utilising polyimide electrodes and barium titanate-based multilayer ceramic capacitors, demonstrating high sensitivity and linearity under simulated chewing conditions [30]. Lantada D et al., proposed a system that integrates a passive force sensor within an oral splint and an external unit for remote data recording, enabling continuous monitoring without the need for a battery within the mouth [31]. Takahashi M et al., designed a metal-free bite force meter using micro pressure sensors and water-filled bags, ensuring safety in magnetic fields while maintaining accurate force measurement [32]. Umesh S et al., developed a fibre Bragg grating bite force recorder, which translates occlusal force into strain changes sensed by a fibre Bragg grating sensor, offering precise and direct bite force measurement [33]. Fastier-Wooller J et al., introduced a maximum voluntary bite force sensor incorporating polyvinylsiloxane layers and a metal strain gauge, facilitating rapid prototyping and reliable force measurement [34]. Van Vuuren LJ et al., devised a resistance-based bite force sensor composed of martensitic stainless steel plates, providing robustness and accuracy in capturing maximum voluntary bite force [35]. Kurosawa M et al., developed a headset-type wearable device that measures ear canal movements to indirectly estimate bite force, demonstrating a strong correlation between ear sensor values and bite force levels, thereby providing a non invasive alternative for bite force assessment [36]. The efficacy of several novel devices was evaluated and the findings of these studies are summarised in [Table/Fig-5] [31,37-39].
Summary of studies with similar novel devices [31,37-39].
| Year | Author | Title of the study | Study protocol | Results | Limitations |
|---|
| 2012 | Lantada AD et al., [31] | Novel system for bite-force sensing and monitoring based on magnetic near field communication | The study has proposed a novel system that utilised magnetic field communication method, to measure human bite forces in bruxism disorder. A passive sensor was implanted inside the oral cavity and an external reader, facilitated distant data capture. In-vivo trials were conducted to validate the system’s capabilities and advantages compared to existing devices. | The findings suggested that the sensor can continuously monitor force over time, with validate the efficacy of and accuracy, with a communication range of approximately 3 cm, even when operating through human tissue. | While the study successfully demonstrated the feasibility of its system through in-vivo trials, it’s essential to note that the measurement of muscle activity was not evaluated. |
| 2016 | Testa M et al., [37] | A validation study of a new instrument for low-cost bite force measurement | The study evaluated the validity of a simple instrument to measuring bite force with a commercially available sensor in a rubberised housing.The characteristic load-response curves of four different sensors in bare and housed conditions was measured in two consecutives days. | The limited thickness of the developed sensor, the easy repositioning of the device in the mouth and its low cost overcome the most common problems encountered in bite force measuring. Indeed, the housing of the sensor can be assembled by hand and the signal conditioning can be obtained by adopting the hardware recommended by the manufacturer or another equivalent solution. | Sensors operating in the mouth arealso potentially exposed to high humidity, whose effect has not been tested in the present study. Also, the device needs multi-point sensor calibration in the specific load range of the measurement due to non linearity of housed sensors. |
| 2022 | Patil SR et al., [38] | The validate the efficacy of a New device for measuring the maximum bite force | 60 healthy and 60 participants with OSMF were included. The maximum bite force was recorded in alternate order with a bite force sensor (D1) and an occlusal force meter (D2). three tests, with 45-second rest between each recording, was documented for right and left-sides. The reliability was evaluated. | Pearson’s correlation coefficient between two devices revealed a high and significant positive correlation between D1 and D2 separately and in the whole sample.The observations of the present study suggest that the biteforce sensor can be used as a reliable device for measuring bite force. | While the study confirmed the consistency of the newly developed bite force sensor, it overlooked the significance of muscle Electromyographic (EMG) activity as a crucial indicator for assessing maximum bite force. |
| 2023 | Steffen C et al., [39] | Clinical and technical validation of novel bite force measuring device for functional analysis after mandibular reconstruction | The study evaluated the validity of a novel bite force sensor for edentulous patients and also tested the feasibility of the device in a complex intraoral situation. | The results of the present study show that the novel device provides high accuracy and reproducibility and is suitable for bite force measurements in edentulous patients and patients after mandibular reconstruction. | As a limitation, it needs to be stated that the device was built as a prototype and is not generally commercially available yet. Despite low thickness, remaining interferences with occlusion cannot be excluded and comparisons with other devices with different thicknesses need to be performed in the future. Patients with preoperative damage of the mandible, e.g., pathological fractures, incompliance or limited mouth opening, cannot be tested functionally with this device. |
| 2024 | Present study | Validation and analysis of an integrated device for recording bite force and masseter muscle activity in dentate participants: An observational study | The present study aimed to validate the efficacy of an ingeniously designed integrated device that records the occlusal bite force and muscle activity. | The results of the study revealed a strong positive correlation between bite force and muscle activity recorded by the integrated device. The device recorded bite force and muscle activity simultaneously emphasising the dependence on each other in occlusal corrections and rehabilitation. | There are a few limitations associated with the force-resistive sensor. It cannot function effectively under varied thermal conditions, as it is only capable of tolerating average oral temperatures. Participants need adequate mouth opening to utilise this device for recording. |
While numerous studies have explored the reliability of novel bite force recorders, a significant limitation across these devices is the lack of integration with muscle activity recording capabilities, as shown in [Table/Fig-5]. Most devices feature only a force transducer, necessitating the use of separate equipment for recording muscle activity. Nevertheless, Tekscan remains a valuable tool for assessing occlusal forces; however, its limitation lies in its inability to provide a concurrent measurement of muscle activity. The recent Tekscan with the T-Scan™/BioEMG Integration software synchronises the clinical data of T-Scan with the EMG data from BioResearch’s EMG unit, but again, this is an add-on rather than an inbuilt feature, plus it is very expensive and the sensor must be changed often [40]. This fragmentation could complicate data collection and analysis, potentially leading to inconsistencies and inefficiencies in clinical assessments.
The present study offers a significant advancement by integrating bite force recording with muscle activity monitoring in a single device. This integration provides a comprehensive tool for assessing masticatory function, allowing for the simultaneous measurement of both bite force and muscle activity. The device employs machine learning algorithms, utilising neural networks trained to predict a single output value based on the input values of occlusal bite force and muscle activity. This approach can learn the complex patterns in the data and provide a single, integrated value that represents the relationship between the two variables. Both bite force and muscle activity is quantitatively recorded in units of Newtons, offering a precise and comparable dataset. Moreover, the EMG data is presented in a graphical format, facilitating easy interpretation and visualisation of the results, as seen in [Table/Fig-1b].
This integrated approach allows for a comprehensive understanding of the patient’s condition. The obtained data is systematically stored under the patient’s name, enabling effortless comparisons of pretreatment, during-treatment and post-treatment values.
Limitation(s)
However, there are a few limitations associated with the force-resistive sensor. It cannot function effectively under varied thermal conditions, as it is only capable of tolerating average oral temperatures. Additionally, the sensor is not autoclavable, necessitating the use of a disposable protective sleeve. The study was conducted exclusively on healthy volunteers; therefore, its performance should also be tested on individuals with abnormalities or parafunctional habits, especially in cases requiring complex rehabilitation. Furthermore, minor technical errors may occur if there are network issues, resulting in a time lag between signal pickups.
Conclusion(s)
Within the limitations of the study, the following conclusions can be drawn: The customised device, driven by the force pressure transducer and MyoWare sensor, records bite force and muscle action potential simultaneously in Newtons (N). The bite force and muscle action potential values obtained from healthy volunteers showed a high positive correlation, which was statistically significant at p<0.001. Therefore, the ingeniously developed device can serve as an effective chairside diagnostic tool for identifying undesirable occlusal interferences by recording bite force and concurrent muscle action potential during prosthetic rehabilitation procedures.
N=Newtons