Maxillonasal dysplasia, known as Binder’s syndrome, is a rare congenital deformity characterised by distinctive facial features, including a malformed midface and nose, as well as abnormal positions of the nasal bones. In addition, maxillary hypoplasia, or a shorter upper jaw, and nasal abnormalities may manifest as a flattened nose. Many cases of this condition are associated with other malocclusions, and those affected can be easily identified. Individuals with Binder’s syndrome typically present with an undeveloped upper jaw, a projecting lower jaw, a smaller nose, a flat nasal bridge, and midfacial hypoplasia. This is the first case report describing a physiotherapy method for maxillonasal dysplasia. Hereby, the authors present a case report of a six-month-old male child with Binder’s syndrome who exhibited delayed developmental milestones and physical anomalies. The child’s mother had a complicated pregnancy, culminating in an emergency caesarean section due to preterm premature rupture of membranes. The infant, born with Binder’s syndrome and a cleft palate, displayed poor head control, an inability to roll, and reluctance to engage in sensory interactions. Examination revealed bilateral cortical thumbs, hip joint abnormalities, and heightened sensitivity to touch. Magnetic Resonance Imaging (MRI) findings indicated semilobar Holoprosencephaly (HPE) and dysgenesis of the corpus callosum. Physiotherapeutic interventions focused on parent education and home exercise programs targeting developmental milestones. Over the course of two months, the infant showed significant progress in head control and rolling. Furthermore, after four months of training, the child gained sitting control. The present case underscores the importance of early intervention and parental involvement in optimising outcomes for children with Binder’s syndrome.
Case Report
A six-month-old male child presented to the Paediatric Physiotherapy Department with a chief complaint of delayed milestones, including poor head control, a lack of rolling, and difficulty tracking objects with his eyes. The parents reported that the baby had not grown within the normal range for his age, as evidenced by a small head circumference and low weight. The mother also noted tightness in the upper and lower limbs, which was particularly noticeable during dressing and bathing. Compared to his twin sister, the parents observed poor social interaction, such as a lack of eye contact and an aversion to being handled by unfamiliar people, which was indicated by crying.
The twin sister appeared normal at birth and showed no abnormalities upon observation and examination. Her growth and development were uneventful.
The mother was 32 years old at the time of spontaneous conception. She underwent routine ultrasonography examinations every three months and was informed that there were no anomalies in the development of the twins. The trimesters were uneventful, except for slightly elevated Thyroid Stimulating Hormone (TSH) levels at 12 weeks of gestation. At 36 weeks of gestation, she underwent an emergency Lower Segment Caesarean Section (LSCS) due to Preterm Prelabor Rupture of Membranes (PPROM), and the baby was delivered just 10 seconds after his twin sister. He cried at birth, weighed 2.1 kg, had a head circumference of 30 cm, and exhibited a facial abnormality that was subsequently identified as Binder’s Syndrome, along with a cleft palate. The baby was then placed in special care for five days of monitoring and observation before being discharged. He was fed formula through a tube due to poor sucking and rooting reflexes.
The parents noticed that their baby did not hold the head upright while being handled during the initial one to three months. Additionally, they observed that the child did not prefer being touched or having sensory contact with relatives. In the early months, the mother noted mild tightness in both the upper and lower limbs while bathing and dressing the baby, compared to their other child. There was also poor eye contact with the parents and feeding difficulties. The child exhibited abnormal facial features, including an underdeveloped nose and upper lip. Due to the facial deformity, the child experienced trouble breathing. At six months of age, the child underwent cheiloplasty surgery, which aimed to reconstruct the lip, correct the nasal deformity, construct the floor of the nose, and properly align the maxillary segments [Table/Fig-1].
Facial deformity: a) Before surgery, the nose and lips were underdeveloped; b) Postsurgery with nasal stent.

Following the surgery, the parents were advised not to place the baby in a prone position to avoid rubbing the child’s face against the bed, to keep the stitches clean and free of crusting, and to maintain the nasal stent in place. As a result, the child was primarily kept in a supine position, which contributed to sustained developmental delays and the inability to achieve rolling even after 4-5 months.
During the physical examination, the baby showed no abnormal signs related to the cardiopulmonary system. The Paediatrician found no abnormalities in the baby’s cardiopulmonary health. Upon observation in the supine position, a facial deformity [Table/Fig-1], bilateral cortical thumbs, and bilateral abducted and externally rotated hip joints were noted. Random limb-kicking movements were observed, such as pushing and kicking in the upper and lower limbs; however, the elbows were partially flexed during these movements. No tracking of objects was noted. A flat skull and poor hair growth were observed at the back of the skull due to constant pressure resulting from the prolonged supine position.
Primitive reflexes, such as the palmar and plantar reflexes, were present. Curling of the toes was observed when the foot made contact with the floor and even when it was in contact with cloth. An Asymmetric Tonic Neck Reflex (ATNR) with an incomplete pattern was noted. A sensory examination was conducted based on the mother’s input regarding the child’s reactions to different sensory stimuli. It was reported that the baby is hypersensitive to touch and other sensations. However, the infant reacted differently to various stimuli, such as touch, light, and changes in position. The motor examination included Range of Motion (ROM), muscle tone, and reflexes. Passive ROM was measured for all joints using a goniometer. The ranges for all joints were full, but slight resistance was noted. The Modified Ashworth Scale (MAS) was used for all muscle tone assessments [1]. A slight increase in muscle tone was observed in the bilateral upper and lower limbs, indicating grade 1 on the MAS.
The baby was placed in a prone position as part of an assessment for prone position tolerance. Initially, the infant was able to sustain this position for only 10 seconds and did not bear weight on his arms. He made poor attempts to elevate his head off the floor and was able to maintain the position for approximately five seconds without crying.
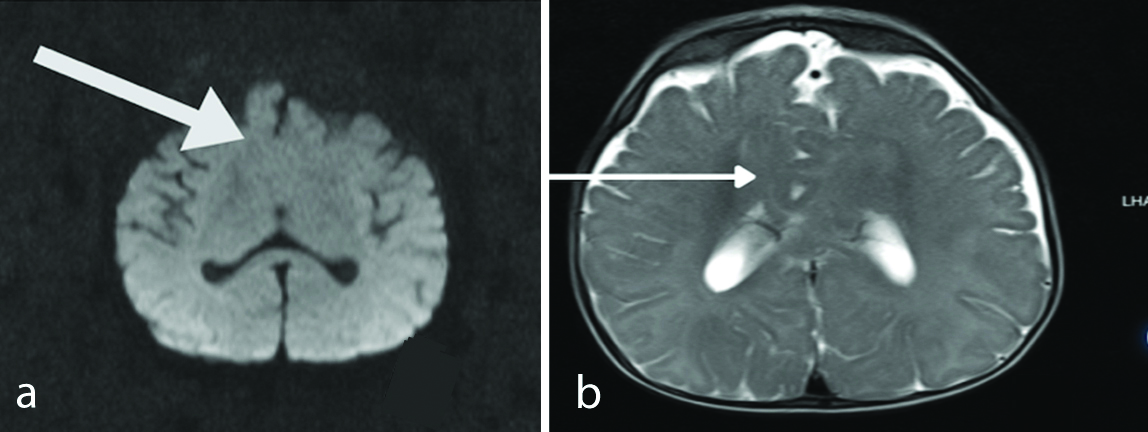
An MRI scan conducted at six months revealed fusion of the anteroinferior aspect of the frontal lobe across the midline. The frontal horns of the lateral ventricles and the septum pellucidum were absent. Additionally, the anterior aspect of the third ventricle was partially obliterated, and there was evidence of dysgenesis of the corpus callosum. The MRI findings were suggestive of semilobar holoprosencephaly [Table/Fig-2a,b].
a) The anteroinferior portion of the frontal lobe is fused in the middle. Dysgenesis of the corpus callosum; b) The third ventricle is partially obliterated.
Physiotherapy goals aimed at improving child developmental milestones were established. The goals set for the first two months of rehabilitation were to achieve head control, upper limb weight acceptance, and trunk dissociation with the lower limb. Once the child attains these goals, the subsequent objectives will focus on improving head and eye movement for tracking objects and facilitating trunk balance for upright sitting.
The rehabilitation process began with parental education. The Physiotherapist explained the diagnosis and its clinical features to both the mother and father. Addressing the parents’ questions and providing insights into the disease and its symptoms gave them a better understanding of the necessity for physiotherapy and the importance of regular visits to the healthcare system. The significance of a home exercise program and the interaction between parents and children for early recovery were also emphasised during this education. The home exercise program aimed to enhance developmental milestones and included positioning, handling the child, and performing exercises a minimum of two times a day for 15-20 minutes. Furthermore, the education focused on helping parents understand the expected outcomes and the dos and don’ts during rehabilitation.
The physiotherapy rehabilitation included tummy time to promote weight-bearing on the hands while in a prone position and to achieve head control. The exercise was performed as follows: the infant was placed on a wedge or an inclined surface, where head control was initiated. Initially, this was done for one minute in three sets, progressing to five minutes in three sets per day.
Secondly, to initiate independent rolling, the infant’s parents were taught the initiation and completion of rolling. The therapist or caregiver would assist by turning the head and body, using stimuli provided by the therapist. For example, the therapist placed a palm on the left-side of the child’s face, and the child’s right hand was abducted above shoulder level to facilitate a smooth roll towards the right-side. The therapist would then slowly turn the face to the right-side, providing the child with a cue for how to turn, usually accompanied by the help of primitive reflexes such as head-on-body righting reactions. This exercise was performed for 2-3 repetitions per set, in three daily sets. An alternative technique for completing the roll involved placing the infant on a wedge, where the initiation of rolling could be assisted by gravity [Table/Fig-3].
Facilitation of rolling on inclined surfaces. Baby kept on an inclined pillow for gravity-assisted rolling.

To train the child to sit, the mother placed him on her lap. This was followed by 5 to 6 minutes of sitting in a chair with support. Another strategy advised to parents is to place the child on a mat and support the child’s trunk using their hands. Initially, support was offered at the axilla, and as the child improved, the hand was lowered to hip level. This adjustment requires increased muscular activation from the child for better sitting control. Later, the child was encouraged to sit by using their hands for support on the floor [Table/Fig-4]. This exercise was performed for 2 to 3 minutes for three sets per day and was later progressed to 5 to 6 minutes for three sets per day.
The child was made to sit by taking support with his hand.

This intervention began in July 2023 when the infant was six months old. The parents continued the home program for two months and maintained contact with the therapist throughout. The infant gained head-holding control for more than 10 minutes, initiated rolling independently, and was able to sit with back support for longer periods. He also sustained himself on his elbows for over 10 minutes and was less irritable in different positions.
Later, at the age of 14 months, the child experienced recurrent fever, which was accompanied by seizures. During this time, the parents were unable to continue the exercises with the child, and as a result, a deterioration in progress was observed. Unfortunately, the child’s condition worsened, and he eventually passed away.
Discussion
Maxillonasal dysplasia, also known as Binder’s Syndrome, is an uncommon congenital deformity initially identified in 1939 by Von Binder [2]. He named it maxillonasal dysplasia since, it is a developmental condition affecting the maxillary anterior area, nasal complex, nose, and jaw [2]. It is characterised by an arhinic face (abnormal position of nasal bones), maxillary hypoplasia, a reduced or non existent nasal bridge, distortion of the nasal bones, hypertrophy of the turbinate with atrophy of the nasal mucosa, and absence of the frontal sinus, though not always. These are Binder’s six classical distinctive traits [3-5]. According to a study by Cossellu G et al., conducted in 2015, Binder syndrome occurs in less than one in every 10,000 live births [6]. Orthodontic or surgical therapy, or a combination of both, may be advised depending on the degree of nasal deformity, malocclusion, and the age of presentation [7,8]. Along with genetic factors [9], there is evidence that vitamin K deficiency [10] in pregnant women can be a cause of Binder syndrome. However, in present case, the mother did not have any such history during her pregnancy.
Binder hypothesised that the abnormality was of archencephalic origin and suggested that there was a disturbance in the prosencephalic induction centre during foetal development. This is indicative of abnormalities in the brain and is further associated with mental retardation [2,11,12].
Holoprosencephaly (HPE) is a brain abnormality caused by incomplete prosencephalon cleavage, which occurs between the 18th and 28th days of gestation and affects both the frontal region and the face. In a previous study, HPE was reported to be associated with Binder’s disease [13]. HPE is expected to occur in 1 in 16,000 newborns [14,15]. Neurological deficits such as developmental delay, mental retardation, hypotonia, spasticity, weakness, epilepsy, and abnormal movements can be observed in HPE. In the present case, the child exhibited delayed development and weakness. Furthermore, the child experienced recurrent seizures and was receiving medication for them.
Craniofacial malformations include microcephaly, hypotelorism or hypertelorism, cleft lip and/or palate, iris coloboma, a flat nose, single maxillary central incisors, hypoplasia of the pyriform aperture, and midline or lateral cleft lip and/or palate. These are clinical findings associated with HPE. Oromotor dysfunction is common in present condition and results in difficulties with eating and swallowing [16]. In present case, the child had no control over head movements and rolling, along with the presence of facial deformities.
The infant’s physiotherapy rehabilitation included tummy time to encourage weight bearing on the hands and to develop head control. To foster independent rolling, the parents were instructed to assist using stimuli. The therapist directed the baby’s head and hand movements to enable smooth rolling, leveraging primitive reflexes. Alternatively, a wedge was used to aid rolling with gravity. Over a two-month period, the child attained fair head control. Furthermore, after four months of training, the child gained sitting control with minimal support.
The parents visited the Department for a review after five months, at which point they were taught about the next milestones, such as quadruped and kneeling activities. Since there are no documented cases of maxillonasal dysplasia and its physiotherapy management, we could not compare it with other rehabilitation strategies. However, the child developed a fever and recurrent seizures in the following month, which hindered progress. Tragically, the child was reported dead by the parents due to respiratory distress in April 2024, at the age of one year and four months.
Conclusion(s)
A multidisciplinary approach to present rare disorder may lead to improvements in developmental milestones. Parents’ education and involvement will be essential parts of this process. However, frequent illnesses have hindered progress.
[1]. Meseguer-Henarejos AB, Sánchez-Meca J, López-Pina JA, Carles-Hernández R, Inter- and intra-rater reliability of the Modified Ashworth Scale: A systematic review and meta-analysisEur J Phys Rehabil Med 2018 54(4):576-90.Epub 2017 Sep 1310.23736/S1973-9087.17.04796-728901119 [Google Scholar] [CrossRef] [PubMed]
[2]. Madiyal A, Babu S, Ajila V, Castelino RL, Rao K, Madi M, Binder’s Syndrome-An unusual craniofacial anomalyJournal of Dentistry Indonesia [Internet] 2018 [cited 2024 May 26] 25(1):69-72. [Google Scholar]
[3]. Olow-Nordenram M, Thilander B, The craniofacial morphology in individuals with maxillonasal dysplasia (Binder’s syndrome). A longitudinal cephalometric study of orthodontically untreated childrenEur J Orthod [Internet] 1987 [cited 2024 Jul 28] 9(3):224-36. [Google Scholar]
[4]. Quarrell OW, Koch M, Hughes HE, Maxillonasal dysplasia (Binder’s syndrome)J Med Genet [Internet] 1990 [cited 2024 Jul 28] 27(6):384-87. [Google Scholar]
[5]. Nedev PK, The Binder syndrome: Review of the literature and case reportInt J Pediatr Otorhinolaryngol 2008 72(10):1573-76. [Google Scholar]
[6]. Cossellu G, Biagi R, Faggioni G, Farronato G, Orthodontic treatment of binder syndrome: A case report with 5 years of follow-upCleft Palate Craniofac J [Internet] 2015 [cited 2024 May 26] 52(4):484-88. [Google Scholar]
[7]. Holmström H, Clinical and pathologic features of maxillonasal dysplasia (Binder’s syndrome): Significance of the prenasal fossa on etiologyPlast Reconstr Surg 1986 78(5):559-67.10.1097/00006534-198611000-000013763743 [Google Scholar] [CrossRef] [PubMed]
[8]. Horswell BB, Holmes AD, Barnett JS, Levant BA, Maxillonasal dysplasia (Binder’s syndrome): A critical review and case studyJ Oral Maxillofac Surg 1987 45(2):114-22.10.1016/0278-2391(87)90401-03468213 [Google Scholar] [CrossRef] [PubMed]
[9]. Mazzone E, Cos Sanchez T, Persico N, Cannie MM, Jani J, Binder syndrome: A phenotype rather than a definitive diagnosis?Ultrasound Obstet Gynecol 2019 53(1):131-32.10.1002/uog.1919830084160 [Google Scholar] [CrossRef] [PubMed]
[10]. Howe AM, Webster WS, Lipson AH, Halliday JL, Sheffield LJ, Binder’s syndrome due to prenatal vitamin K deficiency: A theory of pathogenesisAust Dent J [Internet] 1992 [cited 2024 Jul 18] 37(6):453-60. [Google Scholar]
[11]. Cuillier F, Cartault F, Lemaire P, Alessandri JL, Maxillo-nasal dysplasia (Binder Syndrome): Antenatal discovery and implicationsFetal Diagn Ther 2005 20(4):301-05. [Google Scholar]
[12]. Mehrotra R, Srivastava P, Katiyar A, Binder’s syndrome: A case reportIndian J Otolaryngol Head Neck Surg 2019 71(Suppl 3):1757-61.Epub 2017 Feb 8. PMCID: PMC684830110.1007/s12070-017-1100-y31763239 [Google Scholar] [CrossRef] [PubMed]
[13]. Keppler-Noreuil KM, Wenzel TJ, Binder phenotype: Associated findings and etiologic mechanismsJ Craniofac Surg 2010 21(5):1339-45.10.1097/SCS.0b013e3181ef2b7120818242 [Google Scholar] [CrossRef] [PubMed]
[14]. Dubourg C, Bendavid C, Pasquier L, Henry C, Odent S, David V, HoloprosencephalyOrphanet J Rare Dis [Internet] 2007 [cited 2024 May 26] 2(1):01-14. [Google Scholar]
[15]. Raam MS, Solomon BD, Muenke M, Holoprosencephaly: A guide to diagnosis and clinical managementIndian Pediatr [Internet] 2011 [cited 2024 May 26] 48(6):457-66. [Google Scholar]
[16]. Blaas HG, Eriksson AG, Salvesen KA, Isaksen CV, Christensen B, Møllerløkken G, Brains and faces in holoprosencephaly: Pre- and postnatal description of 30 casesUltrasound Obstet Gynecol 2002 19(1):24-38.10.1046/j.0960-7692.2001.00154.x11851965 [Google Scholar] [CrossRef] [PubMed]